Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
Cardiovascular variations are very common and often without consequences for the individual. One could expect that variationsin larger vessels such as the translocation of the subclavian artery result in some kind of symptoms, but it is often only foundincidentally during unrelated medical examinations not related to it or during anatomical dissections in educational settings.Here we present two cases of a translocated right subclavian artery, which is commonly called aberrant right subclavianartery or arteria lusoria. Both donors lived their entire lives with the condition remaining undiagnosed before the dissectionduring a medical anatomy course setting. We describe the course of the artery and associated other anomalies as found in thedonors and discuss the developmental causes of the observed variations. Additionally, we point out why a thorough evaluationof any patient is important before operations in the neck or thoracic cavity given the potential presence of an aberrant rightsubclavian artery.
Abbreviations
PAAs: Paired Pharyngeal Arch Arteries; ASAs: Aberrant Subclavian Arteries; ALSA: Aberrant Left Subclavian Artery; ARSA: Aberrant Right Subclavian Artery; NRLN: Non- recurrent Laryngeal Nerve; ORRC: Office of Regulatory Research Compliances; AFib: Atrial fibrillation; MRI: Magnetic resonance imaging; TEVAR: Thoracic Endovascular Aortic Repair.
Introduction
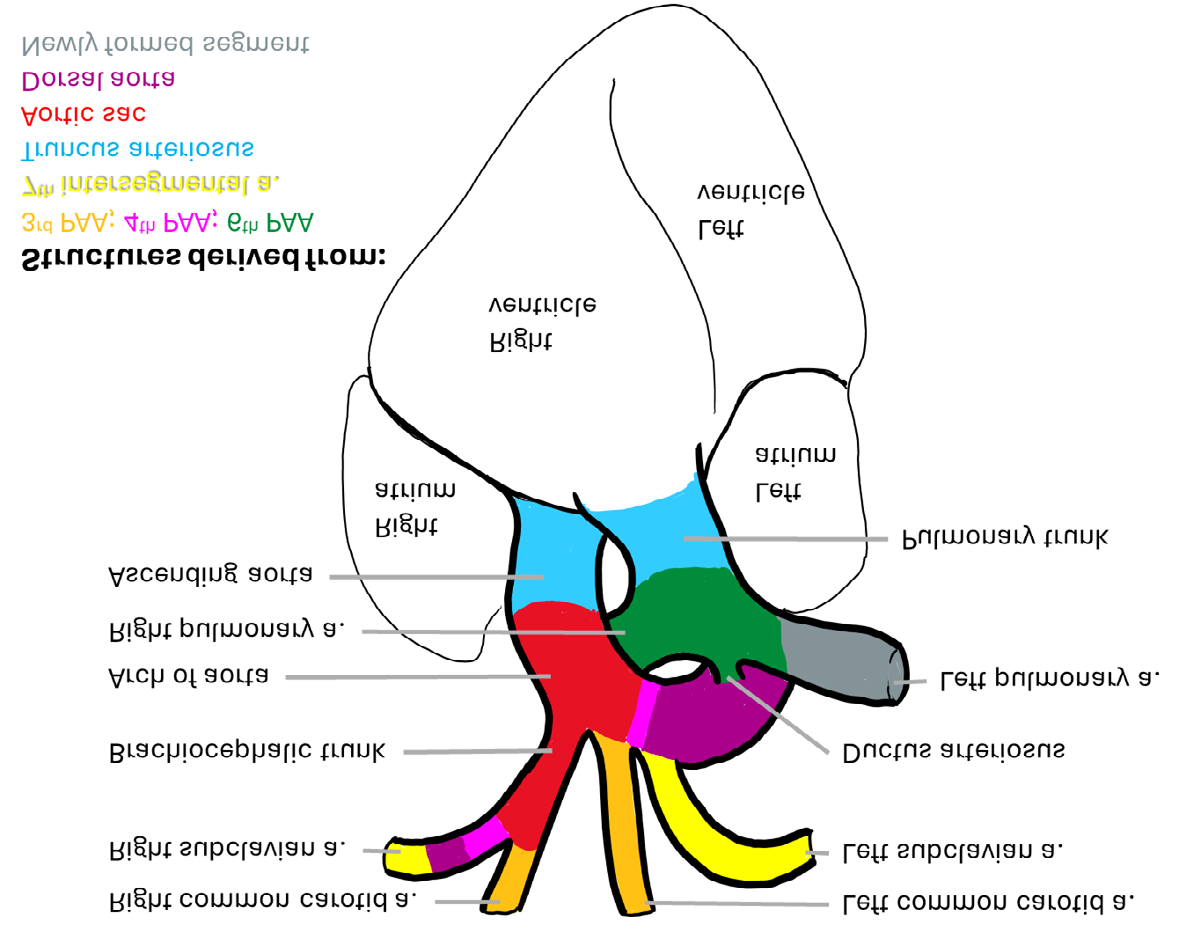
Taking all congenital anomalies together, heart anomalies are the most common birth defects [1]. Several congenital heart anomalies, such as ventricular septal defects, require surgery sooner or later. Other anomalies, such as atrial septal defects or displacements of arteries or veins, are often unrecognized or are only discovered in adulthood [2]. The aortic arch and its main branches are known to have regular variations and abnormalities [3, 4]. In mammals, including humans, the aortic arch most commonly has three branches [5], which are from right to left: brachiocephalic trunk, left common carotid artery, and left subclavian artery (Figure 1). The right common carotid artery and right subclavian artery arise from the brachiocephalic trunk. Any deviations from this pattern are caused by developmental changes or disturbances.
In humans, the aorta development begins with the fusion of angiogenic cell clusters during the third gestational week while the endocardial tube is formed in parallel through lateral folding processes of the embryo. The endocardial tube is closed by day 21 [6]. The primitive aorta includes dorsal and ventral segments which connect through the first aortic arch, also known as the first or mandibular arch artery. The paired ventral aortae limbs fuse to form the aortic sac [7]. During the fourth week, the dorsal aortae fuse from spinal levels T4 to L4, thereby forming the descending aorta passing through the thorax and abdomen.
Rostrally, where the dorsal aortae are not fused, there are five paired pharyngeal arch arteries (PAAs), also called aortic arch arteries, that develop from anterior to posterior between the dorsal and ventral aortae. These arteries are numbered 1-6; however, number 5 is not formed in the mammalian embryonic development. Caudal to these arteries emerge intersegmental arteries from the fused dorsal aorta. The PAAs are remodelled during development and give rise to the arteries of the head, neck, and upper extremity (Figure 1) [8, 9]. Specifically, the first and second PAAs regress and their remnants are the maxillary arteries and stapedial arteries, respectively. The third PAAs differentiate into the common carotid arteries and the beginning of the internal carotid arteries. The fourth and sixth PAAs follow an asymmetrical developmental pattern. The left fourth PAA is integrated into the aortic arch. The proximal right fourth PAA forms the proximal part of the right subclavian artery arising from the brachiocephalic trunk, which itself is a remnant of the aortic sac. The distal part of the fourth PAA remains in contact with a remnant of the right dorsal aorta. The right seventh intersegmental artery enlarges, forming the distal portions of the right subclavian artery. The left seventh intersegmental artery differentiates into the left subclavian artery. The sixth pharyngeal arch artery forms the distal part of the pulmonary trunk and the pulmonary arteries. The left sixth pharyngeal arch artery additionally gives rise to the ductus arteriosus.
Important for the current case report is that during normal development the right subclavian artery arises from three structures: the proximal portion from the fourth PAA, and the distal portion from both the right dorsal aorta, and the right seventh intersegmental artery (Figure 1). The left subclavian artery, however, forms entirely from the left seventh intersegmental artery.
During the reorganization of the PAAs, it is common to observe minor or major variations or anomalies. Some aortic arch anomalies may present as clinically complex cases with elusive etiologies due to their rarity (e.g., see Hanneman, et al. [3]). Aberrant subclavian arteries (ASAs) occur in up to 3% of the normal population and are usually asymptomatic [10]. When symptoms do occur, they are often related to secondary compression of the trachea or the esophagus [11]. The occasional occurrence of an aberrant left subclavian artery (ALSA) is also reported [12].
An aberrant right subclavian artery (ARSA) or arteria lusoria is the most common variation of the typical pattern [13, 14, 15]. Developmentally, ARSA results from the involution of both the right fourth PAAs and the proximal portion of the right dorsal aorta, coupled with persistence of the right seventh intersegmental artery [16]. This causes the translocation of the right subclavian artery to the far left [17], resulting in an aortic arch with four main branches from right to left: right common carotid, left common carotid, left subclavian, and right subclavian. The ARSA then needs to extend from left to the right arm, thereby passing the midline.
An ARSA was first recorded by the French anatomist Hunauld [18]. The term arteria lusoria is derived from Bayford [19], who described ‘dysphagia lusoria’ as a syndrome caused by this vascular anomaly. There are variations in the course of the ARSA, which can be retroesophageal, inter-tracheo- esophageal, and antetracheal in 80%, 15%, and 5% of cases, respectively [20, 21]. In rare instances, this atypical branching and the changed course of the ARSA can prevent timely and accurate diagnoses and surgical treatments [22]. Clinical presentation of ARSA varies from having no symptoms (most common) to having complications and symptoms including cough [23], dysphagia [17, 24], hoarseness, dyspnoea and back or chest pain [25, 26]. Only 5% of adult patients with this ARSA reported symptoms [22]. Occasional associated with ARSA are arterial-esophageal fistula [27] and/or an aneurysmal degeneration of the aorta at the orifice of ARSA, which is also called diverticula lusoria or Kommerell’s diverticulum [23, 28, 29].
Previous studies proposed a classification system for ASAs that takes into account the location, size, and clinical significance of the anomaly [28, 30]. The proposed system by Plotkin, et al. [28] includes four categories: type 1 – ARSA arises from the aortic arch distal to the left common carotid artery; type 2 – ARSA arises from the descending aorta along with a common carotid trunk (giving rise to both right and left common carotid arteries); type 3 – ALSA arises on the right side of the aortic arch; and type 4 – ALSA arises on the right with the common carotid trunk. Plotkin, et al. [28] also emphasizes the importance of identifying ASAs during preoperative planning for aortic surgery to avoid complications. Others have proposed alternative classifications with more extensive criteria [30]. Most commonly, the ARSA is the only abnormality of the aortic arch but occasionally patients with ASRA and coarctation, right- sided aortic arch, or even complete aortic arch interruptions were reported [22].
The vagus nerve (cranial nerve X) extends from the brain, through the neck and thorax, to the upper gastrointestinal tract. After passing into the thorax the vagus nerve usually gives off a branch that returns into the neck to innervate laryngeal muscles and is therefore called the recurrent laryngeal nerve. During embryological development the recurrent laryngeal nerve arises originally below the level of the sixth PAAs and crosses under the sixth arches to innervate intrinsic muscles of the larynx. However, during the remodelling of the PAAs the left recurrent laryngeal nerve becomes caught under sixth arch (ductus arteriosus) and can then be found returning under the aortic arch. The right recurrent laryngeal nerve becomes caught under the right fourth PAA as the distal sixth PAA disappears [31]. In the case of an ARSA, the right recurrent laryngeal nerve does not get caught under the fourth PAA and directly passes from the vagus nerve to the laryngeal muscles without forming the typical loop. A non-recurrent laryngeal nerve (NRLN) is found in most ARSAs [32].
For the purposes of this case presentation, we will be using the Plotkin, et al. [28] classification criteria. Here, we describe two cadaveric cases of Type 1 retroesophageal- placed ARSA with concurrent presence of a NRLN on the right side. Both anomalies will be discussed in light of their clinical implications.
Materials & Methods
The whole-body donors with the here described anomalies were part of the Howard University's Donor Program, housed in the Department of Anatomy, Howard University, Washington, DC, USA. This project was reviewed by the Office of Regulatory Research Compliances (ORRC) of Howard University and ruled exempt (IRB-2023-0997; FWA00000891). Both donors were caucasian females in their early 90s and died from renal cancer (donor 1) and hemorrhagic shock (donor 2). Donor 2 had other chronic conditions, including Atrial fibrillation (AFib) and kidney disease. The initial dissection (opening thorax and pericardium, removal of heart) was performed by first year medical students. Upon recognition of the unusual patterning of the aortic arch branches, further dissection of the anomalous branches, along with the associated nerve variations, was performed. The progress was then photographed using a Nikon D5300 camera (24.2 MP, with 18-55mm f/3.5-5.6G ED VR Auto Focus-S DX NIKKOR Zoom Lens).
Results
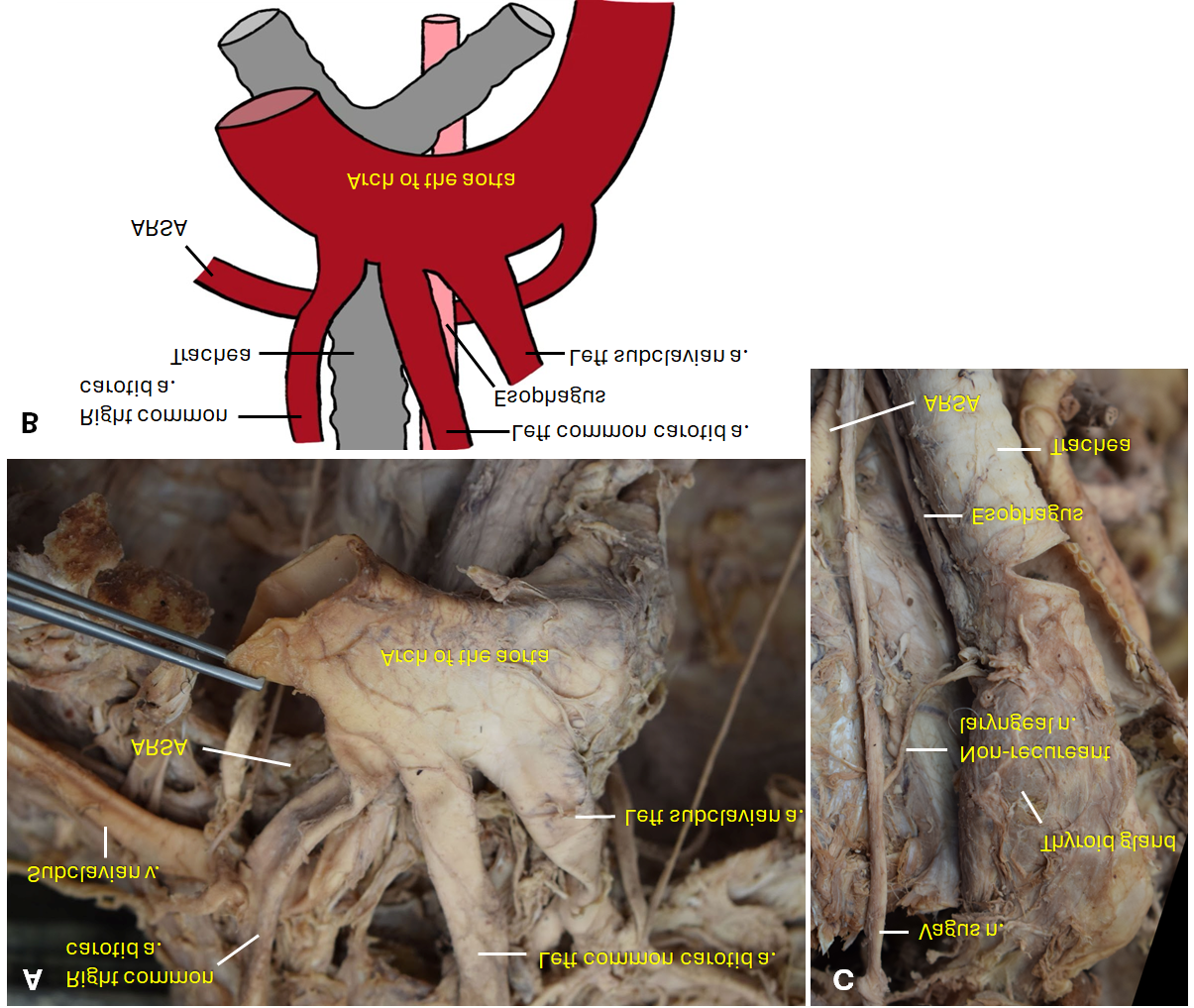
During routine dissections of the heart and associated larger vessels, two female human body donors were found to exhibit ARSAs. In both donors the ARSA extended retro- esophageal and the brachiocephalic trunk was absent (Figure 2a, 2b). In addition to the ARSA, Donor 1 had an associated NRLN anomaly (Figure 2C). The laryngeal components of Donor 2 were removed before we could check on their anatomy.
In both donors, the ARSAs and the left subclavian arteries, had the typical associated branching from medial to lateral: vertebral artery, thyrocervical trunk, internal thoracic artery, and the dorsal scapular artery. Typically, the thyrocervical trunk arises from the first part of the subclavian artery, which was also the case in the left subclavian arteries. However, the right thyrocervical trunk originated from the ARSA. Both thyrocervical trunks had a normal branching pattern giving rise to four branches: inferior thyroid artery, suprascapular artery, ascending cervical artery, and transverse cervical artery.
Investigation of the external and internal features of the heart found no anomalies in structures or arteriovenous vessels (atrial septum or ventricular septum, coronary arteries, interventricular arteries, or great vessels).
Discussion
Identification of the presence of an ARSA is clinically important to practitioners, as their appearance may cause surgical complications during unrelated procedures. Furthermore, it is essential to diagnose and treat symptoms caused by ARSA. While most patients with ARSA seem to be asymptomatic, others might need surgical intervention in the case of prolonged symptomatology. Our case presentation, detailing the presence of ARSAs in two caucasian, female human body donors with concurrent NRLN anomalies, contributes to the existing literature on congenital vascular anomalies. Neither donor was known to have an ARSA before the dissection, indicating that the prevalence of ARSA could be higher than the 0.3%-3% found in literature [10]. The identification of ARSAs during routine dissection underscores the importance of thorough anatomical exploration, as these anomalies, though rare, can have significant clinical implications and less significant but still impactful implications for anatomical education.
Our findings align with the previously described characteristics of ARSA, that is its origin from the left side of the aortic arch, occurring in a minority (0.5% to 1.8%) of the general population [17]. There seems to be a higher prevalence of ASA in females (58%) than in males (42%) [22]. This is also presented when looking only at ARSA, where females make up about 55.3% of cases whereas 44.7% are males [10]. However, a comprehensive review on ASAs with surgical interventions resulted in identifying 732 patients with ASA or an aortic pathology with ASA, where 60.1% (440) were males [33]. The prevalence of ARSA in Trisomy 21 individuals is 19% to 36% while prevalence in the general population is just 0.2% to 13.3% [34]. In fact, detection of an ARSA in first trimester ultrasounds is a soft marker that can be used in the diagnosis of trisomy 21 [35].
In children and adults, ASAs can be identified with aortic arch angiographies, performed through catheterization of the right femoral artery. This procedure appears to be the standard to diagnose ASA [11, 36, 37]. Additionally, a CT can demonstrate the course of a blood vessel that causes an esophageal impression [36]. Magnetic resonance imaging (MRI) can be used to evaluate the vasculature including the branching from the aortic arch. Lastly, endoscopic ultrasonography was successfully used to identify ARSAs [38]. The presence of NRLNs on the right side further adds to the complexity of these anatomical variations. Although the NRLN is an asymptomatic variant of the recurrent laryngeal nerve, there are complications that can arise, especially during neck operations, including thyroid surgical injury, which often leads to temporary or permanent paralysis of the vocal cord [39]. In cases where the NRLN is undetected, there is a six-fold increase in surgically related nerve injury. Thus, an increased understanding of NRLN is vital in reducing intraoperative complications associated with its occurrence [39].
Besides the occurrence of NRLN, ARSA is usually the only abnormality of the aortic arch; however, some patients occasionally may also present with coarctation, right-sided aortic arch, or even complete aortic arch interruptions [22]. In cases where ARSA requires surgical intervention the survival rate is relatively high independent of the surgical technique used [33]. Most commonly open surgery [40, 41] and thoracic endovascular aortic repair (TEVAR) [42, 43, 44, 45] are implemented in these treatments.
Conclusion
Comparing our results with the existing literature, we provide two more cases highlighting the potential asymptomatic nature of ARSAs, the diagnostic modalities for living adults and fetuses, and the associated complications, such as dysphagia lusoria. Additionally, we underscore the importance of recognizing ARSAs in preoperative planning for aortic surgeries and the potential gender differences and genetic associations. The coexistence of NRLNs in our donors emphasizes the need for heightened awareness during surgical interventions in the anterior neck to minimize the risk of iatrogenic injuries. Identification and diagnosis of symptoms caused by ARSA are clinically important to practitioners, as their appearance may present surgical complications during unrelated surgeries, or necessitate surgical intervention in the case of prolonged symptomology by someone familiar with ARSA. Overall, our case study expands the understanding of ARSAs and associated anomalies, providing valuable insights for anatomical education, clinical practice, and future research endeavors.
Acknowledgments
The authors wish to thank Dr. Jordy Salcedo-Girlado for his Figure 2. drawing. This work was made possible through institutional support from the Anatomy Department at Howard University College of Medicine.
References
-
Hoffman JL, Kaplan S (2002) The incidence of congenital heart disease. Journal of the American College of Cardiology 39(12): 1890-1900.
-
Romfh A, Pluchinotta FR, Porayette P, Valente AM, Sanders SP (2012) Congenital Heart Defects in Adults: A Field Guide for Cardiologists. Journal of Clinical & Experimental Cardiology 15(Suppl 8): 007.
-
Hanneman K, Newman B, Chan F (2017) Congenital variants and anomalies of the aortic arch. Radiographics 37(1): 32-51.
-
Priya S, Thomas R, Nagpal P, Sharma A, Steigner M (2018) Congenital anomalies of the aortic arch. Cardiovascular Diagnosis and Therapy 8(Suppl 1): S26.
-
Parsons FG (1902) On the arrangement of the branches of the mammalian aortic arch. Journal of Anatomy and Physiology 36(Pt 4): 389.
-
Schleich J (2002) Images in Cardiology. Development of the Human Heart: Days 15–21. Heart 87(5): 487.
-
Sadler TW (2010) Langman’s Medical Embryology. (Ed.), Wolters Kluwer Health/Lippincott Williams & Wilkins, Philadelphia.
-
Effmann EL, Rieger R, Boyadjiev SA, et al. (1986) Mechanisms of Pharyngeal Arch Artery Remodeling. American Journal of Medical Genetics 24(2): 157-169.
-
Mocarska A, Szylejko M, Staroslawska E, Burdan F (2014) An unusual origin of the right subclavian artery– arteria lusoria. Current Issues in Pharmacy and Medical Sciences 27(4): 234-236.
-
Polguj M, Chrzanowski Ł, Kasprzak JD, Stefańczyk L, Topol M, et al. (2014) The aberrant right subclavian artery (arteria lusoria): the morphological and clinical aspects of one of the most important variations--a systematic study of 141 reports. The Scientific World Journal 2014: 292734.
-
Klin B, Tauber Z, Peer A, Broide E, Vinograd I, et al. (1996) Dysphagia lusoria in children. European Journal of Vascular and Endovascular Surgery 11(4): 504-506.
-
Salanitri J (2005) MR angiography of aberrant left subclavian artery arising from right-sided thoracic aortic arch. The British Journal of Radiology 78(934): 961-966.
-
Gomes MMR, Bernatz PE, Forth RJ (1968) Arteriosclerotic aneurysm of an aberrant right subclavian artery. Diseases of the Chest 54(6): 549-552.
-
Pome G, Vitali E, Mantovani A, Panzeri E (1987) Surgical treatment of the aberrant retroesophageal right subclavian artery in adults (dysphagia lusoria). Report of two new cases and review of the literature. The Journal of Cardiovascular Surgery 28(4): 405-412.
-
Turkenburg JL, Versteegh MIM, Shaw PC (1994) Case report: aneurysm of an aberrant right subclavian artery diagnosed with MR imaging. Clinical Radiology 49(11): 837-839.
-
Inami T, Seino Y, Mizuno K (2013) Unique case of giant Kommerell diverticulum with aberrant left subclavian artery arising from the left aortic arch associated with situs inversus. International Journal of Cardiology 163(3): e47-e48.
-
Saraceni C, Kwan WC, Joshi TV, Spera MA, Landreneau SW (2018) Aberrant Right Subclavian Artery: A Rare Cause of Dysphagia: 1720. American Journal of Gastroenterology 113(2018): S982-S983.
-
Hunauld F (1735) Examination of some parts of a monkey. History of the Royal Academy of Sciences 2: 516
-
Bayford D (1794) Account of singular case of obstructive deglutition. Mem Medical Society London 2: 271-282
-
Domínguez R, Corredera L (2009) Aberrant right subclavian artery (Arteria lusoria): Report of three cases, one with a bicarotid trunk. European Journal of Anatomy 13(1): 43-46.
-
Naqvi SEH, Beg MH, Thingam SKS, Ali E (2017) Aberrant right subclavian artery presenting as tracheoesophagial fistula in a 50-year-old lady: Case report of a rare presentation of a common arch anomaly. Annals of Pediatric Cardiology 10(2): 190-193.
-
Molz G, Burri B (1978) Aberrant subclavian artery (arteria lusoria): sex differences in the prevalence of various forms of the malformation. Evaluation of 1378 observations. Virchows Archiv. A, Pathological Anatomy and Histology 380(4): 303-315.
-
Cinà CS, Althani H, Pasenau J, Abouzahr L (2004) Kommerell’s diverticulum and right-sided aortic arch: a cohort study and literature review. Journal of Vascular Surgery 37(3): 588-593.
-
Chan S, Fermanis G (2023) Translocation of aberrant right subclavian artery to the ascending aorta—a treatment for dysphagia lusoria. Journal of Surgical Case Reports 2023(2): rjad054.
-
Edwards JE (1948) Anomalies of the derivatives of the aortic arch system. Medical Clinics of North America 32(4): 925-949.
-
Kieffer E, Bahnini A, Koskas F (1994) Aberrant subclavian artery: surgical treatment in thirty-three adult patients. Journal of Vascular Surgery 19(1): 100-111.
-
Peress S, Tuqan W, Thomas A (2021) Upper Gastrointestinal Bleeding from Aberrant Right Subclavian Artery-Esophageal Fistula. The Ochsner Journal 21(4): 406-412.
-
Plotkin A, Ng B, Han SM, Weaver FA, Ham SW, et al A. (2020) Association of aberrant subclavian arteries with aortic pathology and proposed classification system. Journal of Vascular Surgery 72(5): 1534-1543.
-
Bath D’Oria M, Rogers RT, Colglazier JJ, Braet DJ, Coleman DM, et al. (2023) Contemporary Outcomes after Treatment of Aberrant Subclavian Artery and Kommerell’s Diverticulum. Journal of Vascular Surgery 77(5): 1339-1348.
-
Vučurević G, Marinković S, Puškaš L, Kovačević I, Tanaskovic S, et al. (2013) Anatomy and radiology of the variations of aortic arch branches in 1,266 patients. Folia Morphologica 72(2): 113-122.
-
Allen E, Minutello K, Murcek BW (2017) Anatomy, Head and Neck, Larynx Recurrent Laryngeal Nerve. StatPearls [Internet].
-
Avisse C, Marcus C, Delattre JF, Marcus C, Cailliez-Tomasi JP, et al. (1998) Right nonrecurrent inferior laryngeal nerve and arteria lusoria: the diagnostic and therapeutic implications of an anatomic anomaly: Review of 17 cases. Surgical and Radiologic Anatomy 20: 227-232.
-
Konstantinou N, Antonopoulos CN, Tzanis K, Kölbel T, Peterß S, et al. (2022) Systematic review and meta- analysis of outcomes after operative treatment of aberrant subclavian artery pathologies and suggested reporting items. European Journal of Vascular and Endovascular Surgery 63(5): 759-767.
-
Polednak AP (2017) Prevalence of the aberrant right subclavian artery reported in a published systematic review of cadaveric studies: the impact of an outlier. Clinical Anatomy 30(8): 1024-1028.
-
Martínez-Payo C, Suanzes E, Gómez-Manrique A, Arranz A, Pérez-Medina T (2022) Aberrant right subclavian artery as soft marker in the diagnosis of trisomy 21 during the first trimester of pregnancy. Archives of Gynecology and Obstetrics 305(6): 1439-1444.
-
Maier W (1981) Dysphagia lusoria: anomalous origin of the right subclavian artery. Demonstration by computed tomography. European Journal of Radiology 1(3): 229- 231.
-
Harms J, Vogel T, Ennker J, Felix R, Hetzer R (1994) Diagnostic evaluation and surgical management of the aberrant right subclavian artery. Bildgebung= Imaging 61(4): 299-303.
-
De Luca L, Bergman JJ, Tytgat GNJ (2000) EUS imaging of the arteria lusoria: case series and review. Gastrointestinal Endoscopy 52(5): 670-673.
-
Henry BM, Sanna S, Graves MJ, Vikse J, Sanna B, et al. (2017) The Non-Recurrent Laryngeal Nerve: a meta- analysis and clinical considerations. Peer J 5: e3012.
-
Ota T, Okada K, Takanashi S, Yamamoto S, Okita Y (2006) Surgical treatment for Kommerell’s diverticulum. The Journal of Thoracic and Cardiovascular Surgery 131(3): 574-578.
-
Ikeno Y, Koda Y, Yokawa K, Gotake Y, Henmi S, et al. (2019) Graft replacement of Kommerell diverticulum and in situ aberrant subclavian artery reconstruction. The Annals of Thoracic Surgery 107(3): 770-779.
-
Matsumura JS, Lee WA, Mitchell RS, Farber MA, Murad MH, et al. (2009) The Society for Vascular Surgery Practice Guidelines: management of the left subclavian artery with thoracic endovascular aortic repair. Journal of Vascular Surgery 50(5): 1155-1158.
-
Alghamdi MA, Al-Eitan LN, Elsy B, Abdalla AM, Mohammed HM, et al. (2021) Aberrant right subclavian artery in a cadaver: a case report of an aortic arch anomaly. Folia Morphologica 80(3): 726-729.
-
Forde R, Williams EW (2016) The Non-recurrent Laryngeal Nerve -- A Rare Phenomenon Which Requires Vigilance. The West Indian Medical Journal 64(3): 303- 304.
-
Myers PO, Fasel JH, Kalangos A, Gailloud P (2010) Arteria lusoria: developmental anatomy, clinical, radiological and surgical aspects. Annals of Cardiology and Angiology 59(3): 147-154.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat
- Communicating Neuroanatomical Fibers in Health and Diseases