Parvo B19 and Anaemia: The Various Profiles – A Mini Review
Introduction: Parvovirus 19 (Parvo B19) is a single stranded DNA virus which predominantly affects school-aged children, parents of such children and adults who are working in day care centres or schools. Individuals with underlying haemoglobinopathies, haemophilia, immunocompromised, malignancy and pregnancy states are at a higher risk of infection. This virus has been associated with multiple clinical manifestations including erythema infectiosum, arthopathy, fetal cardiomyopathy and hydrops fetalis. However, one of the most significant complications is the anaemia caused in the adult population. This includes pure red cell aplasia and transient aplastic crisis (TAC). Review: Pure red cell aplasia occurs predominantly in patients with immunocompromised states. The aplasia characteristically presents with a chronic or recurrent severe normocytic normochromic anaemia with reticulocytopaenia. The bone marrow reveals an absence of red-cell precursors or with the presence of giant pro-normoblasts with intra-nuclear inclusions. The condition is effectively managed using packed red cell transfusions, based on the degree of anaemia, and with intravenous immunoglobulin at 1g/kg over a period of 2 days or, more preferably, 500mg/kg over 5 days. The majority of patients respond after 1-3 doses. Correction of the underlying patient risk factors is vital. TAC occurs more frequently in patients with underlying red-cell abnormalities. This presents with a one to two week severe anaemia with variable smear and cellular findings varying from microcytic hypochromic to normocytic normochromic. Additionally, there is a reduced reticulocyte percentage and index. Packed red cell transfusion and correction of the underlying risk factor are often sufficient for the management of anaemia. The addition of immunoglobulin administration, 500mg/kg over 5 days, may be needed for patients who are immunocompromised. Conclusion: Parvovirus B19 remains a prevalent and prominent virus associated with multiple medical conditions particularly in immunocompromised states such as that of HIV, as well as erythrocyte disorders. Clinically, the virus has a plethora of presentations, two of which are severe anaemias: transient aplastic crisis and pure red cell aplasia. These conditions may be effectively and successfully managed with intravenous packed red-cell transfusions, intravenous immunoglobulins and by addressing of the underlying patient risk factors.
Introduction
Parvovirus B19 (Parvo B19) is a single stranded DNA virus of the Erythoparvovirus genus in the Parvoviridae family, with Genotype 3 being the most common sub-strain in Sub-Saharan Africa, and Genotype 1, being the most common sub-strain in Europe and the United States [1, 2]. Within the South African context this human obligate virus is known to have a prevalence varying from approximately 3% in pregnant women to approximately 18% in HIV positive non- suppressed patients [3, 4]. The virus predominantly affects children aged 5–15 years, as well as adult parents of such children in that given age group. Additionally, adults who are working in day care centres or schools, are also at high risk of transmission [5]. Parvo B19 predominantly spreads via respiratory droplets, but may also spread haematogenously in patients who receive blood products or organs. The virus is known to favour individuals with underlying haemoglobinopathies, haemophilia, immunocompromised states, malignancy and pregnancy [4, 5, 6].
Parvo B19 has been associated with erythema infectiosum, arthopathy, fetal cardiomyopathy and hydrops fetalis. However, one of the most significant complications of the virus is the anaemia caused. This is largely limited to pure red cell aplasia and transient aplastic crisis in the adult population [7].
Red Cell Aplasia
Parvo B19 virus may result in a chronic or recurrent pure red cell aplasia, whereby the bone marrow erythroid lineage arrests in the G1 and G2 cell cycle stage due to the cytotoxic non- structural 1 protein expression and UV-inactive B19 viruses [8]. This anaemia persists until a host or passive neutralizing antibody is generated, or administered respectively [9]. This pure red cell aplasia occurs predominantly in patients with immuno-compromised states, such as those with lymphoproliferative neoplasms, transplants recipients, and in the South African context, HIV infection with immune suppression, with or without co-morbid zidovudine marrow suppression, is a major cause [4].
Clinically, this anaemia may present as weakness, fatigue, shortness of breath, pale skin or mucous membranes, as well as with systolic cardiac murmurs, depending on the severity of the anaemia. The distinctive slapped-cheek rash and arthralgia typically caused by parvo-B19 are usually not present, as these are immune mediated [10]. This anaemia is typically a severe normocytic normochromic anaemia with reticulocytopaenia, with a concurrent bone marrow examination revealing the absence of red-cell precursors or the presence of giant pro-normoblasts with intra-nuclear inclusions, as reflected in Figures 1 & 2) [11]. Serologically, patients may express variable viral capsid antigen (anti-B19) IgM, with Anti-B19 IgG being present and positive with limited neutralizing capacity. Thus, polymerase chain reaction confirmation is favoured in such patients with limited immune response capacity [12].
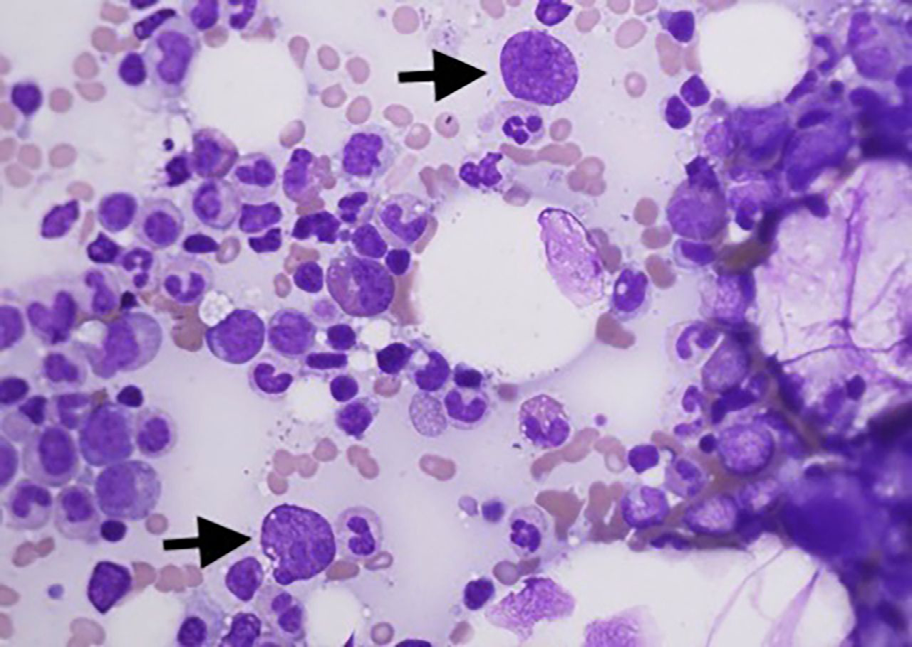
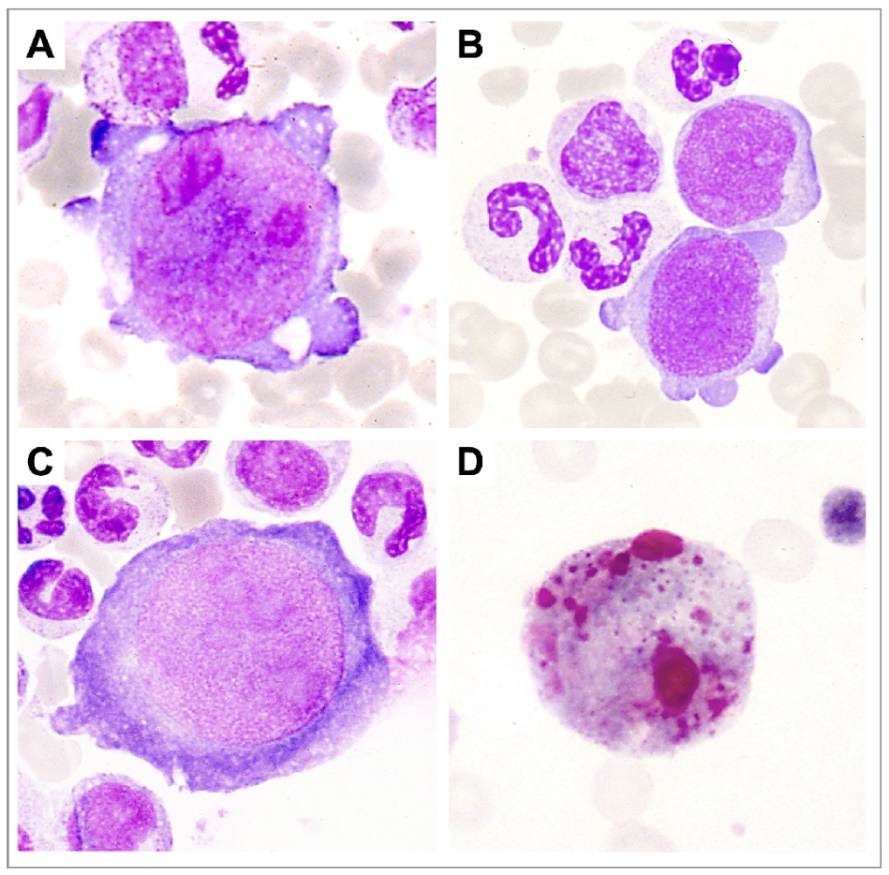
Figure 2: (Courtesy of Journal Haematologica – LN 230323). (A and B) Image showing marked erythroblast lineage hypoplasia. Additionally, there is atypical hyperbasophilic giant cells with very large, prominent nucleoli. These are giant cells also called giant pro-normoblasts, are pathognomonic of Parvo B19 infection. (C) An imaging showing an enormous pro-erythroblast with numerous nuclear inclusions. (D) An image showing atypical erythroblasts.
Management may vary per institution protocol, but may include some or all of the following: packed red cell transfusion, based on the degree of anaemia, and the administration of intravenous immunoglobulin at 1g/kg over a period of 2 days, or more preferably, 500mg/kg over a period of 5 days, the latter having fewer adverse effects, as well as a safer profile for patients with underlying cardiac and renal pathologies [12]. Most patients respond after 1-3 doses of intravenous immunoglobulin [12]. Additionally, the underlying risk factors should be corrected, especially the administration of highly active anti-retroviral therapy, in HIV infected patients [9, 12, 13].
Transient Aplastic Crisis
Parvovirus B19 may result in a transient aplastic crisis (TAC). This is a temporary suspension of erythropoiesis secondary to the parvo-B19 virus attaching to the P-antigen receptor and subsequent destruction and failure of the pro- erythroblasts to develop later stage erythroid precursors [14]. This frequently leads to a severe and life threatening anaemia with a similar or if not more pronounced clinical presentation to that of aplastic pure red cell aplasia. Additionally, patients may show non-specific flu like symptoms, fever and lethargy [11, 14].
TAC occurs more frequently in patients with underlying red-cell abnormalities these include states with high erythrocyte destruction, such as sickle cell disease, autoimmune haemolytic anaemia and hereditary spherocytosis, as well as in patients with reduced erythrocyte productive states such iron deficiency anaemia. Additionally, the Genotype 3, the most common variant in sub-Saharan Africa, is more associated with TAC than other variants [15].
Patients usually have a severe anaemia with variable types ranging from microcytic hypochromic to normocytic normochromic with a reduced reticulocyte percentage and index. Additional features such as spherocytes, erythrocyte aggregation or sickle cells may be present depending on the patients underlying co-morbid red cell pathology. The marrow findings usually reflect a red cell aplasia with giant pro-normoblasts with viral nuclear inclusions. This pathology is largely limited to one to two weeks in durations, with red cell transfusion being sufficient for the management of anaemia. The addition of immunoglobulin administration, at 500mg/kg over a 5 day period, may be needed for patients who are immuno-compromised, such as those with HIV infection [14, 15, 16, 17].
Conclusion
Parvovirus B19 remains a prevalent and prominent virus associated with multiple medical conditions particularly in immunocompromised states such as that of HIV, as well as erythrocyte disorders. Clinically, the virus has a plethora of presentations, especially severe anaemia. These conditions may be effectively and successfully managed with intravenous packed red-cell transfusions, intravenous immunoglobulins and by addressing the underlying patient risk factors.
Acknowledgments
The authors would like to thank the British Medical Journal and Journal Haematologica for their permission in allowing the use of their figures for the purposes of this article.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding
None
References
-
(1993) Virus taxonomy update. The International Committee on Taxonomy of Viruses. Arch Virol. 133(3- 4): 491-495.
-
Parsyan A, Szmaragd C, Allain JP, Candotti D ( 2007) Identification and genetic diversity of two human parvovirus B19 genotype 3 subtypes. J Gen Virol 88(2): 428-431.
-
Mirambo MM, Maliki F, Majigo M, Mushi MF, Moremi N, et al. (2017) The magnitude and correlates of Parvovirus B19 infection among pregnant women attending antenatal clinics in Mwanza, Tanzania. BMC Pregnancy Childbirth 17(1): 176.
-
Glatt N (2017) The prevalence of parvovirus B19 infection in a cohort of HIV infected patients with severe anaemia. Wits Wired.
-
Heegaard ED, Brown KE (2002) Human parvovirus B19. Clin Microbiol Rev 15(3): 485-505.
-
Francois KL, Parboosing R, Moodley P (2019) Parvovirus B19 in South African blood donors. J Med Virol 91(7): 1217-1223.
-
Cilla N, Domitien L, Arrada N, Chiffre D, Mahe P, et al. (2020) Transient aplastic crisis triggered by parvovirus B19 in a family with hereditary spherocytosis. IDCases 21: e00802.
-
Chisaka H, Morita E, Yaegashi N, Sugamura K (2003) Parvovirus B19 and the pathogenesis of anaemia. Rev Med Virol 13(6): 347-359.
-
Gigler A, Dorsch S, Hemauer A, Williams C, Kim S, et al. (1999) Generation of neutralizing human monoclonal antibodies against parvovirus B19 proteins. J Virol 73(3): 1974-1979.
-
Koch WC, Massey G, Russell CE, Adler SP (1990) Manifestations and treatment of human parvovirus B19 infection in immunocompromised patients. J Pediatr 116(3): 355-359.
-
Thibile S, Barrett C, Potgieter S, Joubert G, Malherbe J, et al. (2022) Adult pure red cell aplasia at Universitas Academic Hospital, Bloemfontein, South Africa: A 9-year review. S Afr Med J 112(9): 753-759.
-
Koduri PR (2000) Parvovirus B19-related anemia in HIV- infected patients. AIDS Patient Care STDS 14(1): 7-11.
-
Kurtzman G, Frickhofen N, Kimball J, Jenkins DW, Nienhuis AW, et al. (1989) Pure red-cell aplasia of 10 years’ duration due to persistent parvovirus B19 infection and its cure with immunoglobulin therapy. N Engl J Med (8): 519-523.
-
Nandu NS, Hafzah H, Patel C (2020) Parvovirus-Induced Transient Aplastic Crisis in a Patient With Newly Diagnosed Hereditary Spherocytosis. Cureus 12(7): e8995.
-
Nguyen QT, Sifer C, Schneider V, Allaume X, Servant A, et al. (1999) Novel human erythrovirus associated with transient aplastic anemia. J Clin Microbiol 37(8): 2483- 2487.
-
Manthri S, Chakraborty K (2019) Acute parvovirus B19 infection diagnosed by bone marrow biopsy. BMJ Case Rep 12(5): e230403.
-
Invernizzi R (2022) Images from the Haematologica Atlas of Hematologic Cytology: parvovirus-induced pure red cell aplasia. Haematologica 107(7): 1493.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia