Proposal for the Use of Canakinumab in Acute Respiratory Distress Secondary to COVID-19 Infection
The outcome of the SARS-CoV-2 (COVID-19) infection mainly affects the pulmonary field, causing a picture of ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS). This process is an inflammatory condition, caused by a cascade of cytokines under the protection of the NLRP3 INFLAMOSOME, which is mainly responsible for the destruction of the alveoli. Among all the cytokines that are triggered in this picture, IL-1Î’ stands out. CANAKINUMAB is a potent biological drug, capable of blocking this IL-1Î’. We propose its use, in order to control ARDS secondary to COVID-19 infection, using the intravenous route and higher doses than those used according to its technical data sheets.
Letter to Editor
It is known that the outcome of patients infected with Covid-19 is caused - in a significant number of cases - by cardiopulmonary failure: Acute Respiratory Distress Syndrome (ARDS) [1]. Since 1995, several authors have pointed out the central role of Beta IL (IL-1β) in the inflammatory cascade surrounding ARDS [2, 3]. Two publications include more than 20 patients with elevated plasma and bronchoalveolar lavage levels of IL-1β. In addition to these publications, many others confirm and describe the inflammatory picture caused by ARDS. An inflammatory environment refractory to numerous drugs has been detected, but with a common denominator: an increase in innumerable pro-inflammatory cytokines (IL-1, Letter to Editor IL-6, TNFalpha, IL-8...) [4].
In 2018, Aranda-Valderrama, et al. published a model to better understand the flow of proinflammatory cytokines in patients affected by ARDS.5 It is observed that IL-1β is located as a previous step to macrophage activation from its inactive cytokine (pro IL-1β) located in the alveolus, progressing to active IL-1β. Once the macrophage is activated, the cytokine plurarity increases and therefore, its inflammatory activity (IL-6, TNF, G CSF,CCCL2,...). In this and other publications [6], the NLPR3 inflammasome is related to its presence in the alveoli of patients with ARDS. A complex of proteins that interact in a unidirectional manner towards the generation of an inflammatory cascade in the pulmonary alveolus are treated. This complex is known to be activated in situations of stress, whether physical (trauma) or chemical/toxic (infections) [7].
Therefore, if an activated SARS-CoV-2 virus can provoke a violent immune response, it can in turn activate the NLRP3 inflammasome, causing a violent immune response with a potentially deadly ‘cytokine storm’. Inflammasomes are part of our innate immune system: they are multi-protein oligomers that mediate inflammatory responses [8, 9]. The NLRP3 inflammasome is regulated by the NLRP3 gene. This gene can detect molecular patterns that are linked to a potential hazard, called hazard associated molecular patterns (DAMPs) or pathogen associated molecular patterns (PAMPs), through pattern recognition receptors (PRRs), such as toll-type receptors (TLRs). DAMPs and PAMPs can activate the NLRP3 gene and the inflammasome in it. Activation of such an inflammasome releases large amounts of pro-inflammatory interleukins, which cause inflammation to attack the invader. In the case of SARS-CoV-2, interleukin 1β (IL-1β), one of our most pro-inflammatory cytokines, is produced (Figure 1).
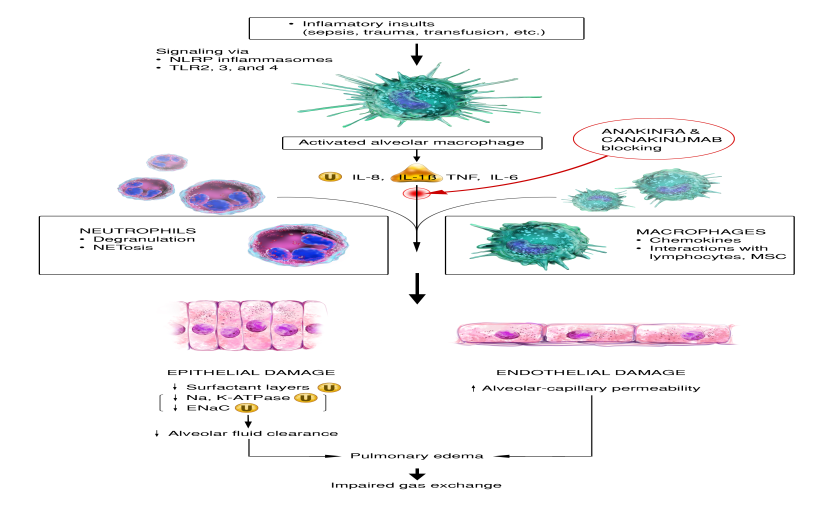
Figure 1: Initial inflammatory insults, including mitochondrial DAMPs, activate alveolar macrophages via TLR and NLR signaling pathways. Activated alveolar macrophages release proinflammatory cytokines and recruit circulating macrophages and neutrophils to injured sites. Excessive neutrophils and persistently activated macrophages cause extensive damage to lung epithelia and endothelia, resulting in an impaired alveolar–capillary barrier. Disruption of this barrier allows protein-rich fluid to enter the alveoli, causing fluid accumulation in alveolar spaces (pulmonary edema) that interferes with gas exchange.
NLRP3 inflammation can cause serious respiratory disorders: acute distress respiratory syndrome (ARDS) and acute lung injury (ALI), with the possible consequence of pneumonia (severe) [10]. We currently have a drug called Canakinumab, which binds with high affinity specifically to human IL-1β and neutralizes its biological activity by blocking interaction with IL-1 receptors, thus preventing IL-1 beta-induced gene activation and production of inflammatory mediators. Canakinumab has been shown to be effective in the treatment of autoinflammatory disease (muckle-wells, multisystemic neonatal disease, familial cold hives, hyperimmunoglobulin syndrome and cryopyrine- associated diseases, a rare genetic disease caused by an autosomal dominant mutation in the NLRP3 [11, 12].
The presence of an NLRP3 inflammasome is related to the origin of the inflammatory cascade of an ARDS picture, a fact that has been confirmed by the medical literature [10, 11]. The initiation pathway of IL-1β gives it a specific and central target in order to control the pro-inflammatory picture of the pulmonary alveolus. It is therefore a possible therapeutic target for the control of patients who may progress to ARDS after infection with COVID19.
References
-
Tang X, Du R, Wang R, Cao T, Guan L, et al. (2020) Comparison of Hospitalized Patients with Acute Respiratory Distress Syndrome Caused by COVID-19 and H1N1. Chest 26.
-
Meduri GU, Headley S, Kohler G, Stentz F, Tolley E, et al. (1995) Persistent elevation of inflammatory cytokines predicts a poor outcome in ARDS: Plasma IL-1 beta and IL-6 levels are consistent and efficient predictors of outcome over time. Chest 107(4): 1062-1073.
-
Meduri GU, Kohler G, Headley S, Tolley E, Stentz F, et al. (1995) Inflammatory cytokines in the BAL of patients with ARDS. Persistent elevation over time predicts poor outcome. Chest 108(5): 1303-1314.
-
Dinarello CA, Simon A, van der Meer JW (2012) Treating inflammation by blocking interleukin-1 in a broad spectrum of diseases. Nat Rev Drug Discov 11(8): 633- 652.
-
Aranda-Valderrama P, Kaynar AM (2018) The Basic Science and Molecular Mechanisms of Lung Injury and Acute Respiratory Distress Syndrome. Int Anesthesiol Clin 56(1): 1-25.
-
Han SH, Mallampalli RK (2015) The acute respiratory distress syndrome: from mechanism to translation. J Immunol 194(3): 855-860.
-
Franchi L, Munoz-Planillo R, Nuñez G (2012) Sensing and reacting to microbes through the inflammasomes. Nat Immunol 13: 325-332.
-
Grailer JJ, Canning BA, Kalbitz M, Haggadone MD, Dhond RM, et al. (2014) Critical role for the NLRP3 inflammasome during acute lung injury. J Immunol 192: 5974-5983.
-
Jones HD, Crother TR, Gonzalez-Villalobos RA, Jupelli M, Chen S, et al. The NLRP3 inflammasome is required for the development of hypoxemia in LPS/mechanical ventilation acute lung injury. Am J Respir Cell Mol Biol 50(2): 270-280.
-
Favero G, Franceschetti L, Bonomini F, Rodella LF, Rezzani R (2017) Melatonin as an anti-Inflammatory Agent Modulating Inflammasome Activation. Int J Endocrinol 2017.
-
Molto A, Olive A (2010) Anti-IL-1 molecules: new comers and new indications. Joint Bone Spine 77(2): 102-107.
-
Willingham SB, Allen IC, Bergstralh DT, Brickey WJ, Huang MT, et al. (2009) NLRP3 (NALP3, Cryopyrin) facilitates in vivo caspase-1 activation, necrosis, and HMGB1 release via inflammasome-dependent and -independent pathways. J Immunol 183(3): 2008-2015.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia