Non-Specific Immune Modulation Response by Use of Aboriginal Potent Herbal Combination in Diabetic Urban Population
World, a globally experiencing rapid socioeconomic progress and urbanization, carries a considerable share of the global diabetes burden. In the present study, powdered dodecyl sulphate of ‘poly-herbal formulation’ was evaluated for its imuno-enhancing/modulation potency to polymorpho nuclear lymphocytes, against normal and diabetic individuals. Subjects were divided into three groups of 140 subjects in each group consisted of all men in urban population (Mean age, 45 + 12.8 years). group I were diabetics, group II were tolbutamide (oral hypoglycemic drug) treated diabetic patients, group III were receiving combination herbal formulation in the, dosage of 5 g. /Day for one month. Results were analyzed using Student ‘t’ test followed by Tukey's test. Significant changes were noticed in Cellular water content, calcium concentration contact angle, Phagocytosis and Phagocytic index, parameters in normal diabetic patients, Tolbutamide treated diabetics and diabetics’ individuals treated with different dosages ‘polyherbal combination formulation’ alone. The efficacy of ‘ Drug formulation’ as an increase phagocytosis activity and strength the non-specific immune system which is the first line of defense in innate immunity gets disturbed in diabetic patients resulting in array of infection in them which might be reduces the risk of non-specific infection of diabetic individuals.
Introduction
Diabetes mellitus is one of the most prevalent and serious diseases in the World. Diabetes mellitus affects approximately 14% urban and 2.9% rural people and approximately more than 500 million people worldwide and accounts for about one fifth of all expenditures for health care and day by day increase this number rapidly [1, 2, 3]. Patients with type 2 diabetes mellitus (T2DM) are immunocompromised and have an increased incidence of infections, mainly in the bone and skin, as well as in the respiratory, enteric and urinary tracts [4]. Diabetic foot ulcers are often complicated by infection and represent the first cause of non-traumatic amputations and are a leading cause of hospitalization among diabetic patients [5]. Diabetes also influences the outcomes of specific infections, such as bacteremia and mortality following community-acquired pneumonia [6]. In addition, it has recently been reported that diabetes triples the risk of hospitalization after influenza A (H1N1) infection and quadruples the risk of intensive care unit admission after hospitalization [7].
The reasons why diabetic patients present an increased susceptibility to frequent and protracted infections are still far from being understood. Several factors have been suggested, including genetic susceptibility to infection, local factors including poor blood supply and nerve damage, alterations in metabolism associated with diabetes, and defects in innate immune defence mechanisms [8]. Regarding the innate immunity, phagocytic activity of peripheral blood mononuclear cells (PBMCs) plays an essential role in protecting the host from infectious diseases, and decreased PBMC function has been implicated in the increased risk of infections that occurs in diabetic patients [9]. Hyperglycemia and poor glycemic control are considered to be the key basal factors in the development of diabetes and its associated secondary complications. Moreover diabetics also suffer from delayed wound healing and depressed infection fighting capability due to decrement in phagocytosis efficiency. Numerous experimental studies based on clinical observation showed that Phagocytic function of various cells were decreased in diabetes, investigation carried out to understand the pathogenesis of these changes have shown that the changes in cholesterol/phospholipids ratio of the cell membrane due to diabetic infection [10, 11].
Consequently since phagocytosis is one of the properties of cell membrane. Phagocytosis is carried out by specific group of cells in the body, the efficient working of these cells depends upon their membrane potential regulated the enzymes Na+/K+, ATPase and calcium homeostasis in their intracellular milleau [12]. Diabetics are more prone to long lasting infections due to several above reasons. The modulation of immune response by using medicinal plant products as a possible therapeutic measure has become a subject of active scientific investigation. The basic concept has, however, existed in the ancient Vedic scripture, ‘The Ayurveda. The main reason for the sages request to the gods was to avoid diseases and remain fit for a long time. Hence the major approach to therapy in Ayurveda is one which emphasizes prevention. Certain medicinal plants can play a great role in improving phogocytosis thereby potentiating the immune system the presented study was to evaluate the efficacy of novel herbal drug formulation to enhance the non-specific immune system from diabetic patients.
Materials & Methods
The plants were selected on the bases of their potential activities and wide medicinal uses in the traditional literatures. The ease of availability of plant is also taken into consideration during selection. Roots of Asparagus racemosus (Shatavari), Andrographis paniculata (Kalmegh), and Tinospora cordifolia (Guduchi) rhizomes and leaves of Gymnema sylvestre (Gudmar) were collected and authenticated by the “Sanjivani Nursery”, Department of Forest, Government of Madhya Pradesh, Link Road, Bhopal (M.P.) India [8, 9, 10, 11].
Formulation
After preparation of dry powder and mixed properly until a homogeneous mixture was obtained, the next step was to formulate a polyherbal preparation. The mixture was encapsulated to ensure blinding, uniformity of administration and for convenience of patients (Table 1). One capsule contained 500mg of the blended herbal powder [12].
| Subjects | Fasting Plasma Glucose(mg/dl) | ||
|---|---|---|---|
| S. No | N=60 | Zero Weeks | Four Weeks |
| 1 | NH | 78.4±8.5 | 79.0±5.2 |
| 2 | DI | 174±15.4b | 288.6±42.6a |
| 3 | TTD | 163.9±2.0 | 82..1±1.5 |
| 4 | HFTD | 165.9±28.5a | 80.1±2.0 |
| ap<0.0001,bp<0.01 | |||
Table 1: Effect of combination herbal drug formulations on the fasting plasma glucose level in diabetic patients after treatment
Ethics Statement
Informed written consent was obtained from all participants and the study was approved by the hospital's human ethics committee (K.N.Katju Hospital and Hamidia Hospital). After taking permission for clinical studies from the volunteers were selected as per norms of center ethics committee on human research (CECHR) and local ethics committee. (Reg.No.1/441). No patients had any severe infection nor were on any sort of medication.
Case-Control Study
In this study we have investigated the effect of type 2 diabetes and the degree of glycaemic control on the phagocytic activity of monocytes/macrophages. On this basis, of case control study, a total of 60 type-2 diabetic patients of urban origin and free of chronic diabetic complications who were attending the outpatient Diabetes Unit of hospital were recruited for the study over a 1-month period (cases). Subjects were divided into four groups of 60 subjects. Group I (NH) were normal healthy subjects, Group II (DI) were diabetics , group III (TTD) were tolbutamide, group IV .(HFTD-1, HFTD-2, HFTD-3 (three different dosage class) were diabetic patients receiving combination herbal formulation in the, dosage of 1g/day, 2.5g/day and 5 g. /day for 4 weeks [13]. The formulation was administered one hour before food to prevent any interference with its absorption. Diabetic patients were contacted and convinced from two government hospitals-Hamidia Hospital, Bhopal and K.N. Katju hospital, Bhopal.
Determination of Blood Glucose Level
The blood glucose level was measured in all the groups by using Glucose oxidase-peroxidase method (Autoanalyser method), Oral glucose tolerance test: (OGTT) [14].
Isolation of PMNL (polymorphonuclear leukocyte)
After an overnight fast of 10 h, venous blood was collected from the antecubital vein in preheparinised syringes at 8.00 am. During the next 60 minutes 100 µL of the heparinized whole blood was exposed for 30 minutes at 37°C in the dark to 20 µL of eppendrorf tube. PMNL were isolated by the method of with slight modifications [15]. 10 to 15 ml fasting blood samples were drawn into heparinized tubes already containing 5% dextran (prepared in 0.9% NaCl; use 2 ml 5% dextran for every 10ml of blood).. This preparation contained 97-99% PMNL when viewed under phase contrast microscope. (Tarl-zeif, AXIOVERT-200).
Ca2+/Mg2+ - ATPase of the Plasma Membrane
Plasma membrane fraction was prepared as described in methodology (Chari and nath 1984) and was finely suspended in 0.34 M sucrose [16]. The suspension served as the enzyme source. Ca2+/Mg2+ - ATPase activity was assayed by the method of Lynch and Cheung [17]. Incubation mixture consisted of 40mM Tris-HCl (pH 7.4), 3mM MgCl2, 80mM NaCl, 20mM KCl, 0.2mM Ouabain, 2mM ATP, 100 μM Ca2+ and enzyme preparation in a final volume of 0.4 ml. Reaction mixture was incubated for 30 min at 370C. Reaction was terminated by the addition of 0.08 ml of 5% solution of sodium dodecyl sulpfate. Inorganic phosphate released was measured and the blue color developed after 10 min was read at 660 nm. Specific activity was expressed as n mol of Pi liberated/min/mg protein [18].
Cyclic-3’, 5’-Adenosinemonophosphate Phosphodiesterase Activity
PMNL were suspended in 0.34 M sucrose and homogenized with chilled Teflon pestle for 1 min. Cells were further disrupted by sonication for 1 min in a Ralsonics Sonicator with controls set at 140. Broken cells were centrifuged at 600 x g for 10 min and the supernatant so obtained was again centrifuged at 15,000 x g for 20 mins. The supernatant so obtained served as the enzyme source. cAMP phosphodiesterase activity was assayed by the previously described method of Butcher, et al_._ [19].
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$
The reaction mixture consisted of 0.36
AMP, 1.8μmoles MgSO4, 36
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$
Tris-HCl buffer (pH 7.5) with a suitable dilution of the enzyme source in a final volume of 0.9 ml. This mixture was then incubated at 300C for 30 min. After the first 20 min. of incubation, 0.1 ml Crotalus Atrox venom solution was added containing 0.1 mg venom in 1 x 10-2M Tris-HCl buffer (pH 7.5). The entire reaction was terminated by the addition of 0.1 ml of cold 55% TCA. The precipitate was removed by centrifugation and aliquot of the supernatant was analyzed for inorganic phosphate by the modified method of Fiske and Subbarow Specific activity was expressed as nmol of pi liberated/min/mg protein [20].
Phospholipasec Activity
Broken PMNL were centrifuged at 600 x g for 10 min. and the pellet thus obtained was washed twice and resuspended in 0.34 M sucrose. This suspension served as the enzyme source. Phospholipase c activity using phosphatidylinositol or phosphatidy 1- choline or phosphatidylethanolamine as substrate was assayed by the method described previously by Ottolenghi [21]. Required quantity of phosphatidyl-inositol, phosphatidyl choline and phosphatidyl-ethanolamine was suspended in triple distilled water and sonicated vigorously for 20 min for a complete dispersion of aforementioned phospholipids. Reaction mixture consisted of 5 µmol sonicated phosphatidylinositol or phosphatidylcholine or phosphatidylethanolamine, the desired enzyme aliquot, sufficient water and Tris-maleate buffer (pH 7.2) to make the final 5ml system, 5mM with respect to tris.
The mixture was then incubated at 37°C and duplicate 2ml samples were taken at appropriate times and added to centrifuge tubes containing 4ml cold 10% HClO4, 0.5 ml 2% albumin was then added to aid precipitation. The tubes were then allowed to stand in ice for 30 min and then centrifuged. The remaining floating particles were filtered off through a Millipore filter. Digestion of the filtrate was carried out in an oil bath at approximately 170°C for 2 to 2.5 hrs. The solution was then allowed to cool. Phosphate measurement was done by addition of 10ml of the reagent used by Lowry (50 µl of 0.25% ammonium molybdate in 0.1 N sodium acetate to which add 1ml of 10% ascorbate per 10ml solution) [22]. After development of the color for 30min at 37°C, the optical density was read at 740 nm Specific activity was expressed as nmol of Pi released/min/mg protein.
Phagocytosis
Experiments on phagocytosis, unless otherwise stated, were performed by suspending PMNL in Hank’s balanced salt solution (with glucose) and incubating with 0.01 ml polystyrene latex beads for 20 minutes at 370 C in a shaking water-bath. Phagocytosis was stopped by the addition of one mg iodoacetate a preparation of zymosan granules (0.01ml) was used sometimes in place of latex beads [23].
Measurement of Phagocytic Index
The extracts were combined, and the optical density of the purple color of reduced nitroblue tetrazolium (NBT) was determined at 515 nm against a pyridine blank. The optical density of an extract of cells and NBT incubated for 10 sec was also determined, and this value was subtracted from the others as a reagent blank. Resting and phagocytosing values were obtained and the difference (OD per 15 min per 2.5 x 106 PMNL) calculated was expressed as phagocytic index [24].
Statistical Analysis
Normal distribution of the variables was evaluated using the Kolmogorov–Smirnov test. Data were expressed as the means and standard deviation. Comparisons between groups were made using the Student's t test for continuous variables and the χ2 test for categorical variables. All p values were based on a two-sided test of statistical significance. Significance was accepted at the level of p<0.05. Statistical analyses were performed using the SSPS statistical package (SPSS, Chicago, IL, USA [25]).
Results
Many herbal products have been described for the care of diabetes mellitus in ancient literature of ‘Ayurveda’ in India. The present study demonstional significant improvement in the level of FBG and glucose tolerance with the use of herbal formulation a dosage of 5g/day (containing 1g Gymonema sylvesterase in diabetic patients when used as mono therapy does not causes hypoglycemic and is this termed anti-hyperglycemic. The present formulations at a prescribed dosage could bring down the sugar level to normal, which was at par with the oral hypoglycemic drug tolbutamide (Table 1). Similar improvement was seen in glucose tolerance studies also Table 2 in the prescribed dosage of the formulations, the peak value after one hour were normal range (140.3±3.0 mg/dI) and after two hours the plasma glucose value were not normal, but even lower the initial value (82.5 Vs 84.1 mg /dI) in this case also the result were almost comparable with allopathic drug tolbutamide.
| S. No | Subjects | Plasma Glucose (mg//dl) | ||||
| S. No | N=60 | 0 hrs | 0.5 hrs | 1 hrs | 1.5 hrs | 2 hrs |
| 1 | NH | 81.0±6.5 | 112.5±4.2 | 142.2±5.3 | 98.5±6.7 | 84.3±5.2 |
| 2 | DI | 160.7±14.3a | 240.5±77.2b | 270.0±90.0b | 282.5±81.4a | 273.1±83.2a |
| 3 | TTD | 80.0±1.0 | 109.0±1.5a | 143.3±7.5a | 98.5±2.3a | 79.5±2.5c |
| 4 | HFTD | 84.1±2.0 | 112.0±2.5a | 140±3.0a | 104.7±2.3 | 82.5±3.6c |
Table 2: Plasma glucose level in glucose tolerance test after weeks of treatment.
| Subject | Na+/K+ - ATPase (ouabain sensitive).mμ moles of Pi liberated/min/mg protein | Na+/K+ - ATPase (ouabain insensitive).mμ moles of Pi liberated/min/mg protein | |||
| Resting | Phagocyting | Resting | Phagocyting | ||
| 1 | NH | 4.67±0.41 | 0.94±0.09 | 19.93±2.31 | 42.11±2.31 |
| 2 | DI | 1.37*±0.17 | 0.69**±0.19 | 9.64±1.07* | 16.83*±2.70 |
| 3 | TTD | 2.11***±0.76 | 0.81**±0.11 | 10.23ns±1.91 | 18.19ns±3.62 |
| 4 | HFTD | 3.93±0.81 | 0.84±0.2 | 18.51±1.99 | 36.11±2.61 |
Table 3: change in the activities ouabain sensitive) and insensitive ATPase of Polymorphonuclear leucocyte (PMNL).
*P<0.001 as compared to group-I P<0.01 as compared to group-I *P<0.02 as compared to group-I Ns= non-significant as compared to group-I Table 3: change in the activities ouabain sensitive) and insensitive ATPase of Polymorphonuclear leucocyte (PMNL).
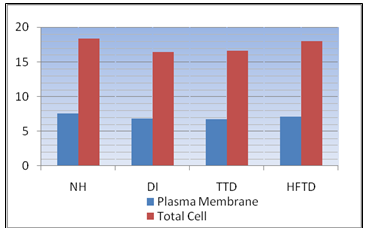
Phagocytosis which is the first line of defiance gets disturbed in diabetic patients resulting in an array of infections in them. Phagocytosis is carried out by specific group of cells in the body polymorphonuclear leucocyte (PMNL). The activity of ouabain (insensitive) ATPase escalated during phagocytosis in normal PMNL, (control), (91.63 %). PMNL obtained from untreated diabetic patients had quite depressed activity of this enzymes both in resting and phagocytosing state as compared to normal, (control), Table 4 tolbutamide treated diabetic group did not show any significant recovery As shown (Figure 1), the leucocyte (Ca2+) of diabetics recorded significant increment (104±0.2 nmol) as compared to normal (control ), (67±0.5nmol),(p<0.001). The sight, but not insignificant decrease in total as well as plasma membrane (PM), Calcium was noticed in untreated as well as tolbutamide treated diabetic patients. The values of total as well as PM calcium were observed (Figure 2).
The leucocyte (Ca2+) of diabetics recorded significant increment (104±0.2 nmol) as compared to normal (control), (67±0.5nmol), (p<0.001). The sight, but not insignificant decrease in total as well as plasma membrane (PM).
| Subject | cAMP Phosphodiesterase activity(nmol PI liberated/min/mg protein) | |
|---|---|---|
| N=60 | ||
| 1 | NH | 3.51±0.41 |
| 2 | DI | 1.32*±0.09 |
| 3 | TTD | 2.26**±0.43 |
| 4 | HFTD | 3.18ns±0.56 |
Table 4: Phospholipase-c activity of PMNL using varied substrate under resting condition.
*P<0.001 as compared to group-I Ns= non significant as compared to group-I Table 4: cAMP Phosphodiesterase activity of PMNL in resting state.
| S.No | Subject | Phospholipase-c | ||
| S.No | N=60 | (n mol of Pi liberated/min/mg protein) | ||
| S.No | substrates | |||
| S.No | Phosphatidylinositol | phosphatidylcholin | Phosphatidylethanolamine | |
| 1 | NH | 3.76±0.16 | 5.14±0.64 | 4.73±0.35 |
| 2 | DI | 1.43*±0.32 | 2.41*±0.43 | 2.13*±0.11 |
| 3 | TTD | 1.91*±0.34 | 3.21*±0.72 | 2.98*±0.71 |
| 4 | HFTD | 3.01*±0.27 | 4.96*±0.2 | 4.39**±1.99 |
Table 5: cAMP Phosphodiesterase activity of PMNL in resting state.
*P<0.001 as compared to group-I *P<0.02 as compared to group-I Table 5: Phospholipase-c activity of PMNL using varied substrate under resting condition.
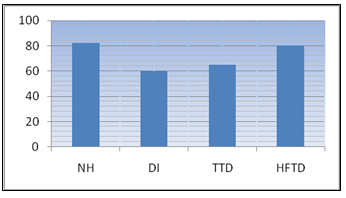
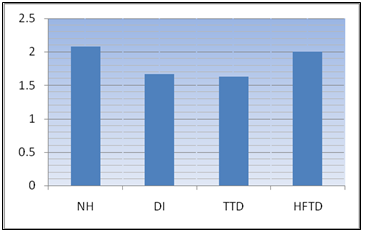
Table 4 reveals the cAMP Phosphodiesterase profile of normal diabetic and treated PMNL in resting state. cAMP Phosphodiesterase activity was significantly low in resting diabetic PMNL (1.22±0.09nmol) as compared to normal (control). Figure 3 represented the fold increase in activity of cAMP Phosphodiesterase of normal diabetic, tolbutamide treated and herbal drug treated PMNL during phagocytosis. The activity of this enzyme rases 2.08 fold in normal phagocytosing PMNL as compared to resting values. The raise was only 1.63 fold in diabetic PMNL. There was a partial recovery in the fold increase of phagocytosis PMNL of controlled diabetic patients, Response with tolbutamide being quite insignificant (1.6 fold) and herbal formulation being appreciable 2.0 fold (Table 5). Contact angle of Opsonized E.coli. (29˚± 1˚) and S.aureus (24.3˚±1˚) were higher as compared to their unopsonized counter parts (26˚±1* and 19.7˚±1˚ respectively).
| S.No | Subject | Particles internalized | %PMNL participation in Phagocytosis | ||||||
| S.No | N=60 | E.coli | S. aureus | E.coli | S. aureus | ||||
| S.No | opsonized | unopsonized | opsonized | unopsonized | opsonized | unopsonized | opsonized | unopsonized | |
| S.No | Value represented as mean +SE | Only mean values represented | |||||||
| 1 | NH | 4.6±0.36 | 2.7±0.27 | 2.2±0.24 | 1.3±0.12 | 88 | 85 | 51 | 43 |
| 2 | DI | 1.7±0.14* | 0.32±0.09* | 0.21±0.03 | 0.08±0.01 | 68 | 55 | 11 | 11 |
| 3 | TTD | 1.8±0.17* | 0.34±0.21* | 0.23±0.09* | 0.07±0.01 | 63 | 57 | 12 | 12 |
| 4 | HFTD | 4.3±0.16** | 1.9±0.12 | 1.46±0.06* | 1.0±0.02 | 79 | 74 | 43 | 39 |
Table 6: comparative Phagocytic capabilities of PMNL with Opsonized and unopsonized E.coli and S. aureus.
*P<0.001 as compared to group-I P<0.02 as compared to group-I *P<0.1 as compared to group-I Table 6: comparative Phagocytic capabilities of PMNL with Opsonized and unopsonized E.coli and S. aureus.
| S.No | Subjects | Phagocytic index |
|---|---|---|
| N=60 | OD=515nm(Phagocytic cells) | |
| 1 | NH | 0.26±0.02 |
| 2 | DI | 0.14±0.05 |
| 3 | TTD | 0.23±0.01 |
| 4 | HFTD | 0.22±0.01 |
Table 7: Changes in Phagocytic index (NBT reduction test of PMNL).
Contact angle was significantly increased in diabetic
PMNL (25.2˚±0.1˚) compared to normal (17.20˚±0.1˚)
(Figure 4). Phagocytic capability of normal PMNL was
$$ h i g h e r u s i n g O p s o n i z e d E. c o l i (4. 6 \pm 0. 3 6 p a r t i c l e s $$
internalized) S. aureus (22+0.24 particles internalized), as
compared to the Phagocytic capability with unopsonized
particles (Table 6). Among these E.coli demonstrated a
higher Phagocytic capability compared to S. aureus. The
Phagocytic index (NBT reduction assay) estimates the
ability of neutrophills and macrophages to produce
oxygen radicals (O2, OH-, H2O2). The ability of PMNL and
macrophages to kill pathogenic microbes is probably one
of the most important mechanisms of defense NBT
reduction assay (Table 7). It is evident that the Phagocytic
index of diabetic PMNL, (0.12±0.05) in highly depressed
as compared to normal (0.23±0.02).
![Figure 1: Alteration in cytosolic calcium concentration [Ca2+] of Polymorphonuclear leucocyte (PMNL).](/fulltextimages/2597/fig_1.png)
Discussion
In the present study we provide evidence that in diabetic mellitus (T2DM) patients the attenuated phagocytic activity of PMNLs exhibits a significant reversibility after glycemic control is improved. In addition, our baseline results confirm and extend previous reports concerning the impairment of phagocytosis that occurs in PMNLs from diabetic patients [26]. Previous studies have described diminished PMNLs function (i.e. defective chemotaxis, bacterial killing, superoxide production, leukotriene release, lysosomal- enzime secretion and endoplasmic reticulum stress) as well as altered basal levels of intracellular calcium and superoxide in diabetes [27].
In the present study a homogenous population of patients with T2DM was analyzed, the number of subjects included was sufficient for the purpose of the study, a close matched control group was included, the collection of PMBCs was accurate and the method used for measuring phagocytic activity was highly sensitive and reproducible [28]. Nevertheless, further studies addressed to examining the clinical usefulness of this method for evaluating the risk of diabetic patients to acquire infections are needed. Phagocytic cells are the cornerstone of the innate immune system, and individuals with inherited defects in phagocyte function typically present recurrent, unusual, and/or difficult to clear bacterial infections [29]. Our findings reinforce the theory that, in contrast to the sustained immune deficits that occur in genetic disorders, the extent of impairment of phagocytosis in diabetic patients oscillates in relation to glycemic control [30].
Therefore, persistently poor glycemic control could have a progressively deleterious effect, predisposing affected individuals to an increased incidence and severity of infection [31, 32]. In addition, our results suggest that an improvement of phagocytic activity can be considered as another beneficial effect of hyperglycemia optimization. The reasons why hyperglycemia or related pathways down regulate phagocytic activity remain to be elucidated [33]. The deleterious effects of free radicals are enhanced in diabetes, because they are less easily eliminated as a result of the reduced effectiveness of the protecting agents. Diabetes activates aldose-reductase which leads to a reduction of glucose excess in sorbitol (polyol pathway) [34].
This pathway is a great consumer of NADPH, which is then less available for PMNLs functions and for free radical elimination by antioxidants. In fact, aldose reductase inhibition enhances neutrophil oxidative killing by diabetic neutrophils. Although our data on the improvement of phagocytosis dysfunction [35]. Numerous experimental studies based on clinical observation showed that Phagocytic functions of various cells were decreased in diabetics. Investigations carried out to understand the pathogenesis of these changes in the cholesterol/phaspholipid ratio of the cell membrane due to diabetic infection cause hypercholestrolmia [36]. This has been associated with a decreases in membrane fluidity, thus altering several function including the cation transport mechanisms specially Na+/K+ ATPase activity.
A decrease in the activity of Na+/K+ ATPase has been observed in diabetic macrophages and PMNL’s. Androphecous paniculata roots which were included in the herbal formulation have claimed to be an activator of Na+/K+ ATPase activity. A recovery in the activity of Na+/K+-ATPase in diabetic PMNL consequent to the administration of 5grams/day of the herbal formulation for four weeks also demonstrate significantly recovery in the cellular water contents. Simultaneously activity Ca2+/Mg2+ ATPase was also assayed. It is the enzymes responsible for the mobalizaation of calcium from intercellular stores. It is also become imperative to determine the total as well as plasma membrane calcium content. It was successful attempts where the formulation containg Aspargous reacemosous and Tinospora cardifolia could implement a correction in the cell [Ca2+]c. which had been found to be disturb in diabetic mellitus . It is well recognized that in diabetic leucocyte mobility chemotoxins and phagocytosis are grossly decreased [37]. There are no doubt that plats like Aspargous racemosous and Tinospora cordifolia have been proved to be immune potentiating as well as antioxidant in the vast literature assayable on medicinal plants.
Evidence of opsonisation affecting a raise in bacterial contact angle and associated phagocytic ability with normal PMNL, and the finding of the difference in contact angle (Delta-c) between normal PMNL, with E.coli being greater than S.aureus eliciting higher bacterial internormalization in proportion to (Delta-c) is in conformation with the concept that hydrophobicity determines Phagocytic capability. Ethanolic extract of T. cardifolia has been shown to improve phagoytic function in mice [38]. Root of A. racemosous , and T. cordifolia are well known for their immune-potentiating effect [39, 40].
But till date no work was ever done on studying the effect of herbal drugs on enzymes, which are so important in maintaining a proper biochemical balance inside the cell. In the present study where roots of above plants were blended and included in the formulation were quite effective since they could demonstratrate a significant recovery by increasing activity of the enzymes Phaspholipase-C, in HFTD, PMNL during resting followed by an enhanced increase during phagocytosis [41]. The combination herbal formulation demonstrate a significantly recovery in all the above mentioned parameters. Increment in generation of superoxide anion during phagocytosis is an established fact and in thought to play an important role in microbial killing. It may , however be pointed that superoxide radicals and its product the hydroxyl radical may be very toxic to the host cell as well in order to a null the inherent toxicity of these free radicals [42, 43, 44, 45] .
Conclusion
The herbal formulation could thus prove its efficacy by reducing higher sugar level; potentiating the immune system and improving the anti-oxidant status of diabetic patients the presence of T2DM and the degree of glycaemic control are related to substantially impaired phagocytosis activity which is reversible after glycemic control has been improved. Our results suggest that an improvement in phagocytic activity can be added to the beneficial effects of metabolic optimization. Further studies addressed to examining whether this improvement of phagocytic activity leads to a reduction of the rate of infection in diabetic patients are needed. Present therapeutic strategies mostly try to relief the chemical manifestation of diabetic and its complications. The major challenge in diabetic research is to define not only the cause –effect relationship between various risk factors and complications, but also to compared the effects of pharmaceutical agents that are beneficial in the management of diabetic complications. The specific activity in the formulation has been proven scientificcally in the present study and will really prove to be a “boon” for diabetic patients, in the coming future.
References
-
Ogbonnia SO, Adekunle AA, Olagbende–Dada SO, Anyika EN, Enwuru VN, et al. (2008) Assessing plasma glucose and lipid levels, body weight and acute toxicity following oral administration of an aqueous ethanolic extract of _Parinari_ _curatellifolia_ Planch (Chrysobalanceae) seeds inalloxan-induced diabetes in rats. Afr J Biotech 7 (17): 2998-3003.
-
Vats RK, Kumar V, Kothari A, Mital A, Uma Ramachandran (2000) Emerging targets for diabetes. Curr Sci 88: 241-247.
-
Weidmann P, Boehlen LM, DE Courten M (1993) Pathogenesis and treatment of hypertension associated with diabetes mellitus. American Heart Journal 125(5): 1498-1513.
-
Zhicai Zhang, Feng-Jie Cui (2007) Non-enzymatic glycosylation reaction contributes to a rise of blood glucose in alloxan-induced diabetic rats. Int J Diabetes & Metabolism 15: 52-59.
-
Joshi N, Caputo GM, Weitekamp MR, Karchmer AW (1999) Infections in patients with diabetes mellitus. N Engl J Med 341(25): 1906-1912.
-
Shah BR, Hux JE (2003) Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care 26(2): 510-513.
-
Fisher TK, Wolcott R, Wolk DM, Bharara M, Kimbriel HR, et al. (2010) Diabetic foot infections: A need for innovative assessments. Int J Low Extrem Wounds 9(1): 31-36.
-
Yende S, van der Poll T, Lee M, Huang DT, Newman AB, et al. (2010) The influence of pre-existing diabetes mellitus on the host immune response and outcome of pneumonia: analysis of two multicentre cohort studies. Thorax 65(10): 870-877.
-
Allard R, Leclerc P, Tremblay C, Tannenbaum TN (2010) Diabetes and the severity of pandemic influenz A (H1N1) infection. Diabetes Care 33(7): 1491-1493.
-
Ata A, Lee J, Bestle SL, Desemone J, Stain SC (2010) Postoperative hyperglycemia and surgical site infection in general surgery patients. Arch Surg 145(9): 858-864.
-
Pozzilli P, Leslie RD (1994) Infections and diabetes: mechanisms and prospects for prevention. Diabet Med 11(10): 935-941.
-
Geerlings SE, Hoepelman AI (1999) Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunol Med Microbiol 26(3-4): 259-265.
-
Fornas O, Garcia J, Petriz J (2000) Flow cytometry counting of CD34+ cells in whole blood. Nat Med 6: 833-836.
-
Baskaran K, Ahamath BK, Shanmugasundaram RK (1990) Glucose control support. Ibid 30: 295-300.
-
Clement S, Braithwaite S, Magee MF, Ahmann A, Smith EP, et al. (2004) Management of diabetes and hyperglycaemia in diabetes. Diabetes care 27 (2): 553-591.
-
Parkar MM, Humollen FL, Mahler DJ (1967) Determination of copper and Zinc in biological material. Clin Chem 13(1): 40-48.
-
Lynch TJ, Cheung WY (1979) Calcium transport by a calmodulin regulated Ca-ATPase. Arch Biochem Biophys 194: 165-172.
-
Fiske CH, Subba Row (1925) The colorimetric determination of phosphorus. J Biol Chem 66: 375- 378.
-
Butcher RW, Sutherland EW (1962) Adenosine 3', 5'- phosphate in biological materials. I. Purification and properties of cyclic 3', 5'-nucleotide phosphodiesterase and use of this enzyme to characterize adenosine 3', 5'-phosphate in human urine. J Biol chem 237: 1244-1250.
-
Ottotenghi AC (1969) Phospholipase C. Methods in Enzymology 14: 193.
-
Van Oss CJ, Gillman Cf, Neumann AW (1975) Phagocytes Engulfment and cell Adhesiveness as cellular surface pteusmere Marcel Dekker. Inc, Newyork and Basel.
-
Baehner RL, Nathan DG (1968) Quantitative Nitro Blue Tetrazolium test in chronic granulomatious disease. New Engl J Med 278(18): 971-976.
-
Paglia DE, Valentine WN (1967) Studies on the quantitative and qualitative characterization of erythrocyte glutathione peroxidase. J Lab clin Med 70(1): 158-164.
-
Strauss RR, Paul BB, Jacobs AA, Sbarra AJ (1969) Biochem Biophys 135: 265-274.
-
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, et al. (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370: 1453-1457.
-
Markhoffer W, Stein M, Maeser E, Federlin K (1992) Impairment of polymorphonuclear leukocyte function and metabolic control of diabetes. Diabetes Care 15(2): 256-260.
-
Alexiewicz JM, Kumar D, Smogorewski M, Klin M, Massry SG (1995) Polymorphonuclear leukocytes in non-insulin-dependent diabetes mellitus: abnormalities in metabolism and function. Ann Intern Med 123(12): 919-924.
-
Inoue S, Lan Y, Muran J, Tsuji M (1996) Reduced hydrogen peroxide production in neutrophils from patients with diabetes. Diabetes Res Clin Pract 33(2): 119-127.
-
Delamaire M, Maugendre D, Moreno M, Le Goff MC, Allannic H, et al. (1997) Impaired leucocyte functions in diabetic patients. Diabet Med 14(1): 29-34.
-
McManus LM, Blood RC, Prihoda TJ, Blodgett JL, Pinckard RN (2001) Agonist-dependent failure of neutrophil function in diabetes correlates with extent of hyperglycemia. J Leukoc Biol 70(3): 395-404.
-
Komura T, Sakai Y, Honda M, Takamura T, Matsushima K, et al. (2010) CD14+monocytes are vulnerable and functionally impaired under endoplasmic reticulum stress in patients with type 2 diabetes. Diabetes 59(3): 634-643.
-
Geisler C, Almdal T, Bennedsen J, Rhodes JF, Klendorf K (1982) Monocyte functions in diabetes mellitus. Acta Pathol Microbiol Immunol Scand C 90(1): 33-37.
-
Wierusz-Wysocka H, Wysocki H, Siekierka H, Wykretowicz A, Szczepanik A, et al. (1987) Evidence of polymorphonuclear neutrophil activation in patients with insulin-dependent diabetes mellitus. J Leuk Biol 42(5): 519-523.
-
Descamps-Latscha B, Nguyen AT, Feutren G (1990) Phagocyte oxidative metabolism in cyclosporine- or placebo-treated patients with insulin-dependent (type 1) diabetes mellitus of recent onset. J Autoimmun 3(2): 201-213.
-
Andrews T, Sullivan KE (2003) Infections in patients with inherited defects in phagocytic function. Clin Microbiol Rev 16(4): 597-621.
-
Tebbs SE, Gonzalez AM, Wilson RM (1991) The role of aldose reductase inhibition in diabetic neutrophil phagocytosis and killing. Clin Exp Immunol 84(3): 482-487.
-
Patti ME, Corvera S (2010) The role of mitochondria in the pathogenesis of type 2 diabetes. Endocr Rev 31(3): 364-395.
-
Falagas ME, Kompoti M (2006) Obesity and infection. Lancet Infect Dis 6(7): 438-446.
-
Tanaka S, Isoda F, Ishihara Y, Kimura M, Yamakawa T (2001) T lymphopaenia in relation to body mass index and TNF-alpha in human obesity: adequate weight reduction can be corrective. Clin Endocrinol 54(3): 347-354.
-
O'Rourke R, Kay T, Scholz M, Diggs B, Jobe B, et al. (2005) Alterations in T-cell subset frequency in peripheral blood in obesity. Obes Surg 15(10): 1463- 1468.
-
Tong Q, Dalgin G, Xu H, Ting CN, Leiden JM, et al. (2000) Function of GATA transcription factors in preadipocyte-adipocyte transition. Science 290(5489): 134-138.
-
Menghini R, Marchetti V, Cardellini M, Hribal ML, Mauriello A, et al. (2005) Phosphorylation of GATA2 by Akt increases adipose tissue differentiation and reduces adipose tissue-related inflammation: a novel pathway linking obesity to aterosclerosis. Circulation 111(15): 1946-1953.
-
Post RL, Sen AK (1967) [116] Sodium and Potassium stimulated ATPase. Methods in Enzymology 10: 762- 768.
-
Parker JC (1971) Ouabair - insensitive effects of metabolism onion and water content of red blood cells. Am J physiol 221: 338.
-
Murphy E, Coll K, Richy TL, Williamson J (1980) J Biol Chem 255: 6600-6606.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey