Subvalvular Aortic Valve Abscess Causing Atrioventricular Abnormalities, Fever of Unknown Origin and Deteriorating Dyspnea: A Case Report
Background: We report the case of an infective endocarditis of a native aortic valve that, along with the vegetations of the aortic cusps, caused a massive subvalvular abscess. Clinically was manifested by dyspnea, persisting fever, symptoms of heart failure and atrioventricular conduction abnormalities, which in the acute setting led to the implantation of a dual chamber permanent pacemaker. Case summary: The patient was a 77-year old male, who had undergone routine dental procedures during the summer and was ultimately referred to our emergency department due to recurrent febrile episodes and progressively worsening exertional dyspnea. After a number of medical consultations, he was administered many different empirical antibiotic combinations, mainly targeting a possible lower respiratory infection, based on the patient’s known smoking-induced COPD. Both the initial transthoracic and the subsequent transoesophageal echocardiographic reports in our establishment, revealed vegetations on the calcified cusps of a stenosed aortic valve, along with a large, drained cavity at the level of the sinuses of Valsalva. The most probable diagnosis was that of an endocarditis-induced subvalvular aortic root abscess. Discussion: Persistent fever, fulfilling the criteria of the notorious fever of unknown origin, should always raise the alarm about the need of a cautious approach and in-depth evaluation of the patient’s history, clinical presentation, laboratory abnormalities, and imaging results. Empirical antibiotic combinations should not be the go-to solution, especially when dealing with a known valvulopathy and newly appearing electrocardiographic abnormalities. In such cases, clinical suspicion of infective endocarditis should be high. Most importantly, when permanent intracardiac devices are planned to be implanted, special attention to excluding sources of bacteraemia must be given. Imaging plays an irreplaceable role, with TOE generally setting the diagnosis while modern imaging techinques such as Cardiac 64-slice CT and 18F-FDG PET/CT-scan can be of great assistance in future.
Introduction
Infective endocarditis is an infection of the inner surface of the heart, most frequently involving the valves. Symptoms include fever, hemorrhagic rash (e.g. Janeway lesions), Roth’s spots on the retina, new-onset of heart murmurs, anemia and generalised malaise. Acute valvular regurgitation and subsequent heart failure, embolic stroke and acute kidney failure can be some of the complications of the disease. The most commonly involved microorganisms are of the streptococcal and staphylococcal species. Risk factors for its appearance include pre-existing valvular disease, congenital heart disease, the presence of artificial valves, hemodialysis, intravenous drug use and also, pacemaker devices and indwelling venous catheters. Based on the well known Duke criteria, diagnosis depends on blood cultures, clinical presentation and echocardiographic (transthoracic and transoesophageal) imaging.
Case Presentation
An 77-year-old male patient was transported to the emergency room department with progressively deteriorating despnea and a two-month history of mostly afternoon fever. His medical history included hypertension, chronic obstructive pulmonary disease due to smoking, Aortic Valve stenosis (Calcified Aoritc cusps), Parkinson’s disease, hyperuricemia and a history of Deep Vein Thrombosis in the left leg with the diagnosis of thrombophilia as a result of mutation on factor V Leiden. The patient had undergone a denstal surgery involving implantation of dental implants 4 months ago, a recent dual-chamber pacemaker implantanion (50 days ago) and a coronary angiography (29 days ago) that revealed a severe stenosis (90%) in the Left Circumflex coronary artery and was performed in the setting of the patient’s workup for the aortic valve replacement. At the time of admission, the patient was hemodynamically stable (Blood Pressure: 117/74mmHg, peripheral capillary oxygen saturation- SpO2 89%, Heart Rate 104 beats per minute) and with a body temperature of 37,8 C. Clinical assessment affirmed signs of possible underlying heart failure. Indeed the patient was tachypnoeic with Respiratory rate of 18 breaths per minute. Ascultation of lung fields revealed mild rales in the basilar portion of the lungs. Cardiac sounds were audible, with the presence of an S3 sound. New onset of holodiastolic murmur at Aortic valve level, along with the pre -existing crescendo systolic one were also important findings. Jugular pressure was elevated but no swelling of lower limbs was obvious. The standard 12-lead electrocardiogram showed sinus rhythm with sinus tachycardia at 104 beats per minute. Chest X-ray was pathognomonic of COPD.
Blood tests displayed anemia and thrombocytopenia with elevated markers of infection (elevated CRP value, leukocytosis). Myocardial enzymes were also elevated (high- sensitive cardiac Troponin-T=111pg/ml) together with NT- ProBNP=11793pg/ml.
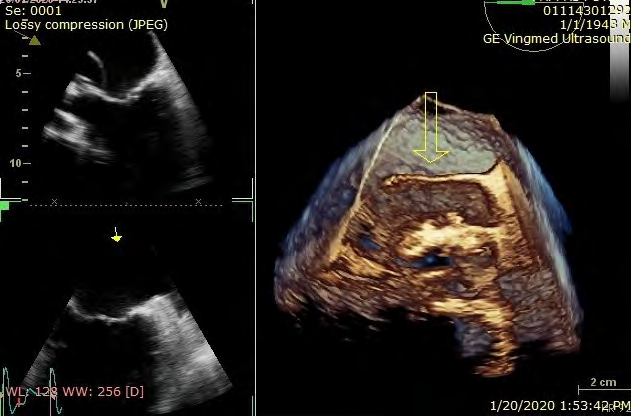
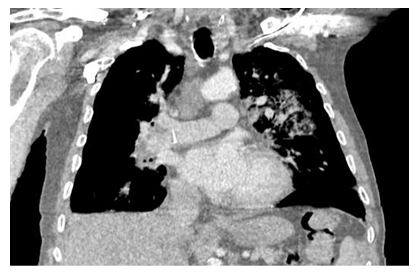
Several samples of blood amd urine cultivations were taken and the patient was treated with empirical intravenous antibiotics. He was then taken to the echocardiography laboratory where Transthoracic Echocardiography (TTE) brought to light the presence of a large cavity presenting subvulvularly at Aortic valve level. Doppler colour flow imaging exposed mixed Aortic valve disease with both severe Stenosis and Regurgitation (Figures 1-4) . The next day Transesophageal Echocardiography (TOE) affirmed the original findings (Figures 5,6,) and the 3D Echocardiography demonstrated the Aortic Abscess clearly (Figure 7). Ct Scan highlited similar results (Figure 8).
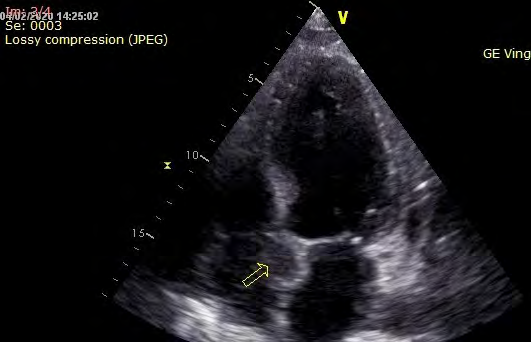
After the completion of the antibiotic treatment, a surgical intervention was decided. The TOE in the operation confirmed the findings from the previous examinations depicting the Aortic abscess and a barely functional aortic valve. The patient was submitted to a typical median sternotomy. Firstly, large pleural effusions were detected and drained. The procedure was performed under moderate hypothermia (30oC) cardiopulmonary bypass with the implementation of bi-caval and ascending aorta cannulation, venting of the heart through right superior pulmonary vein, administration of antegrade and retrograde cardioplegia. After the aortotomy, an almost destroyed non-functional triscupid aortic valve with the presence of extensive vegetations was found and removed totally. Subsequently, the abscess was clearly evident in close proximity to the aortic annulus and it was expanding just above the mitral valve without signs of any contact. The abscess was drained and samples for cultivations were received, (the cultivations were negative as a result of long term antibiotic therapy). All the necrotic or infected tissues were carefully removed. Fortunately, there was no fistula between the cardiac chambers and a primary closure with stitches and without a patch involvement was possible. A bioprothesis was chosen for the aortic valve replacement. When the replacement was completed, the cables of the pacemaker were removed through an incision in the right atrium. Finally the subcutaneous pacemaker implant was also removed and the procedure was completed uneventfully. The function of the bioprothesis was checked with the TOE and it was satisfactory enough, the heart contractility was improved and there were no findings suggesting the presence of residual cavity or fistula.
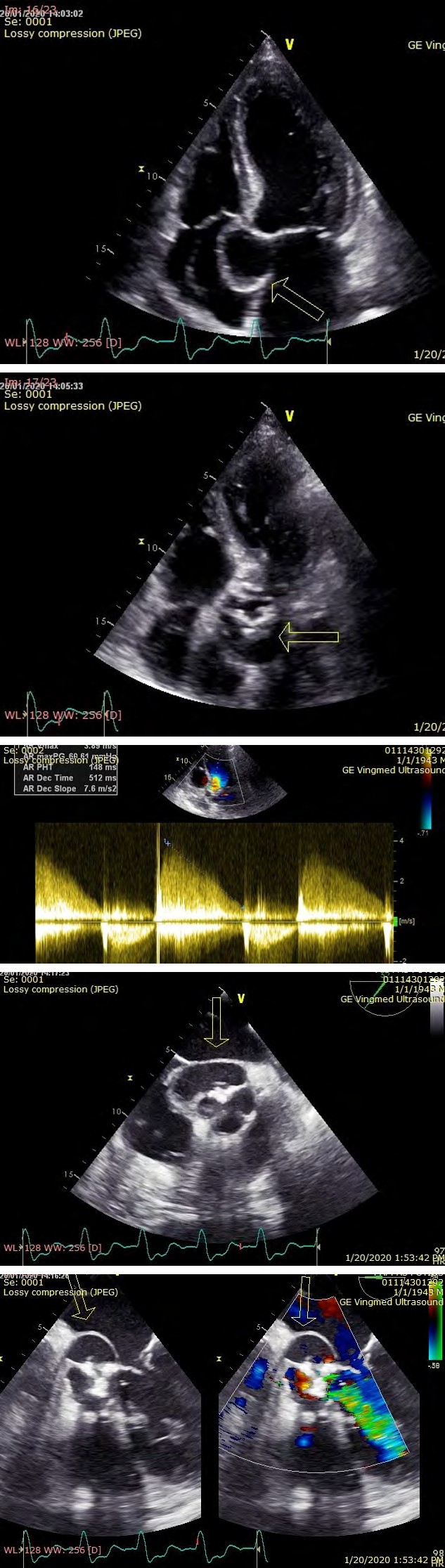
Figures 1,2: TTE Apical Four Chamber Views showing the Subvalvular Aortic Root abscess (arrows)
Figure 3,4: TTE Doppler Colour Flow Imaging revealing both severe Aortic Valve Stenosis (first image) and severe Aortic Valve Regurgitation (second image)
Figure 5,6: TOE Transesophageal views at 0 (first image) and at 52 degrees (second image) with the presence of the Aortic abscess (marked with arrows)
Discussion
Infective endocarditis (IE) complicated with aortic valve abscess can be a life-threatening condition. Careful clinical examination with a well recorded medical history can help physicians to suspect this medical entity before devastating complications appear. Clinical suspicion for IE increases in the presence of predisposing cardiac conditions, new or changing murmurs, bloodstream infection, clinical evidence of embolic phenomena, and evolving heart failure or certain other hemodynamic abnormalities. Chest x-ray, electrocardiogram, blood tests, echocardiography and computed tomography (CT) can help in early diagnosis. It is of critical importance that any electrocardiographic abnormalities (e.g. any level of atrioventricular conduction block) are not undervalued. Clinicals need to be aware in order to put the diagnosis of Infective endocarditis as soon as possible because early diagnosis and medical/ surgical treatment have significantly better clinical outcomes for the patients. Optimal cooperation between medical fields and different specialties is critical for every day practice [1].
The global burden of disease due to IE is so far not known, so further studies need to be developed therefore. A nationwide retrospective study from Netherlands that was carried out by Mr Van den Brink and his colleagues between 2005 and 2011 with a total of 5,213 patients hospitalized for IE (mean age, 67.5 years; 70% male) revealed that almost all (91%) had positive cultures, mostly for staphylococcal or streptococcal species [2].
Native valve IE was predominant (72%), followed by prosthetic valve endocarditis (21%) and pacemaker or ICD IE (7%). IE manifests with definite vegetations most commonly in the mitral valve position (41%), followed by the aortic valve position (38%), the tricuspid valve position (12%) and pulmonary valve position (1%) [3]. The second most common native valve lesion predisposing to IE is aortic regurgitation after mitral regurgitation which associated with mitral valve prolapse [3]. In case series of confirmed aortic valve IE, bicuspid aortic valve (BAV) is relatively common (16% to 43%) and in patients older than 65 years of age aortic stenosis is seen as the aortic valve lesion in IE at a rate 28% [4, 5, 6]. Our patient presented with symptoms of heart failure due to mixed valvular aortic regurgitation and stenosis and presence of subvalvular aortic valve abscess, findings that justify the presence of persistent fever and need for surgical intervention (Figures 1-7) [1].
Cardiac troponins are often seen elevated in IE. In our case high-sensitive cardiac troponin-T was 111pg/ ml at admission, whereas his peak value was 699 pg/ml.
Lab tests returned to normal values gradually after the surgery. Elevation of myocardial enzymes is most commonly associated with myocardial injury due to myocardial abscess or embolic infarction or septicemia. Ventricular wall stress in the case of heart failure is another possible mechanism. An increase in troponin-I level greater than 0.4ng/mL has been found to notably affect the risk of in-hospital mortality and need for early valve replacement [7]. A subset analysis of the ICE-PCS cohort study demonstrated that in patients with IE, a troponin-T level of 0.08ng/mL or higher was affiliated with increased risk of cardiac abscess, central nervous system events, and death IE [8].
Due to the close proximity of the atrioventricular node and the proximal intraventricular conduction system to the aortic valve and root, this location is the most common cause of new atrioventricular block (AVB) of any grade or block branch block (BBB). For this reason, our patient in the beginning presented 3d type AVB. In these cases the incidence of AVB ranges from 10% to 20%, whereas new BBB occurs in approximately 3%. The occurrence of a new conduction abnormality also is a multivariate risk predictor for death associated with IE [9, 10, 11].
Imaging always plays an important role in the diagnosis of IE. TEE has a reported sensitivity of 80% to 90%, specificities of greater than 90%, with positive and negative predictive values in the range of 85% to 90% for the diagnosis of perivalvular extension. Cardiac 64-slice CT and 18F-FDG PET/CT-scan have been shown to be an accurate alternative imaging procedure for the evaluation of IE and perivalvular extension of infection. In a small group of patients with suspected IE, cardiac CT was 96% sensitive for the detection of valvular vegetations, identical in this respect to multiplane TEE, in comparison with surgery [1, 12].
Conclusion
We would suggest CT-scan or Positron emission tomography with 2- deoxy-2-[fluorine-18]fluoro-D-glucose integrated with computed tomography (18F-FDG PET/ CT-scan) in patients with high clinical suspicion of IE presented and initial negative results in TEE with any level of AV conduction abnormalities before the implantation of permament pacemaker.
References
-
Habib G, Patrizio Lancellotti, Manuel J Antunes, Bongiorni MG, Casalta JP, et al. (2015) 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC) Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). European Heart Journal 36(44): 3075-3128.
-
Van den Brink FS, Swaans MJ, Hoogendijk MG, Alipour A, Kelder JC, et al. (2017) Increased incidence of infective endocarditis after the 2009 European Society of Cardiology guideline update: a nationwide study in the Netherlands. Eur Heart J Qual Care Clin Outcomes 3(2): 141-147.
-
Murdoch DR, Corey GR, Hoen B, Miró JM, Fowler VG Jr, et al. (2009) Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch Intern Med 169(5): 463-473.
-
Tribouilloy C, Rusinaru D, Sorel C, Thuny F, Casalta JP, et al. (2010) Clinical characteristics and outcome of infective endocarditis in adults with bicuspid aortic valves: A multicentre observational study. Heart 96(21): 1723-1729.
-
Kahveci G, Bayrak F, Pala S, Mutlu B (2009) Impact of bicuspid aortic valve on complications and death in infective endocarditis of native aortic valves. Tex Heart Inst J 36(2): 111-116.
-
Durante-Mangoni E, Bradley S, Selton-Suty C, Tripodi MF, Barsic B, et al. (2008) Current features of infective endocarditis in elderly patients: Results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch Intern Med 168(19): 2095-2103.
-
Tsenovoy P, Aronow WS, Kopacz MS (2009) Patients with infective endocarditis and increased cardiac troponin I levels have a higher incidence of in-hospital mortality and valve replacement than those with normal cardiac troponin I levels. Cardiology 112(3): 202-204.
-
Stancoven AB, Shiue AB, Khera A, Pinkston K, Hashim IA, et al. (2001) Association of troponin T, detected with highly sensitive assay, and outcomes in infective endocarditis. Am J Cardiol 108(3): 416-420.
-
Benito N, Miro J, de Lazzari E, Cabell CH, del Río A, et al. (2009) Health care-associated native valve endocarditis: Importance of nonnosocomial acquisition. Ann Intern Med 150(9): 586-594.
-
Lopez J, Revilla A, Vilacosta I, Villacorta E, González- Juanatey C, et al. (2007) Definition, clinical profile, microbiological spectrum, and prognostic factors of early-onset prosthetic valve endocarditis. Eur Heart J 28(6): 760-765.
-
Graupner C, Vilacosta I, San Roman JA, Ronderos R, Sarriá C, et al. (2002) Periannular extension of infective endocarditis. J Am Coll Cardiol 39(7): 1204-1211.
-
Feuchtner GM, Stolzmann P, Dichtl W, Schertler T, Bonatti J, et al. (2009) Multislice computed tomography in infective endocarditis. J Am Coll Cardiol 53(5): 436-444
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey