Quaint Partners: Pheochromocytoma and Sealed Duodenal Perforation
Introduction: A pheochromocytoma is a rare Ecatecholamine producing adrenal tumor. Pheochromocytoma, along with duodenal perforation is a unique combination. Case summary: A 40 year’s male presented with abdominal pain for the last month. He also had history of episodic headache, flushing and palpitation. The patient was further evaluated, Blood and urine metanephrines were found to be elevated, and radiological studies were suggestive of Right Adrenal mass 8x7 cms. After optimization, he was considered for surgery. Along with Right adrenal mass, one sealed perforation .75x.75 cms was seen in the first part of duodenum with scarring and minimal spillage. Excision of right adrenal mass along with duodenal ulcer perforation closure with an omental flap was done. The histopathology was suggestive of pheochromocytoma. The histopathology of the duodenal ulcer margin was suggestive of chronic inflammation and scarring in duodenal tissue. Conclusion: Pheochromocytoma is a great masquerader. The pheochromocytoma association with a duodenal ulcer is more than a coincidence. Phaeochromocytoma should always kept in mind in atypical cases of abdominal pain
Introduction
A pheochromocytoma is a rare, catecholamine- secreting tumor derived from chromaffin cells. The term phaeochromocytoma (in Greek, phios means dusky, chroma means color, and cytoma means tumor) refers to the color the tumor cells acquire when stained with chromium salts. It presents with headache, palpitations, hypertension, etc [1]. It has atypical presentations in 9-10%, which often delay diagnosis [2]. We report a case of sealed duodenal perforation detected during surgery for the excision of pheochromocytoma. The clinical, biochemical, radiologic, and pathologic description of the case has been described below.
Case Summary
A 40 year’s male presented with abdominal pain, dyspepsia, and hypertension for the last one month. He also had a history of episodic headache, flushing, and palpitation for the last six months. The patient was a known case of gastritis on pantoprazole. On examination, mild tenderness was present in the epigastrium. The patient was having tachycardia 110/min, and blood pressure was 160/110 mmHg. Routine blood investigations were Hb 11.5 gm%, TLC 8900, Urea 35, creatinine 1.1, chest X-ray normal. The patient was suspected for pheochromocytoma; hence urine metanephrines were done. Urine metanephrines were found to be elevated significantly. CECT scan showed a heterogeneous smooth-surfaced right adrenal mass (8x7 cm) with high HU 40 with an intense enhancement of intravenous contrast injection with early washout (Figures 1 & 2). The patient was started on phenoxybenzamine. After achieving adequate alpha blockade, he was considered for surgery. Intraoperative blood pressure fluctuated during operation and managed by intravenous vasodilators. On exploration, adhesions were encountered during the kocherisation of the duodenum. Along with Right adrenal mass, one sealed perforation .75x.75 cm was seen in the first part of duodenum with scarring and minimal spillage. Excision of right adrenal mass along with duodenal ulcer perforation closure with an omental flap was done (Figures 3 & 4). The histopathology was suggestive of phaeochromocytoma. The histopathology of the duodenal ulcer margin was suggestive of chronic inflammation and scarring in duodenal tissue (Figure 5).
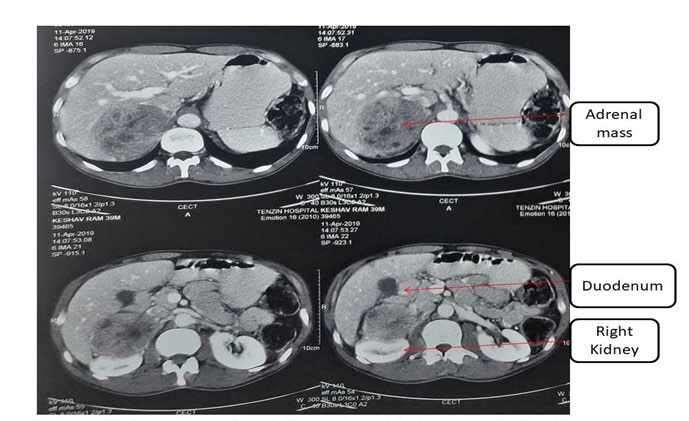
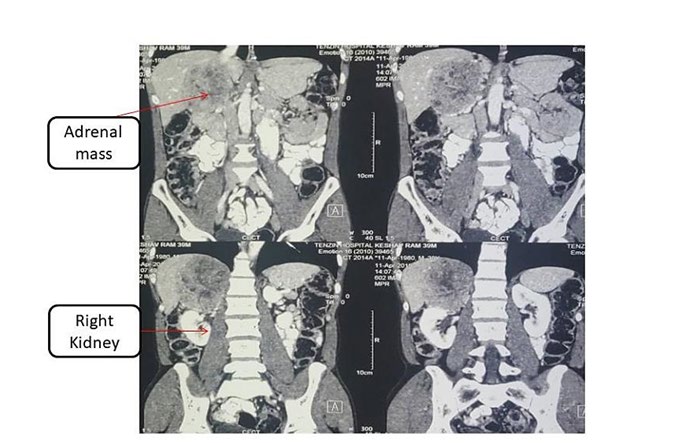
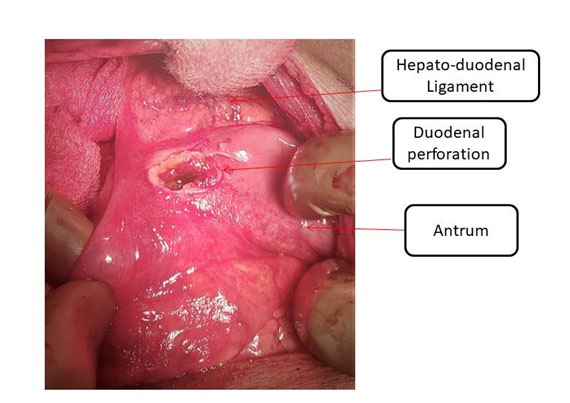
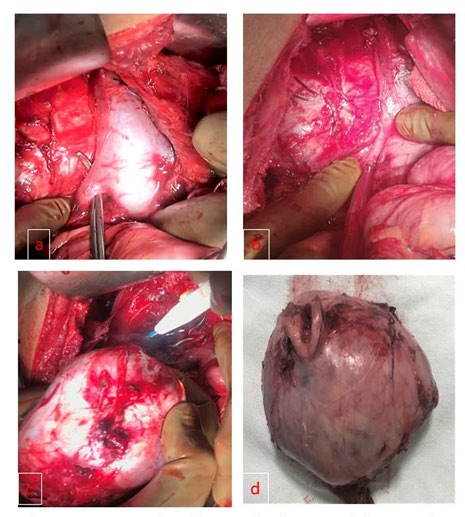
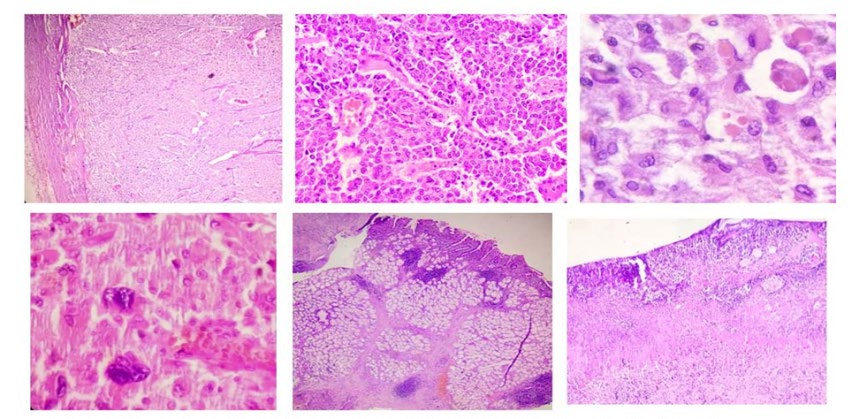
Figure 5: A Well encapsulated lesion with nests of tumor cells separated by fibrovascular septae(Zallballen pattern).(scanner view), B. Round to oval tumor cells with mild pleomorhism, stippled chromatin, moderate to abundant granular eosinophilic cytoplasm with indistinct cell borders. (High power view). C. Tumor cells with intracytoplasmic hyaline globules (High power view). D. Another field showing bizzare tumor gaint cells. E-F. Fragment of duodenal mucosa showing denudation of epithelium, lamina propria showing marked chronic inflammatory infiltrate(lymphocytes and plasma cells).
Discussion
Approximately 10% of phaeochromocytoma and 35% of extra-adrenal pheochromocytomas are malignant. Although the majority of pheochromocytomas are sporadic, about 30% result from inherited mutations [1]. Among the features that suggest a malignant course are large tumor size and an abnormal DNA ploidy pattern (aneuploidy, tetraploidy). The diagnosis of malignant pheochromocytomas is by metastasis, but pathology and local invasion are also helpful [3]. The triad of headache, sudden, episodic perspiration, and tachycardia is a classic hallmark of pheochromocytoma. Epigastric pain, flank pain, constipation are unusual symptoms of pheochromocytoma.
Pheochromocytoma should be suspected if a patient has episodic, paroxysmal symptoms of headache, palpitation and headache [4]. Pheochromocytoma diagnosed by plasma metanephrines, urine metanephrines (more specific). Radiologic studies CECT and MRI are mainstay to delineate anatomic details, in addition PET scan for non-visualized tumors [1]. Surgical resection is treatment of choice and virtually cures the disease. Adequate and effective preoperative blockade of alpha and beta receptors is must to decrease complications.
Pheochromocytoma rarely presents as abdominal pain, may be result of associated musculoskeletal pain, gastritis, cholelithiasis, intestinal colic etc. Pheochromocytoma causes increases in catecholamines, which has minimal influence on pepsin, acid secretion. In literature, only 2 cases have reported pheochromocytoma with gastric ulcer perforation [5, 6]. In a case report, pheochromocytoma presents with dyspepsia in one case and flank pain in another patient [7]. The pathophysiology of duodenal perforation in phaeochromocytoma is unclear. However, bowel vasoconstriction, increased secretion of acid secondary to catecholamine’s appears to be causative.
The association could also be a coincidence as other factors associated with gastritis like a middle-aged man with smoking history from the middle class were present in our patient. The patient also had a history of NSAIDS intake for generalized ache. Detailed pathophysiology of phaeochromocytoma is not clear, so clear association could not be established. In atypical setting we should always keep phaeochromocytoma in differential diagnosis of abdominal pain.
Conclusion
Phaeochromocytoma is a great masquerader. The phaeochromocytoma association with a duodenal ulcer is not reported before. The association of duodenal ulcer and phaeochromocytoma is more than a coincidence. Phaeochromocytoma should always kept in mind in atypical cases of abdominal pain.
References
-
Waguespack SG, Rich T, Grubbs E, Ying AK, Perrier ND, et al. (2010) A current review of the etiology, diagnosis, and treatment of pediatric pheochromocytoma and paraganglioma. J Clin Endocrinol Metab 95(5): 2023- 2037.
-
Rupala K, Mittal V, Gupta R (2017) Atypical presentation of pheochromocytoma: Central nervous system psedovasculitis. Indian J Urol 33(1): 82-84.
-
Thompson LD (2002) Pheochromocytoma of the Adrenal gland Scaled Score (PASS) to separate benign from malignant neoplasms: a clinicopathologic and immunophenotypic study of 100 cases. Am J Surg Pathol 26(5): 551-566.
-
Young WF (1993) Pheochromocytoma:1926-1993. Trends Endocrinol Metab 4(4): 122-127.
-
Sportiello V (1984) Gastric ulcer associated with malignant pheochromocytoma: coincidence or correlation. Minerva Endocrinol 9(1): 49-50.
-
Sigal ES (1986) Perforated gastric ulcer in pheochromocytoma. Klin Med (Mosk) 46(3): 133-134.
-
Rajendra B, Ranjeeth A, Patne P (2014) Unusual presentation of pheochromocytoma. Journal of scientific society 41(2): 136-139.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey