Omphalocele with Hypoalbunemia and Testicular Torsion
An Omphalocele is a birth defect in which an infant’s intestine or other abdominal organs are outside of the body because of a hole in the belly button (navel) area. The intestines are covered only by a thin layer of tissue and can be easily seen. Infants with an Omphalocele often have other birth defects. Defects include genetic problems (chromosomal abnormalities), congenital diaphragmatic hernia, and heart and kidney defects. These problems also affect the overall outlook (prognosis) for the baby’s health and survival the condition looks like gastroschisis. An Omphalocele is a birth defect in which the infant’s intestine or other abdominal organs protrude through a hole in the belly button area and are covered with a membrane. In gastroschisis, there is no covering membrane Omphalocele occurs in 1 in 4,000 births and is associated with a high rate of mortality (25%) and severe malformations, such as cardiac anomalies (50%), neural tube defect (40%), exstrophy of the bladder and Beckwith–Weidman syndrome. Approximately 15% of live-born infants with Omphalocele have chromosomal abnormalities. About 30% of infants with an Omphalocele have other congenital abnormalities.
Risk Factor
1-Old women age 2-Multipara, many deliveries
Causes
Omphalocele is caused by malrotation of the bowels while returning to the abdomen during development. Some cases of Omphalocele are believed to be due to an underlying genetic disorder, such as Edward’s syndrome (trisomy 18) [1, 2] or Patau syndrome (trisomy 13). Beckwith–Weidman syndrome is also associated with Omphalocele.
Occurrence
The Centres for Disease Control and Prevention (CDC) estimates that each year about 775 babies in the United States are born with an omphalocele. In other words, about (3) out of every 5,386 babies born in the United States each year is born with an Omphalocele. Many babies born with an Omphalocele also have other birth defects, such as heart defects, neural tube defects, and chromosomal abnormalities [3].
Our Case
Full term delivered by Cererian section due to previous cecerain baby cried immediately with Apgar score 8-9-9, transferred to NICU ,intubated and covered the intestine by sterile gauze .there was history of polyhydraminase in the mother ,no chronic illness
On Examination
No dimorphic feature, weight is 3kg. Vital signs were stable, blood gas was good 1st and 2nd heart sound was normal Scaphoid abdomen all intestine and liver outside covered by sterile gauze. She was conscious Saw by pediatric surgery prepared for operation
Investigation
1) CBC within normal 2) Chemistry normal apart from albumin which was very low 3) Echo Cardiogram was done normal 4) Chromosomal analysis was sent 5) Coagulation profile was sent 6) Saw by genetic consultant waiting for chromosomal analysis.
Course and Prognosis
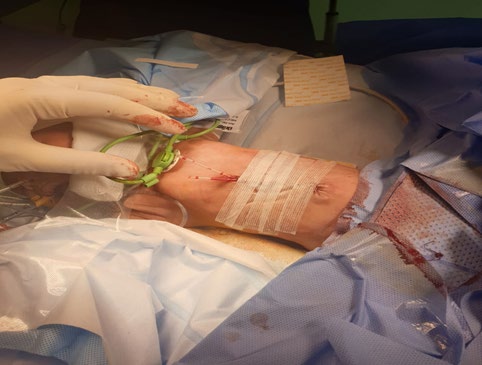
Pediatric surgery tried to made reduction maneuver slowly with observation of vital signs and blood pressure and pulses of lower limb to avoid compartment syndrome Baby doing fine. Kept NPO with TPN Infusion on Mechanical ventilator on 3rd day baby became edematous with swelling of both testes saw by peadiasurgery to rollout torsion. Urgent Doppler ultrasound done blood flow is normal, albumin was very low, and so he received albumin transfusion.

On 6th day general condition is stable followed by pedia surgery took him for complete reduction of Omphalocele if passible Baby came from operation, vital signs were stable on Mechanical ventilation, NPO on TPN Infusion on vancomycin and Meropenam. 3rd day postoperative baby running fever septic workup done blood culture showed staph epidermis continuous antibiotic, chromosomal was normal.

Conclusion
Omphalocele is an emergency case must be attendance in operation room with senior qualified neonatologist and surgeon must be informed from 1st hour of life the defect must be cover by sterile gouse and elective intubation if the defect compromised the respiratory condition the parents have to informed and consoling them about the abnormalities associated with Omphalocele like chromosomal abnormalities and others abnormalities We have to differentiate between gastroschisis and Omphalocele [4].
| Gastroschisis | Omphalocele | |
|---|---|---|
| Location | Right of umbilicus | Umbilicus |
| Sac | No | Yes (may be ruptured) |
| Contents | Small intestine/colon | Liver, intestine, spleen, gonads |
| Etiology | Failure of umbilical coelom development→rupture | Failure of lateral folds |
| Associated anomalies | Intestinal atresia (mechanical) | Chromosomal, cardiac, pulmonary hypoplasia |
| Outcomes | Good (as long as not significant bowel loss) | Dependent upon size and associated anomalies |
Table 1: Congenital Abdominal Wall Defects.
In summary, an Omphalocele or gastroschisis are congenital defects of the anterior abdominal wall. An Omphalocele arises within the umbilical ring as a central defect, while a gastroschisis involves the base of the umbilical stalk, with the defect in the abdominal wall always occurring lateral to the umbilicus. Although the diagnosis of both types is frequently made antenatal by ultrasound, if missed, they are readily apparent after delivery in the delivery room, where striking differences between the two are obvious. Although the survival rate of patients with abdominal wall defects has gradually improved, the outcome is largely dependent on coexisting anomalies. Although surviving children without severe congenital anomalies have a good quality of life, late surgical problems are seen, and close follow-up is essential to good outcome.
Follow up
Baby brought to OPD, he was 3month old gaining weight, tolerate feeding passed stool normal, on breast feeding and artificial.
Conflict of interest: Dr: Najia alhojaili declare that they have no conflict of interest
Compliance with Ethical standards
Human and Animal Right no human or animal research was conducted by the authors for this literature review Informed consent: This paper did not include the collection or analysis of data. Accordingly there is no requirement for review.
References
-
Kanagawa SL, Begleiter ML, Ostlie DJ, Holcomb G, Drake W, et al. (2002) Omphalocele in three generations with autosomal dominant transmission. J Med Genet 39(3): 184-185.
-
Yatsenko SA, Mendoza-Londono R, Belmont JW, Shaffer LG (2003) Omphalocele in trisomy 3q: further delineation of phenotype. Clin Genet 64(5): 404-413.
-
Parker SE, Mai CT, Canfield MA, Rickard R, Wang Y, et al. (2010) Updated national birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol 88(12): 1008-1016.
-
Stoll C, Alembik Y, Dott B, Roth MP (2008) Omphalocele and gastroschisis and associated malformations. Am J Med Genet A 146A(10): 1280-1285.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey