Idiopathic Scrotal Calcinosis: A Case Report
Idiopathic scrotal calcinosis is a subtype of calcinosis cutis characterized by the deposition of calcium and phosphorous in the scrotal skin in the absence of systemic disorders. Idiopathic calcinosis is described in a varying location like the scrotum, penis, breast, vulva, etc. In most cases, diagnosis is made by clinical diagnosis. Secondary investigations need to identify any other associated systemic etiology for the disease. Surgical excision is the recommended treatment for idiopathic scrotal calcinosis. Most of the cases may not recur following surgical excision.
Introduction
Calcinosis cutis is an abnormal condition characterized by the deposition of calcium in the skin and subcutaneous layer. Idiopathic scrotal calcinosis is a subtype of calcinosis cut is characterized by the deposition of calcium and phosphorous in the scrotal skin in the absence of systemic disorders. In most of the cases, it is idiopathic and, in some cases, it is due to dystrophic calcification of pre-existing disease [1]. It is a subtype of calcinosis cutis. It is more common around the middle age group.
Case Report
A 40 years old male patient presented with a complaint of multiple nodules in the scrotum of 2 years duration. The nodule was initially small in size and progressively increased in size. The nodule was initially soft in nature and later it becomes harder. The nodule doesn’t have any specific complaints except cosmetic appearance. The patient denied a history of sexually transmitted disease, trauma, surgery, and inflammation. There is no history of similar lesions elsewhere in the body. There is no history of previous surgery or prolonged medications. There is no history suggestive of hypercalcemia of malignancy elsewhere in the body. Local examination shows multiple greyish-white nodules present in the scrotum (Figure 1). The nodule is firm to hard inconsistency. There is no evidence of inflammation, discharge, and induration (Figure 2).


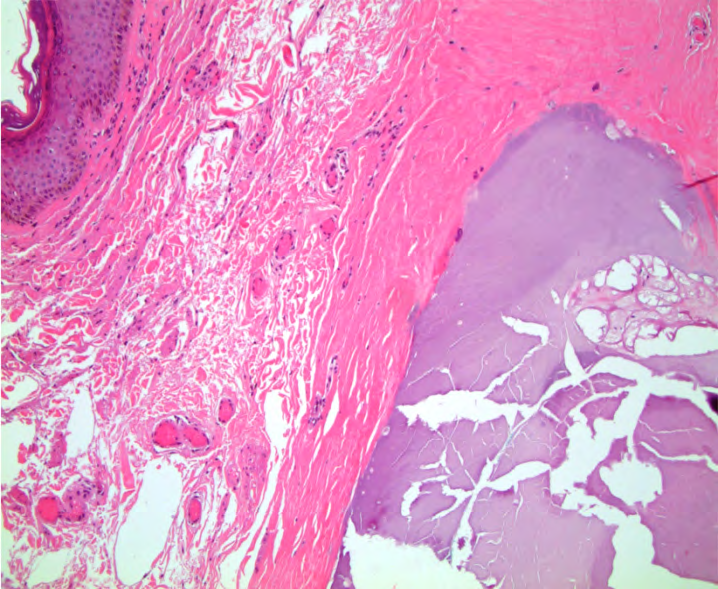
The lesion is excised under local anesthesia using an elliptical incision. The lesion is excised above the dartous muscle and wound closed in layers. Post-operative histopathology examination confirms the diagnosis of scrotal calcinosis (Figure 3). Histology shows wide areas of calcification within the connective tissue. There is no evidence of any other gland or cyst. There is no evidence of malignancy. The patient is followed up for more than 3 years without any evidence of recurrence.
Discussion
Calcinosis cutis is classified into dystrophic, metastatic, iatrogenic, calciphylaxis, and idiopathic based on the etiology of calcification. Idiopathic calcinosis is described in a varying location like the scrotum, penis, breast, vulva, etc [2].
Possible pathogenesis for idiopathic calcinosis cutis is
- Calcification following trauma,
- Calcification of existing epidermal cyst,
- Dystrophic calcification of scrotal skin.
The most commonly proposed hypothesis is constant friction allows extravasation of tissue calcium leads to dystrophic calcification in scrotal calcinosis. Another possible etiology is dystrophic calcification of epidermal cyst, epithelial cyst, eccrine duct, etc [3]. In non-idiopathic scrotal calcinosis is associated with a metabolic disorder, autoimmune disorder, and malignant disease [4].
In idiopathic scrotal calcinosis, there is no identifiable local or systemic cause. In most cases idiopathic scrotal calcinosis is asymptomatic and rarely does it present with itching and pain. Infection of the idiopathic scrotal calcinosis is rare [5]. The rare differential diagnosis of idiopathic scrotal calcinosis is multiple calcified sebaceous cysts of the scrotum.
In the gross picture, the important clinical feature is 1. In most cases it is multiple 2. It never involves penis skin [6]. it shows as greyish- white granular growth, it is usually around 300-400 in number, firm to hard in consistency, with or without discharge. If discharge occurs, it mostly looks like a chalky white in nature. In most of the cases, the penis is not involved. The size of nodules varies from 0.5 cm to a maximum of 3 cm.
In most cases, diagnosis is made by clinical diagnosis. Secondary investigations need to identify any other associated systemic etiology for the disease. In all cases, screening is done serum calcium, phosphorus, parathyroid hormone, serum vitamin D level, uric acid, alkaline phosphatase, cholesterol profile. In fine needle aspiration cytology shows hypocellular irregular crystals.
In macroscopic cut, the section shows a white color or yellow color nodule. Histopathology shows the following classical findings.
- Presence of calcium deposit in the dermis layer.
- Presence of multinucleated giant cells.
- The absence of the epithelial lining. presence of calcium deposit in the dermis layer.
It also shows amorphous basophilic materials surrounded by foreign body giant cells. Von Kossa’s stain shows dark color materials within the nodules confirms calcium deposits [7].
Surgery is the recommended treatment of choice. Primary excision above the dortas muscle is the accepted treatment of choice for idiopathic scrotal calcinosis. Idiopathic scrotal calcinosis can be solitary or multiple [8]. Solitary lesion needs local excision, whereas multiple lesions required en bloc resection with reconstruction. The incidence of recurrence following surgical excision is rare.
Conclusion
Idiopathic scrotal calcinosis is one of the differential diagnoses of multiple scrotal nodules which is a chalky white in nature. Most of the cases don’t associate with identifiable local or systemic causes. Surgical excision is the recommended treatment for idiopathic scrotal calcinosis. Most of the cases may not recur following surgical excision.
References
-
Khallouk A, Yazami OE, Mellas S, Tazi MF, el Fassi J, et al. (2011) Idiopathic Scrotal Calcinosis: A Non-Elucidated Pathogenesis and Its Surgical Treatment. Rev Urol 13(2): 95-97.
-
Pompeo A, Molina WR, Pohlman GD, Sehrt D, Kim FJ (2013) Idiopathic scrotal calcinosis: A rare entity and a review of the literature. Can Urol Assoc J J Assoc Urol Can 7(5–6): E439-441.
-
Yuyucu Karabulut Y, Kankaya D, Şenel E, Dölek Y, Uslu A, et al. (2015) Idiopathic scrotal calcinosis: the incorrect terminology of scrotal calcinosis. G Ital Dermatol Venereol 150(5): 495-499.
-
Parlakgumus A, Canpolat ET, Caliskan K, Colakoglu T, Yildirim S, et al. (2008) Scrotal calcinosis due to resorption of cyst walls: a case report. J Med Case Reports 2: 375.
-
Killedar MM, Shivani AA, Shinde U (2016) Idiopathic Scrotal Calcinosis. Indian J Surg 78(4): 329-330.
-
Tareen A, Ibrahim RM (2018) Idiopathic scrotal calcinosis - A case report. Int J Surg Case Rep 44: 51-53.
-
Dubey S, Sharma R, Maheshwari V (2010) Scrotal calcinosis: idiopathic or dystrophic?. Dermatol Online J 16(2): 5.
-
Akinboro AO, Onilede DA, Babatunde TO, Oiwoh SO, Suleiman OA, et al. (2018) Idiopathic scrotal calcinosis: report of 2 cases, and review of pathogenesis and factors that determine patients’ acceptance of surgical treatment. Clin Cosmet Investig Dermatol 11: 333-337.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey