Evaluation of a Life Functioning Goal Attainment Psychosocial Treatment Program for Adults with Psychotic Disorders
Purpose: To determine if the use of an integrated goal attainment cognitive behavioral social skill training program can impact serious mental illness related treatment and life functioning avolition. Methods: The attendance and goal attainment progress of thirty-eight serious mental ill diagnosed adults admitted to psychiatric clinic’s integrated goal attainment cognitive behavioral social skills group training program were studied. Demographic (age, gender, race, education), clinical (psychiatric diagnosis, trauma history), and life experience (work, income, housing, relational status, friendship support, incarceration and drug arrest histories) variables were compared to identify possible program attendance and goal attainment level associations and differences. Results: Participants attended a mean of 8 program days of the 6 to 8-week program with younger and unmarried attending significantly more days than older and married participants. Greater attendance and participation rates were positively correlated with higher levels of assessed goal attainment. Conclusions: Individuals with serious mental illness conditions are likely to voluntarily attend and participate in psychosocial intervention programs focused on major area life functioning goal attainment. Higher levels of attendance and participation were associated with higher levels of short-term goal attainment. Functioning focused psychosocial interventions may be effective in reducing serious mental illness related avolition.
Abbreviations
SMI: Serious Mental Illness; CBSST: Cognitive Behavioral Social Skills Training; CBT: Cognitive Behavioral Therapy.
Introduction
Serious mental illness (SMI) related avolition, the “lack of interest or engagement in goal-directed behavior”, has been identified as the central factor contributing to deficits Investigation Paper in social interactions, affective expression, experienced pleasure, cognitive decision making, and levels of major life area functioning including work, interpersonal relations, academic pursuits, and self-care [1, 2, 3, 4]. A primary component of avolition is believed to be the abnormal white matter connectivity in motivation-related circuits resulting in an impaired connection between action (behavior) and outcome (effect) and a diminished interest in and motivation for setting and pursuing goals [5, 6, 7, 8].
Avolition and its’ negative symptom and deficit functioning tributaries has been attributed to hypofunctionality of dopamine D1 receptor neurotransmission (i.e., low level dopamine activity) in the prefrontal cortex [9]. Positive symptoms of SMI psychotic conditions have been attributed to hyperactivity of dopamine D2 receptor neurotransmission in subcortical and limbic brain regions (i.e., high level activity). Treatment of psychotic conditions is primarily focused on reducing disturbing positive symptoms (e.g., delusions, hallucinations, disorganized speech, and grossly disorganized or catatonic behavior) usually with an activity level reducing dopamine agonist agent. Dopamine agonist medications are believed to increase avolition largely through reducing the cognitive capacity to learn new associations and the motivation reducing blockade of the mesolimbic reward system [10]. While medication induced lower levels of dopamine activity may increase avolition- related functioning disabilities, avolition, usually the first symptom of psychosis, generally precedes the introduction of dopamine agonist agents [2]. Increasingly there is a push to look beyond dopamine agonist antipsychotic medication in addressing serious mental illness related avolition [11, 12].
Increased SMI-related avolition and associated disabling functioning and decreased dopamine level activity have been associated with experiencing behaviorally disconnecting stressful events such as childhood sexual abuse, traumatic occurrences, racial discrimination, significant losses, social defeat, and stigmatization, and chronic psychosocial adversity/stress [13, 14, 15, 16, 17, 18]. Chronic variable stress disrupts reward processing by altering the attribution of incentive to associated cues impairing the function of multiple brain regions and causing a range of severe hedonic and motivational deficits [19]. It is hypothesized that SMI vulnerable recipients of confusing, non-contingent negative occurrences learn events happen in their lives independent of their behavior, i.e., there is an action – outcome disconnect, that leads to a lack of self-efficacy and cognitive defeatist functioning beliefs [20]. There are efforts to address these avolition-related beliefs through the development of specialized interventions [21, 22, 23, 24]. The belief that SMIs are incurable, irreversible conditions may contribute to defeatist beliefs about recovery and improved functioning among recipients, family members, and providers of psychiatric treatment services [25, 26].
Manifestations of avolition in psychiatric service delivery include low, participation, and sustained involvement in clinical treatment settings, reduced goal-directed pursuit, and low major life area attainment and maintenance levels [27, 28]. Individuals with SMI conditions, especially when combined with substance use, contact with the criminal justice system, and minority status, have observed higher rates of treatment non-attendance, non-adherence, and drop-out, and lower rates of attained and sustained major life area functioning [29].
Though there appears to be no available treatment for avolition and other negative symptoms that have reached the threshold for robust clinically meaningful improvement Fusar-Poli P, et al. [30], major life functioning goal focused treatment, combined with recovery oriented, person- centered approaches that recognize and remediate goal interfering factors have shown promise in significantly reducing behavioral manifestations of avolition, including treatment disengagement and related negative symptoms [31, 32, 33, 34, 35, 36, 37, 38]. Approaches including behavioral activation, motivational interviewing, supportive employment and housing, social/relationship enhancement, cognitive and behavioral remediation and skill approaches have been shown to be effective in decreasing avolition and improving major life area behavioral functioning with individuals diagnosed with SMI conditions [39, 40, 41, 42].
This report describes the development, utilization, and preliminary effectiveness of a person resiliency focused, behavioral goal attainment intervention program for individuals diagnosed with avolition related SMI conditions
Materials and Methods
Program Description: The intervention program is a modified version of the Cognitive Behavioral Social Skills Training (CBSST) program [43]. Instead of one weekly in- person group session, the modified program included four 50-minute virtual group sessions per week over six-to-eight weeks. Each weekly group session focused on one of the social, cognitive, or problem-solving CBSST skill modules or a fourth goal attainment module developed specifically for this program. All group sessions were conducted virtually using a secure Zoom telehealth platform. The groups consisted of one-to-five participant group members and a minimum of two, but usually three participant facilitators (one of whom is the identified primary group leader). Group participant facilitators were individuals trained or actively being trained in providing humanistically applied adaptive functioning- oriented interventions.
Resiliency and Recovery Focus
The modified CBSST program incorporated a recovery/ growth framework. Each person, no matter the title or facilitator or participant role, functioned as a non-hierarchical member in the group, engaging in activities, role plays, and exercises, sharing personal challenges and successes, giving and receiving feedback and suggestions for improvement, and completing out-of-group (homework) assignments. All group members were considered and interacted with as “normal” (no matter the given diagnosis or ascribed pathology) and their thoughts, feelings, and behaviors were considered understandable responses to their current and historical situations, circumstances, experiences, stressors, traumas, conditions, exposures, and environments. Individuals were understood in terms of their personal frame of reference. The groups were run using a strengths- based, positively valued, non-judgmental approach with a particular emphasis on identifying things that were working well and using things not working well as opportunities for improvement. Ascribing negative terms like “wrong”, “bad”, “terrible” or attributing problems to a “mental illness” was avoided.
Emphasis on Adaptive Behavioral Functioning Goal Attainment
The modified CBSST program focused on adaptive functioning goal attainment and emphasized adaptive skill mastery. Each group session sought to help participants utilize a specific skill that could assist with achieving their personal goals. Each participant was introduced to ways to more effectively and efficiently perform skill sets and independently practice and use each improved skill set in everyday living. During each group session a practically useful skill was introduced and practiced, followed by assigned practice the skill “homework” in a non-clinical, natural environment. Each module’s skill set was broken down into small, progressive steps, e.g., the goal attainment step of being able to make a realistic, achievable goal preceded the next step of identifying someone to speak with about specific strategies to achieve the goal.
Goal Attainment Skills
The Goal Attainment Skills module’s focused on helping participants develop and work towards attaining an adaptive behavioral functioning goal. At least one short-term (6-week) goal, aligned with a long-term (6-month) goal was developed for both group participants and facilitators. Developed goals were encouraged to be within adaptive major life area- oriented functioning (e.g., work/employment, housing, family/friend relationships, school/training, enjoyment/ fun, or self-care domains) instead of problem-oriented focused domains (e.g., feel less depressed, stop hearing voices …). The “SMART” goal framework was utilized to help participants develop goals that are specific, measurable, achievable, relevant (meaningful), and time-bound [44]. Each participant’s 6-week and 6-month goals became the focus of all the groups within the modified CBSST program.
The 11 step Goal Attainment Scaling worksheet (starting at step zero - “Thinking about setting a goal”- and ending at step ten - “Maintain/exceed target goal”- was used to promote goal attainment [45]. Each Goal Attainment session introduced and provided examples of one-to-two of the steps, and then individualized support, coaching and guidance were provided in virtual breakout sessions during the group session time.
Cognitive Skills
The Cognitive Skills Module focused on teaching strategies for identifying and examining unhelpful thoughts, and generating alternative, more helpful thoughts. Group members were introduced to the general concepts of cognitive behavioral therapy (CBT), including the relationship between thoughts, actions, and feelings (generic cognitive model), automatic thoughts, thought challenging through behavioral experiments and examining evidence for beliefs, and identifying thinking traps. This module includes the “3C’s” cognitive approach: Catch It, Check It, and Change It (“It” is an unhelpful thought). The cognitive skills group addressed defeatist functioning beliefs that interfered with or prevented participants from attaining their goals.
Social Skills
The Social Skills Module focused on ways to improve communication and relational skills through teaching and practicing active listening, expressing positive and negative feelings, and making positive requests. Many of the role plays emphasized interacting with other people who could help group members attain their goals.
Problem-Solving Skills
Basic problem-solving skills were taught using the acronym SCALE-– Specify the problem, consider all possible solutions, Assess the best solution, lay out a plan, and Execute and Evaluate the outcome. The focus was on developing specific, feasible plans to solve real-world problems that were interfering with group members attaining their goals.
Participants
Participants were 37 individuals being treated for psychotic featured involved SMI conditions in an urban setting adult outpatient behavioral health clinic who agreed to participate in the modified CBSST program between July 2020 through January 2022.
Table 1 displays demographic, clinical, and life- experience information about the study sample. Participants were between 20 and 70 years old with a mean age of 35.51. About half were women (51.4%): the majority were Black/ African American (78.4%); about half had some post-high school education (51.4%); close to half had been diagnosed with Schizophrenia (48.6%) with other participants diagnosed with either Schizoaffective Disorder (29.7%) or a primary mood disorder (21.6%); more than half self- reported previously experienced trauma (62.2%); most were not working (89.2%), lived with other people (64.9%), single (86.5%), reported having no friends (56.8%), and had been incarcerated in the past (59.5%; only 24.3% had been arrested for a drug-related crime). About half of the participants received some type of income (48.6%) primarily through being Social Security Disability Insurance (SSDI) benefit recipients.
Study Procedures
This study was a retrospective chart review of the electronic medical records of the identified 37 program participants. Only the participation data for the first cohort in which an individual participated was examined. There were no exclusion criteria for this study. This study was approved by the Emory University Institutional Review Board (study #00004553).
Measures
Demographics
Each participant’s electronic behavioral health assessment record was reviewed to access reported age at the time of program participation, gender, race, and educational status. For some analyses, age was dichotomized into either 18-34 years and 35 or more years and educational status dichotomized into either 12th grade or less and post-high school higher education.
Clinical Variables
Each participant’s electronic psychiatric assessment was reviewed to access the primary psychiatric diagnosis, and the behavioral health assessment was reviewed to obtain the presence of a self-reported trauma history.
Life Experience Variables
Each participant’s electronic behavioral health assessment was reviewed to access the presence of self- reported work, income and income source, housing (categorized as living alone or living with other people), relationship (categorized as single/divorced/separated or married/partnered), friendship support (categorized as having no friends or one or more friend/s), incarceration history, and drug arrest history statuses.
Program Attendance
Each participant’s electronic group progress notes were reviewed to calculate attendance (the total number of days attended).
Goal Progress Ratings
Each participant’s electronically recorded goal attainment note was reviewed to obtain facilitator accessed highest level of goal attainment ratings.
Data Analysis
Data were entered into IBM SPSS Statistics (Version 28). Descriptive statistics were examined, and data were assessed for outliers and non-normality using histograms and scatterplots. Since the continuous variables were not normally distributed and the sample size was low, non- parametric tests were used. There was no missing data to account for in the dataset.
To examine differences in demographic, clinical, and life experience variables between those who attended at least one day and those who did not attend at all, the Mann- Whitney U test was used for continuous variables and the Fisher’s exact test was used for categorical variables due to small sample sizes and expected low cell counts. Since the Fisher’s exact test can only be used with 2X2 contingency tables, when examining differences between those who attended and those who did not attend, Schizophrenia and Schizoaffective Disorders were combined and compared to stand alone Mood Disorders [46].
To examine whether program attendance (a continuous variable) varied by demographic, clinical, and life experience variables, the Mann-Whitney U test was utilized for dichotomized categorical variables and the Kruskal- Walli’s test was utilized for greater than two categorical variables.
To determine the association between program attendance and goal attainment progress level, Spearman’s correlation coefficient was calculated.
Results
Preliminary Analyses: From July 2020 through January 2022, 37 people were scheduled to participate in at least one cohort of the modified CBSST program. The means, standard deviations, and frequencies for the study variables of the 37 individuals scheduled to participate in the modified CBSST program are displayed in Table 1. The only significant variable difference between the 30 individuals who attended at least one day and the 7 individuals who agreed to participate but never attended was those who attended were younger (M = 33.37 years old) than those who did not attend (M = 44.71), U = 44.50, p < .05.
| Total | CBSST Participants | No Shows | ||||
|---|---|---|---|---|---|---|
| Measure | (n = 37) | (n = 30) | (n = 7) | |||
| Mean (SD) | Frequency (%) | Mean (SD) | Frequency (%) | Mean (SD) | Frequency (%) | |
| Demographics | ||||||
| Age | 35.51 (12.11) | 33.37 (11.45)* | 44.71 (11.15)* | |||
| Gender | ||||||
| Man | 18 (48.6) | 15 (50.0) | 3 (42.9) | |||
| Woman | 19 (51.4) | 15 (50.0) | 4 (57.1) | |||
| Race | ||||||
| Black/African American | 29 (78.4) | 23 (76.7) | 6 (85.7) | |||
| White/Caucasian | 8 (21.6) | 7 (23.3) | 1 (14.3) | |||
| Educational Status | ||||||
| 12th Grade or Less | 18 (48.6) | 13 (43.3) | 5 (71.4) | |||
| More than 12th Grade | 19 (51.4) | 17 (56.7) | 2 (28.6) | |||
| Clinical Variables | ||||||
| Diagnosis† | ||||||
| Schizophrenia | 18 (48.6) | 14 (46.7) | 4 (57.1) | |||
| Schizoaffective Disorder | 11 (29.7) | 8 (26.7) | 3 (42.9) | |||
| Mood Disorder | 8 (21.6) | 8 (26.7) | 0 (0.0) | |||
| Trauma History | ||||||
| Previous Trauma | 23 (62.2) | 19 (63.3) | 4 (57.1) | |||
| No Previous Trauma | 14 (37.8) | 11 (36.7) | 3 (42.9) | |||
| Life Experience Variables | ||||||
| Work Status | ||||||
| Working | 4 (10.8) | 3 (10.0) | 1 (14.3) | |||
| Not Working | 33 (89.2) | 27 (90.0) | 6 (85.7) | |||
| Current Income Status | ||||||
| Income | 18 (48.6) | 14 (46.7) | 4 (57.1) | |||
| No Income | 19 (51.4) | 16 (53.3) | 3 (42.9) | |||
| SSDI Income Status | ||||||
| SSDI Income | 16 (43.2) | 13 (43.3) | 3 (42.9) | |||
| No SSDI Income | 21 (56.8) | 17 (56.7) | 4 (57.1) | |||
| Housing Status | ||||||
| Live Alone | 13 (35.1) | 8 (26.7) | 5 (71.4) | |||
Note: N = 37. SD = Standard deviation. *Statistically significant difference at p < .05. †Due to small sample sizes, when examining differences between CBSST participants and individuals who did not attend the program, Schizophrenia and Schizoaffective Disorders were combined and compared to Mood Disorders. Table 1: Means, Standard Deviations, and Frequencies for Study Variables.
The average number of days attended for the 30 individuals who attended at least one day was 5.57 (SD = 4.99). The only significant variable differences found among those who attended at least one day were younger participants (i.e., those 18-34 years old) attended more program days (M = 8.42) than older participants (35-70 years old; M = 4.18), U = 47.00, p < .05, and single participants attended more program days (M = 7.62) than married participants (M = 2.00), U = 12.00, p < .05 Table 2.
| Mean (SD) | |
|---|---|
| Demographics | |
| Age | |
| 18-34 Years Old | 8.42 (4.57)* |
| 35-70 Years Old | 4.18 (3.54)* |
| Gender | |
| Man | 7.73 (4.61) |
| Woman | 6.00 (4.69) |
| Race | |
| Black/African American | 6.78 (4.66) |
| White/Caucasian | 7.14 (4.98) |
| Educational Status | |
| 12th Grade or Less | 7.08 (5.30) |
| More than 12th Grade | 6.71 (4.25) |
| Clinical Variables | |
| Diagnosis | |
| Schizophrenia | 7.21 (5.21) |
| Schizoaffective Disorder | 7.63 (4.03) |
| Mood Disorder | 5.50 (4.47) |
| Trauma History | |
| Previous Trauma | 6.26 (4.70) |
| No Previous Trauma | 7.91 (4.59) |
| Life Experience Variables | |
| Work Status | |
| Working | 4.67 (2.08) |
| Not Working | 7.11 (4.81) |
| Current Income Status | |
| Income | 7.36 (5.14) |
| No Income | 6.44 (4.30) |
| SSDI Income Status | |
| SSDI Income | 7.62 (5.44) |
| No SSDI Income | 6.29 (4.03) |
| Housing Status | |
| Live Alone | 6.63 (4.34) |
| Live with Others | 6.95 (4.85) |
| Relationship Status | |
| Single/Separated/Divorced | 7.62 (4.53)* |
| Married or Partnered | 2.00 (1.15)* |
| Friendship Support Status | |
| 1 or More Friends | 5.69 (4.55) |
| No Friends | 7.76 (4.66) |
| Drug Arrest History | |
| Previous Drug Arrest | 6.14 (4.41) |
| No Previous Drug Arrest | 7.09 (4.80) |
| Incarceration History | |
| Jail/Prison History | 6.31 (4.48) |
| No Jail/Prison History | 7.50 (4.93) |
Note: N = 30. SD = Standard deviation. *Statistically significant difference at p < .05. Table 2: Number of Program Days Attended Across Demographic, Clinical, and Life Experience Variables.
Primary Analysis
Twelve individuals attended one-to-four program days, seven people attended five-to-eight program days, six people attended nine-to-twelve program days, and five people attended thirteen-to-sixteen program days Table 3.
| Number of Program Days Attended | Total Number of Participants (%) |
| 0 | 7 (18.9%) |
| 4-Jan | 12 (32.4%) |
| 8-May | 7 (18.9%) |
| 12-Sep | 6 (16.2%) |
| 13-16 | 5 (13.5%) |
Table 3: Total number of program days attended by CBSST participants in their first cohort from July 2020 through January Note: N
Five of the 30 individuals who attended groups never developed short or long-term goals (usually because they attended only one goal attainment group where ratings were made). Most of the 25 individuals who did develop goals chose a primary goal related to work followed by self-care Table 4.
| Adaptive Functioning Goal Area | Total Number of Participants (%) |
|---|---|
| Work | 10 (40%) |
| Self-Care | 8 (32%) |
| Education/Training | 3 (12%) |
| Family/Friend Relationships | 3 (12%) |
| Housing | 1 (4%) |
| Enjoyment/Fun | 0 (0%) |
Table 4: Adaptive Functioning Goal Areas Selected by Program Participants.
Note: N = 25. Table 4: Adaptive Functioning Goal Areas Selected by Program Participants.
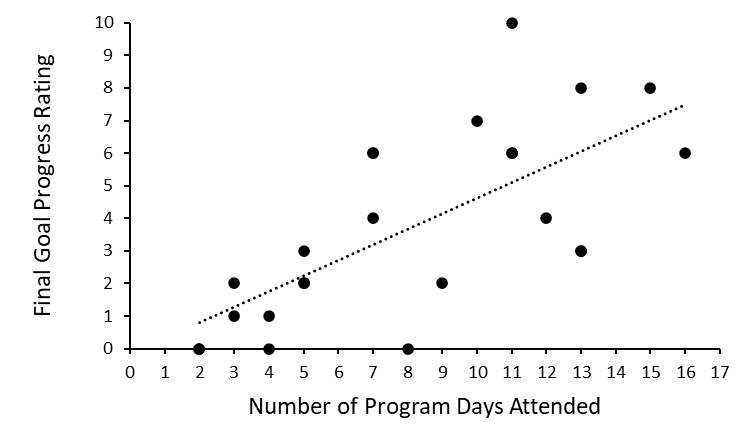
Six of the 30 individual who attended a minimum of one group never received the first goal progress rating which usually occurred during the second goal attainment group day which occurred on the program’s third group day. The average final goal progress level rating received by the 24 program participants was 3.75 (SD = 2.92). Spearman’s correlation between the number of program days attended and each participant’s final goal progress rating was statistically significant, rs = 0.73, p < .05. This represents a large effect size, and a scatterplot of the data is presented in Figure 1.
Discussion
This study demonstrated individuals living with serious mental illness-related avolition can voluntarily engage, identify meaningful short-term functioning goals, and progress towards attaining those goals in an intense, recovery-oriented goal attainment cognitive-behavioral social skills group intervention program. Given that the sample population was largely made up of individuals least likely to participate (adhere or comply) in outpatient psychiatric treatment, e.g., young, Black, men, schizophrenia spectrum diagnosed, with limited education and income, and histories of traumatic, significant substance use, and forensic incarcerations, our findings suggest there are promising avolition penetrating psychosocial approaches that facilitate interest and engagement in functional goal-directed behavior, even among individuals generally considered to be unlikely goal attainment participants.
The higher than literature reported group attendance rates and goal attainment progress with study participants may be attributable to: 1) the intervention focus on attaining personally desired functioning goals (a hope and success ability orientation); not restraining disruption management and control approaches frequently employed with individuals with serious mental illness conditions, 2) normalizing experiences as extensions of shared challenge-facing cognitive, emotional, and behavioral coping efforts; not abnormal indications and symptoms of circumstance-independent illness conditions unique to too often stigmatized individuals with serious mental illness conditions, and 3) using intensively delivered, merged evidence-based interventions that enable individuals to actively improve their skills in handling goal attainment interferers Rao KN, et al. [47]; not hierarchically delivered, anti-motivating approaches frequently focused on externally controlling problematic, disruptive functioning. The higher participation and associated goal step-level attainment with younger individuals in this study may indicate individuals with earlier stages of SMI conditions may be more receptive to and desirous of non-pathological, personal functioning goal-oriented interventions.
This study has confidence limitations in the generalizability of its’ findings. Study limitations include: 1) being a retrospective chart review study with no matched control group anchoring between group comparisons; 2) all study measures were within group comparisons with other comparisons inferred from variable factors and reports in the general psychiatric literature; i.e. treatment (usually meaning prescribed medication) nonadherence and dropout rates ranging from 25% to 90%, with lower treatment nonadherence and dropout rates with some psychosocial interventions Villeneuve K, et al. [48]; 3) measured goal attainment levels were assessed by group leader clinicians and based on each individual’s reported step progress (homework) and accomplishments at the conclusion of each weekly goal attainment group – not independently assessed by trained assessors using standardized measures or instruments; 4) the study sample size was small limiting statistical power; 5) the study sample primarily consisted of public-sector funded, inner-city residing, lower socio- economic status (SES) individuals who may have different responses to treatment interventions than individuals with demographically, socially, and co-occurring condition differences usually associated with higher SES individuals Bennett D, et al. [49]; and 6) levels of avolition and related “negative symptoms” were inferred from psychiatric intervention attendance and participation, goal attainment, and major social factor functioning, not standardized recovery oriented avolition/volition (amotivation/motivation) outcome measures [50, 51]. Another limitation to this study is its’ focus on factors associated with treatment engagement and initiating and improving a level of a major area of life functioning; it did not look at some of the important and needed standard behavioral healthcare outcome indicators including symptom, overall functioning, and quality of life measures.
Conclusion
This record review observational study showed that the implementation of an intensive, goal attainment cognitive- behavioral social skills program can begin breaking avolition’s lack of interest or engagement in goal-directed behavior with individuals with serious mental illness conditions. Individuals with debilitating avolition-related major life functioning deficits can be facilitated to create realistic functioning goals and engaged in the behavioral process of functioning goal attainment. These findings suggest the adjunctive use of functional goal oriented psychosocial interventions can improve major life area functioning and decrease negative symptomatology lack of functioning for individuals with serious mental illness conditions.
References
-
Strauss GP, Bartolomeo LA, Harvey PD (2021) Avolition as the core negative symptom in schizophrenia: relevance to pharmacological treatment development. NJP Schizophr 7(1): 16.
-
Correll CU, Schooler NR (2020) Negative Symptoms in Schizophrenia: A Review and Clinical Guide for Recognition, Assessment, and Treatment. Neuropsychiatr Dis Treat 16: 519-534.
-
Messinger JW, Trémeau F, Antonius D, Mendelsohn E, Prudent V, et al (2011) Avolition and expressive deficits capture negative symptom phenomenology: implications for DSM-5 and schizophrenia research. Clin Psychol Rev 31(1): 161-168.
-
(2013) Diagnostic and Statistical Manual of Mental Disorders. 5th (Edn.), American Psychiatric Association, USA, pp: 992.
-
Amodio A, Quarantelli M, Mucci A, Prinster A, Soricelli A, et al. (2018) Avolition-Apathy and White Matter Connectivity in Schizophrenia: Reduced Fractional Anisotropy Between Amygdala and Insular Cortex. Clin EEG Neurosci 49(1): 55-65.
-
Strauss GP, Whearty KM, Morra LF, Sullivan SK, Ossenfort KL, et al. (2016) Avolition in schizophrenia is associated with reduced willingness to expend effort for reward on a Progressive Ratio task. Schizophr Res 170(1): 198-204.
-
Barnes SA, Der-Avakian A, Markou A (2014) Anhedonia, avolition, and anticipatory deficits: assessments in animals with relevance to the negative symptoms of schizophrenia. Eur Neuropsychopharmacol 24(5): 744- 758.
-
DeRosse P, Barber AD, Fales CL, Malhotra AK (2019) Deconstructing Avolition: Initiation vs persistence of reward-directed effort. Psychiatry Res 273: 647-652.
-
Toda M, Abi-Dargham A (2007) Dopamine hypothesis of schizophrenia: making sense of it all. Curr Psychiatry Rep 9(4): 329-336.
-
Begemann MJH, Thompson IA, Veling W, Gangadin SS, Geraets CNW, et al. (2020) To continue or not to continue? Antipsychotic medication maintenance versus dose-reduction/discontinuation in first episode psychosis: HAMLETT, a pragmatic multicenter single- blind randomized controlled trial. Trials 21.
-
Gomes FV, Grace AA (2021) Beyond Dopamine Receptor Antagonism: New Targets for Schizophrenia Treatment and Prevention. Int J Mol Sci 22(9): 4467.
-
Fervaha G, Foussias G, Agid O, Remington G (2015) Motivational deficits in early schizophrenia: prevalent, persistent, and key determinants of functional outcome. Schizophr Res 166(1-3): 9-16.
-
Bloomfield MAP, McCutcheon RA, Kempton M, Freeman TP, Howas O (2019) The effects of psychosocial stress on dopaminergic function and the acute stress response. ELife 8: e46797.
-
Powers A, Fani N, Cross D, Ressler KJ, Bradley B (2016) Childhood trauma, PTSD, and psychosis: Findings from a highly traumatized, minority sample. Child Abuse Negl 58: 111-118.
-
Mayo D, Corey S, Kelly LH, Yohannes S, Youngquist AL, et al. (2017) The Role of Trauma and Stressful Life Events among Individuals at Clinical High Risk for Psychosis: A Review. Front Psychiatry 8: 55.
-
Der-Avakian A, Mazei-Robison MS, Kesby JP, Nestler EJ, Markou A (2014) Enduring deficits in brain reward function after chronic social defeat in rats: susceptibility, resilience, and antidepressant response. Biol Psychiatry 76(7): 542-549.
-
Varese F, Smeets F, Drukker M, Lieverse R, Lataster T, et al. (2012) Childhood adversities increase the risk of psychosis: A meta-analysis of patient control, prospective- and cross-sectional cohort studies. Schizophr Bull 38(4): 661-671.
-
Jones SR, Fernyhough C (2007) A new look at the neural diathesis--stress model of schizophrenia: the primacy of social-evaluative and uncontrollable situations. Schizophr Bull 33(5): 1171-1177.
-
Spring MG, Caccamise A, Panther EA, Windsor BM, Soni KR, et al. (2021) Chronic Stress Prevents Cortico- Accumbens Cue Encoding and Alters Conditioned Approach. J Neurosci 41(11): 2428-2436.
-
Devoe D, Cadenhead K, Cornblatt B, Granholm E, Addington J (2022) Negative symptoms: Associations with defeatist beliefs, self-efficacy, and maladaptive schemas in youth and young adults at-risk for psychosis. Behavioural and Cognitive Psychotherapy 17: 1-14.
-
Luther L, Coffin GM, Firmin RL, Bonfils KA, Minor KS, et al. (2018) A Test of the Cognitive Model of Negative Symptoms: Associations between Defeatist Performance Beliefs, Self-Efficacy Beliefs, and Negative Symptoms in a Non-Clinical Sample. Psychiatry Res 269: 278-285.
-
Campellone TR, Sanchez AH, Kring AM (2016) Defeatist Performance Beliefs, Negative Symptoms, and Functional Outcome in Schizophrenia: A Meta-analytic Review. Schizophr Bull 42(6): 1343-1352.
-
Abram SV, Weittenhiller LP, Bertrand CE, McQuaid JR, Mathalon DH, et al. (2022) Psychological Dimensions Relevant to Motivation and Pleasure in Schizophrenia. Front Behav Neurosci 16: 827260.
-
Reddy LF, Horan WP, Barch DM, Buchanan RW, Gold JM, et al. (2018) Understanding the Association Between Negative Symptoms and Performance on Effort-Based Decision-Making Tasks: The Importance of Defeatist Performance Beliefs. Schizophr Bull 44(6): 1217-1226.
-
Beck A, Rector N, Stolar N, Grant P (2009) Schizophrenia Cognitive Theory, Research, and Therapy. NY: Guilford Press, New York.
-
Knaak S, Mantler E, Szeto A (2017) Mental Illness- Related Stigma in Healthcare: Barriers to Access and Care and Evidence-Based Solutions. Healthc Manage Forum 30(2): 111-116.
-
Strauss GP, Horan WP, Kirkpatrick B, Fischer BA, Keller WR, et al. (2013) Deconstructing Negative Symptoms of Schizophrenia: Avolition-Apathy and Diminished Expression Clusters Predict Clinical Presentation and Functional Outcome. J Psychiatr Res 47(6): 783-790.
-
Schormann ALA, Buggisch S, Riehle M, Lincoln TM, Schlier B (2022) Low Goal-Directed Behavior in Negative Symptoms is explained by Goal Setting - Results of a Diary Study. J Behav Ther Exp Psychiatry 76: 101740.
-
Strassnig MT, Miller ML, Moore R, Depp CA, Pinkham AE, et al. (2021) Evidence for Avolition in Bipolar Disorder? A 30-Day Ecological Momentary Assessment Comparison of Daily Activities in Bipolar Disorder and Schizophrenia. Psychiatry Res 300: 113924.
-
Fusar-Poli P, Papanastasiou E, Stahl D, Rocchetti M, Carpenter W, et al. (2015) Treatments of Negative Symptoms in Schizophrenia: Meta-Analysis of 168 Randomized Placebo-Controlled Trials. Schizophr Bull 41(4): 892-899.
-
Haugen I, Stubberud J, Haug E, McGurk SR, Hovik KT, et al. (2022) A Randomized Controlled Trial of Goal Management Training for Executive Functioning in Schizophrenia Spectrum Disorders or Psychosis Risk Syndromes. BMC Psychiatry 22(1): 575.
-
Strauss GP, Esfahlani FZ, Sayama H, Kirkpatrick B, Opler MG, et al. (2020) Network Analysis Indicates That Avolition is the Most Central Domain for the Successful Treatment of Negative Symptoms: Evidence from the Roluperidone Randomized Clinical Trial. Schizophr Bull 46(4): 964-970.
-
Robson E, Greenwood K. (2022) Rates and Predictors of Disengagement and Strength of Engagement for People with a First Episode of Psychosis Using Early Intervention Services: A Systematic Review of Predictors and Meta-analysis of Disengagement Rates. Schizophr Bull Open 3(1): sgac012.
-
Favrod J, Nguyen A, Chaix J, Pellet J, Frobert L, et al. (2019) Improving Pleasure and Motivation in Schizophrenia: A Randomized Controlled Clinical Trial. Psychother Psychosom 88(2): 84-95.
-
Dixon LB, Holoshitz Y, Nossel I (2016) Treatment engagement of individuals experiencing mental illness: review and update. World Psychiatry 15(1): 13-20.
-
Tjaden C, Mulder CL, Hollander W, Castelein S, Delespaul P, et al. (2021) Effectiveness of Resource Groups for Improving Empowerment, Quality of Life, and Functioning of People with Severe Mental Illness: A Randomized Clinical Trial. JAMA Psychiatry 78(12): 1309-1318.
-
Wang G, Wang Y, Gai X (2021) A Meta-Analysis of the Effects of Mental Contrasting with Implementation Intentions on Goal Attainment. Front Psychol 12: 565202.
-
Granholm E, Holden J, Worley M (2018) Improvement in Negative Symptoms and Functioning in Cognitive- Behavioral Social Skills Training for Schizophrenia: Mediation by Defeatist Performance Attitudes and Asocial Beliefs. Schizophrenia Bulletin 44(3): 653-661.
-
Mueser KT, Drake RE, Bond GR (2016) Recent Advances in Supported Employment for People with Serious Mental Illness. Curr Opin Psychiatry 29(3): 196-201.
-
Chien WT, Mui JHC, Cheung EFC, Gray R (2015) Effects of Motivational Interviewing-Based Adherence Therapy for Schizophrenia Spectrum Disorders: A Randomized Controlled Trial. Trials 16: 270.
-
Killaspy H, Harvey C, Brasier C, Brophy L, Ennals P, et al. (2022) Community-Based Social Interventions for People with Severe Mental Illness: A Systematic Review and Narrative Synthesis of Recent Evidence. World Psychiatry 21(1): 96-123.
-
Grant PM, Bredemeier K, Beck AT (2017) Six-Month Follow-Up of Recovery-Oriented Cognitive Therapy for Low-Functioning Individuals With Schizophrenia. Psychiatr Serv 68(10): 997-1002.
-
Granholm EL, McQuaid JR, Holden JL (2016) Cognitive Behavioral Social Skills Training for Schizophrenia: A Practical Treatment Guide. New York: Guilford Press, pp: 322.
-
Bovend’Eerdt TJ, Botell RE, Wade DT (2009) Writing SMART Rehabilitation Goals and Achieving Goal Attainment Scaling: A Practical Guide. Clinical Rehabilitation 23(4): 352-361.
-
Tabak NT, Link PC, Holden J, Granholm E (2015) Goal Attainment Scaling: Tracking Goal Achievement in Consumers with Serious Mental Illness. American Journal of Psychiatric Rehabilitation 18(2): 173-186.
-
Field A (2013) Discovering Statistics Using IBM SPSS Statistics. 4th (Edn.), Thousand Oaks, CA: Sage.
-
Rao KN, George J, Sudarshan CY, Begum S (2017) Treatment Compliance and Noncompliance in Psychoses. Indian J Psychiatry 59(1): 69-76.
-
Villeneuve K, Potvin S, Lesage A, Nicole L (2010) Meta-Analysis of Rates of Drop-Out from Psychosocial Treatment among Persons with Schizophrenia Spectrum Disorder. Schizophr Res 121(1-3): 266-270.
-
Bennett D, Rosenheck R (2021) Socioeconomic Status and the Effectiveness of Treatment for First-Episode Psychosis. Health Serv Res 56(3): 409-417.
-
Drapalski AL, Medoff D, Unick GJ, Velligan DI, Dixon LB, et al. (2012) Assessing Recovery of People with Serious Mental Illness: Development of a New Scale. Psychiatr Serv 63(1): 48-53.
-
Raffard S, Norton J, Linden M, Lançon C, Benoit M, et al. (2022) Psychometric Properties of the BIRT Motivation Questionnaire (BMQ), a Self-Measure of Avolition in Individuals with Schizophrenia. J Psychiatr Res 147: 274-282.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey