Ventricular Tachycardia During Ajmaline Challenge
We report the case of a 63 year old woman who comes to an ajmaline challenged. After 8 minutes of infusion her baseline ECG showed significant QRS complex prolongation and switched over to the typical coved-type ECG. Subsequently a sustained monomorphic ventricular tachycardia was developed, followed by a sustained polymorphyc VT onset, which finally degenerated in a hemodynamically non relevant sustained monomorphic VT. Finally, a 200J defibrillation was required to terminate the arrythmia. Sustained ventricular arrhytmia (SVA) is infrequent but not an exceptional event (0.1-18%) and ajmaline is considered a valuable drug. In addition, provocation testing must be performed in an appropiate environment with advanced life support facilities. The evidence shows that the occurrence of ajmaline-induced sustained ventricular arryhtmia in patients with BS might not identify a category at higher risk for further arrhythmic events during follow-up.
Estrada Parra I, Pavón Jimenez R, Leal del Ojo J, Garcia Medina D,
Picon Heras R* and Pastor Torres L
Departamento de Cardiologia, Hospital Universitario Virgen de Valme, Spain
mail: rpiconh@hotmail.com required to terminate the arrythmia.
Proarrhythmia
Abbrevations: ECG: Electrocardiography; BS: Brugada Syndrome; SCB: Sodium Channel Blockers; VT: Ventricular Tachycardia; SVA: Sustained ventricular arrhytmia
Case Report
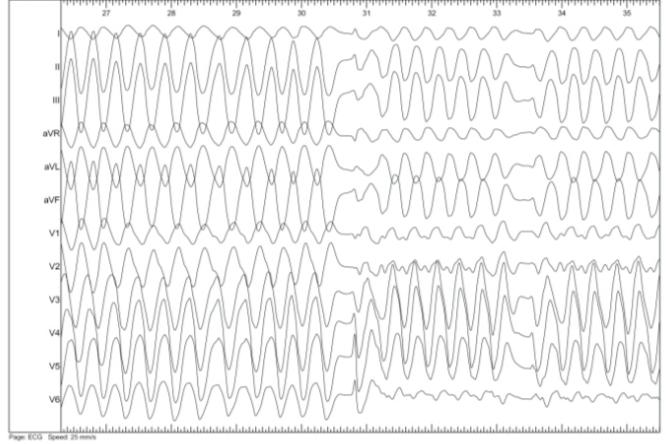
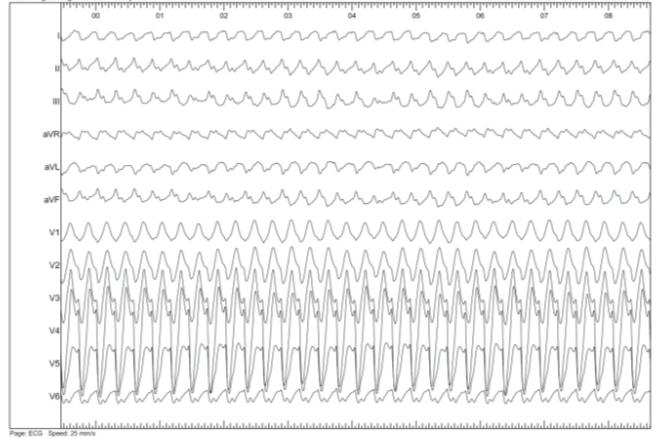
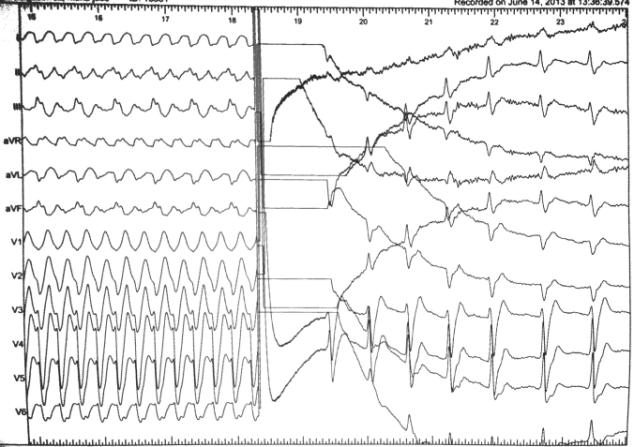
We report the case of a 63 year old woman with arterial hipertensión, who comes to an ajmaline challenged due to a family screening of Brugada syndrome after the recently diagnosis to her 29 year old song. The patient underwent ajmaline challenge and received 50mg in 10 minutes intravenous infusion, as our protocol requires (body weight 60 kg). Her baseline ECG showed a 118 ms QRS complex (Figure 1). After 8 minutes of infusion she showed significant QRS complex prolongation (174 ms) and ST elevation in the right precordial leads, which switched over to the typical coved-type ECG (Figure 2). Subsequently short-coupled ventricular extra systoles occurred and a sustained monomorphyc ventrycular tachycardia was developed, followed by a sustained polymorphyc VT onset (Figure 3), which finally degenerated in a hemodynamically non relevant sustained monomorphic VT with RBBB configuration, inferior axis and a cicle duration of 416 ms. The SMVT showed a progressive shortening until reaching a 288ms cycle duration (Figure 4). 20 minutes later, the SMVT persisted despite intravenous isoprenaline administration (2-5mcg/min). Finally, a 200J defibrillation was required to terminate the arrythmia (Figure 5).


Review
Brugada Syndrome (BS) was introduced as a clinical entity in 1992. It is defined by a characteristic electrocardiographic pattern of ST-segment elevation in right precordial leads and a high incidence of sudden death in young individuals with structurally normal hearts, which is most commonly secondary to the development of polymorphic ventricular tachycardia and fibrillation [1]. The prevalence of the disease is estimated to be 5-20 cases/10 000 [2].
Given that BS is an inherited condition, the mechanisms underlying the syndrome remain to be clarified. Several hypotheses have been proposed involving abnormalities in both repolarization and depolarization, but the same mechanism might not be responsible for the disease in all patients, and several might coexist in a single patient. Inheritance of BS occurs via an autosomal dominant mode of transmission with a low penetrance, but there are sporadic cases as well. Mutations in voltage-gated sodium channels (SCN5A), voltage-gated potassium channels (KCNE3, KCNJ8, KCND3 and KCNE) and in voltage-dependent calcium channels (CACNA1C, CACNB2B and CACNA2D1) have been linked to the síndrome [3, 4]. Current clinical guidelines and consensus documents state that BS is diagnosed in patients with ST-segment elevation with type 1 morphology ≥2mm in one or more leads among the right precordial leads V1 and/or V2 positioned in the second, third, or fourth intercostal space, occurring either spontaneously or after provocative drug testing with intra-venous administration of sodium-channel blockers. Other ECG patterns are not sufficient for the diagnosis, but the diagnostic ECG pattern can be concealed or can fluctuate between a diagnostic and a non-diagnostic pattern [5, 6]. Sodium-channel blockers had been widely used to unmask the diagnostic ECG pattern of BS in case of a non- diagnostic basal ECG, due to its availability, fast action and effectiveness, specially ajmaline, flecainide and procainamide [7]. Ajmaline has been shown to be a potent drug in unmasking the diagnostic ECG pattern of BS and is favoured compared with other sodium-channel blockers because of its short lasting half-life and its electrophysiological effects. In direct comparison with flecainide, ajmaline was superior in unmasking the diagnostic ECG pattern of BS. In a prospective study with 22 patients diagnosed with BS, the responses of the surface ECG to two different intravenously administered sodium-channel blockers (ajmaline and flecainide challenge) were investigated. In 15 of 22 patients (68%) the study revealed concordant results, but in seven patients (32%) intravenous flecainide did not produce the typical ECG changes, and they were only provoked after ajmaline infusión [8]. In a study with 147 individuals, representing 4 large families with SCN5A mutations, 104 were determined to be at possible risk for BS and underwent both genetic and electrocardiographic evaluation with ajmaline test. The sensitivity, specificity, positive and negative predictive values of the drug challenge were 80%, 94.4%, 93.3% and
82.9%, respectively [9]. Meregalli performed 160 tests with flecainide in CN5A- positive probands and their family members. The sensitivity, specificity, PPV and PNV were 77%, 80%, 96% and 36%, respectively. The greater sensitivity to ajmaline may be attributable to differences in the effectiveness of the two drugs in blocking the sodium-channel current INa at the doses used [10]. Ajmaline challenge should be developed by electrocardiography monitoring. The infusion should be discontinued when the diagnostic type I ECG pattern with ST-segment elevation greater than 0.2 mV appears in at least two right pre-cordial leads, the occurrence of PVCs or VT, prolongation of the QRS duration >130% or the occurrence of higher degree AV-block. After termination of ajmaline administration, monitoring should be continued for a minimum of 60 seconds until ST elevation returns back to baseline [11]. It is known that ajmaline challenge produces prolongation of PR, QT and QRS duration [12]. On the other hand, sustained ventricular arrhytmia (SVA) is infrequent but not an exceptional event (0.1-18%) and ajmaline is considered a valuable drug [13]. A recently review of articles published from 2000 to 2015 evaluated the incidence and predictors of SVA during sodium channel blockers (SCB) challenge. The weighted average for induction of any VA during sodium blocking challenge was 2.4%; 0.34% for non-sustained ventricular tachycardia (VT) and 0.59% for sustained VT. No fatal cases were reported. Predictors may be young age, conduction disturbance at baseline ECG, and mutations in the SCN5A gene [14].
We considered our case of special interest based on the rare occurrence of these events, highlighting possible serious complications of an already established diagnostic test
However, due to the prognostic importance, all patients with aborted sudden death or unexplained syncope without demonstrable structural heart disease and family members of affected individuals should presently undergo drug testing for unmasking BS. It can be questioned whether an SCB challenge is necessary in all asymptomatic patients with a suspicious ECG baseline or a family history of BS, considering the good prognosis of asymptomatic patients, but it seems too simple to conclude that the risk of SCB-induced arrhythmia outweighs the potential benefits. In addition, provocation testing must necessarily be performed in an appropriate environment in which advanced life support facilities are present [14]. Finally, the evidence shows that the occurrence of ajmaline-induced sustained ventricular arryhtmia in patients with BS might not identify a category at higher risk for further arrhythmic events during follow-up.
References
-
Brugada P, Brugada J (1992) Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol 20(6): 1391-1396.
-
Patel SS, Anees SS, Ferrick KJ (2009) Prevalence of a Brugada pattern electrocardiogram in an urban population in the United States. Pacing Clin Electrophysiol 32(6): 704-708.
-
Sieira J, Dendramis G, Brugada P (2016) Pathogenesis and management of brugada Syndrome. Nat Rev Cardiol 13(12): 744-756.
-
Rook MB, Bezzina Alshinawi C, Groenewegen WA, Van Gelder IC, Van Ginneken AC, et al. (1999) Human SCN5A gene mutations alter cardiac sodium channel kinetics and are associated with the Brugada syndrome. Cardiovasc Res 44(3): 507-517.
-
Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, et al. (2015) ESC Guidelines for the management of patients with ventricular arrhytmias and the prevention of sudden cardiac death: the task force for the management of patients with ventricular arrhytmias and the prevention of sudden cardiac death of the ESC. Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J 36(41): 2793-2867.
-
Veltmann C, Schimpf R, Echternach C, Eckardt L, Kuschyk J, et al. (2006) A prospective study on spontaneous fluctuations between diagnostic and non-diagnostic ECGs in Brugada syndrome: implications for correct phenotyping and risk stratification. Eur Heart J 27(21): 2544-2552.
-
Brugada R, Brugada J, Antzelevitch C, Kirsch GE, Potenza D, et al. (2000) Sodium channel blockers identify risk for sudden death in patients with ST- segment elevation and right bundle branch block but structurally normal hearts. Circulation 101(5): 510- 515.
-
Wolpert C, Echternach C, Veltmann C, Antzelevitch C, Thomas GP, et al. (2005) Intravenous drug challenge using flecainide and ajmaline in patients with Brugada syndrome. Heart Rhythm 2(3): 254-260.
-
Hong K, Brugada J, Oliva A, Berruezo-Sánchez A, Potenza D, et al. (2004) Value of electrocardiographic parameters and ajmaline test in the diagnosis of Brugada syndrome caused by SCN5A mutations. Circulation 110(19): 3023-3027.
-
Meregalli PG, Ruijter JM, Hofman N, Bezzina CR, Wilde AA, et al. (2006) Diagnostic value of flecainide testing in unmasking SCN5A-related Brugada syndrome. J Cardiovasc Electrophysiol 17(8): 857-864.
-
Rolf S, Bruns HJ, Wichter T, Kirchhof P, Ribbing M, et al. (2003) The ajmaline challenge in Brugada syndrome: Diagnostic impact, safety, and recommended protocol. Eur Heart J 24 (12): 1104- 1112.
-
Batchvarov VN, Govindan M, Camm AJ, Behr ER (2009) Significance of QRS prolongation during diagnostic ajmaline test in patients with suspected Brugada syndrome. Heart Rhythm 6(5): 625-631.
-
Conte G, Sieira J, Sarkozy A, Asmundis C, Giovanni D, et al. (2013) Life-threatening ventricular arrhythmias during ajmaline challenge in patients with Brugada syndrome: Incidence, clinical features, and prognosis. Heart Rhythm 10(12): 1869-1874.
-
Dobbels B, De Cleen D, Ector J (2016) Ventricular arrhythmia during ajmaline challenge for the Brugada síndrome. Europace 18(10): 1501-1506.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study