Tetralogy of Fallot
This is a mini review article of tetralogy of Fallot. This review article will discuss historical, anatomical, pathophysiologic, clinical and surgical management of tetralogy of Fallot. Author also discussed his experience with postoperative follow up in 45 patients with tetralogy of Fallot. Incidence of congenital heart defect is 8 per 1000 life birth. Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart defect (CHD) constitutes 5-10% of all CHD. Prevalence of TOF ranges from 0.26-0.48 percent per 1000 live birth.
Historical Background
Neils Stansion from Copenhagen in 1671 described pathology of Tetralogy of Fallot (TOF) in a still born fetus. Not until 1773 Edwardo Sandifort described clinical symptoms of TOF. Over a century later Etienne-Louis Fallot in 1888 described comprehensive clinical features of TOF “Maladie bleu” and its correlation with autopsy finding in a French journal. Since his description the name Tetralogy of Fallot is established [1]. November 29th 1944 Blalock-Thomas-Taussig first performed Subclavian artery (SA) to pulmonary artery (PA) anastomosis on a 15 month old female with dramatic relieve of cyanosis, known as Blalock-Tausig (BT) shunt enhancing increased pulmonary blood flow relieving cyanosis. Currently this is modified by using Gore-Tex tube connecting the SA to PA augmenting PA blood flow.
C. Walton Lilleahi at the University of Minnesota in 1954 first performed total repair of TOF in an 11 yr. old boy. Since then surgical survival has improved significantly with current mortality less than 1%. The anatomic diagnosis consists of a large mal aligned ventricular septal defect (VSD), right ventricular outflow tract obstruction (RVOTO), Overriding of the aorta and right ventricular hypertrophy. Clinical manifestation and hemodynamic changes depend on the severity of right ventricular outflow obstruction seen at various levels e.g. sub-valvar, valvar and supra-valvar and usually at multiple levels. TOF has fifteen percent incidence of pulmonary atresia [2]. Associated cardiac lesions Coronary artery anomalies in 10% of the patients, left anterior descending arising from the right coronary artery coursing along the RVOT area interferes with surgical repair, bicuspid Pulmonic valve, right sided aortic arch (25-30%), absent left pulmonary artery, Atrial septal defect, atrio-ventricular canal, partial or total anomalous pulmonary venous drainage. Aorto-pulmonary collaterals are more commonly seen in TOF with pulmonary atresia. TOF with absent pulmonary valve is rarely seen. Left superior vena cava is seen in 11% of cases [3, 4].
Embryology
A unique population of pluripotent cells breaks off from the crest of the neural fields and migrates into somatic mesenchyme and further differentiates into multiple cell types. Neural crests that arise from the cardiac crest migrated through developing pharyngeal arches and populate the mesenchyme of the aortic arch, conotruncus and conotruncal septum. Embryos deficient in cardiac neural cells have outflow tract and arch anomalies. These include Tetralogy of Fallot, Truncus arteriosus, double outlet right ventricle and conotruncal ventricular septal defect. Anterior deviation of the conal septum explains subsequent development of large VSD, sub-Pulmonic stenosis, overriding of the aorta and RVH because of equalization of RV and LV pressures. Therefore, the embryologic term “Monology of Fallot” is introduced.
Factors causing increased risk of TOF
Environmental factors e.g. maternal diabetes mellitus has 3 times higher risk. Retinoic acid used for acne, skin wrinkled cream in first trimester of pregnancy, uncontrolled maternal phynylketonuria, trimethadone used for seizure disorder during pregnancy. Genetic factors associated with TOF – DiGeorge’s syndrome, Trisomy 21, 18 and 13 (11.3% incidence), Alagille’s syndrome (10-15% incidence). However, 68% of TOF are non-syndromic [5, 3].
Recurrence Risk
2.5% if one sibling is affected, 8% if 2 or more are siblings are affected, 2.6% if maternal TOF and 1.4% if paternal TOF. Incidence of off-spring of both affected parents of TOF is still unknown.
Clinical Presentation
One third of NB with TOF are clinically recognized to be cyanotic at birth, all will have heart murmur from right ventricular outflow obstruction (RVOTO). Large VSD equalizes both ventricular pressures hence murmur of TOF is not from VSD. Cyanosis is recognized clinically as the child grows with increased RVOTO. Cyanotic spell usually occurs beyond 4 wks. Of age when an infant develops physiologic anemia. More frequently seen in the early morning hours while crying, feeding, defecation and during warm water bath. It does not happen in sleep.
During the spell the infant turns bluer because of increased right to left shunt from decreased systemic vascular resistance followed by hyperventilation to compensate for metabolic acidosis and then becomes limp, listless, and may develop seizure and even cerebro vascular accident (CVA). Heart murmur disappears during the spell because of diminished blood flow to the pulmonary artery. Very rarely congestive heart failure is seen at around 6 weeks of age only when the RVOT obstruction is mild therefore, left to right shunt through VSD. This is also known as “acyanotic TOF”. Usually infants and children are not failure to thrive unless associated with genetic disorder. Older children present with easy fatigue and squatting during physical activities. Cyanotic spell is less common at this age because they learn their limitation of physical activities and squatting prevents cyanotic spell. Clubbing of the finger and toe nail beds develops at around 18 months of age. Ejection systolic murmur is audible from pulmonic stenosis with single second heart sound. The loudness of the murmur is inversely proportional to the degree of cyanosis.
Laboratory Data
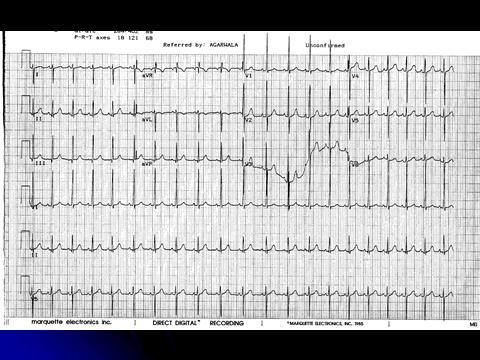
Chest x-ray (figure 1) typical shape of the heart is “Boot-shaped” with empty left hilum because of small main pulmonary artery and decreased bilateral pulmonary vascularities. Right sided aortic arch is seen in 25% of the time.

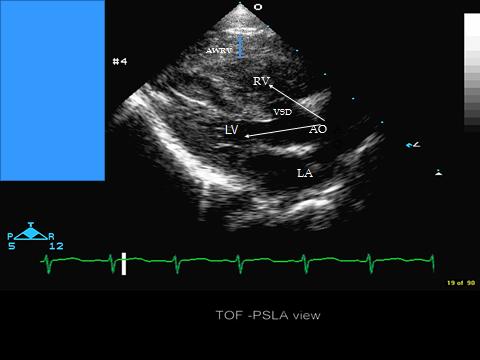
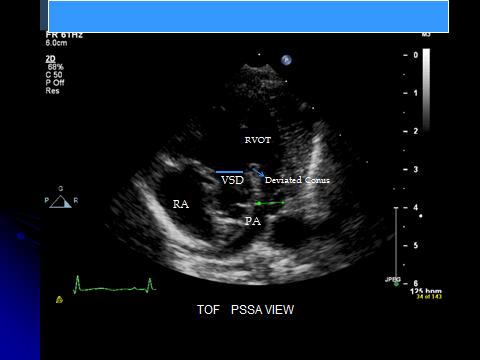
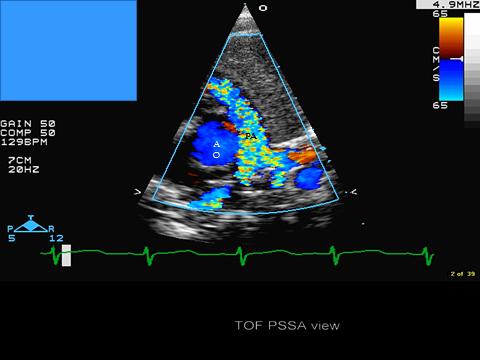
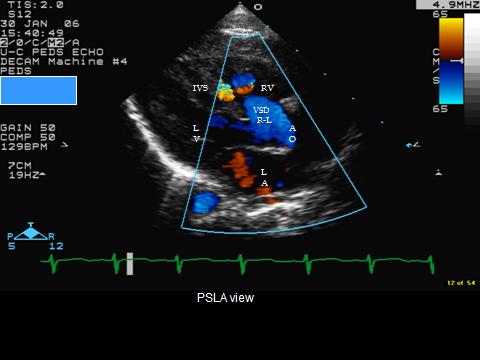
2D/Doppler Echocardiogram is Diagnostic
Rarely cardiac catheterization is needed prior to the surgical repair. ‘Suspected coronary artery anomalies’ can be difficult to detect by echocardiography. Thus, cardiac catheterization is indicated when adequate assessment of the haemodynamics cannot be obtained by non-invasive means and assessment of the pulmonary artery and aortic and coronary anomalies is insufficient by MRI or/and CT angiography. Coronary angiography is also indicated if surgical re intervention is necessary. Balloon dilatation of the pulmonic valve [6] is rarely indicated to delay neonatal surgery in some centers (Figure 3-6). Cardiac CT scan can define the cardiac anatomy and the need for catheterization is declining in most of the cardiac center.
Management
Cyanotic Spell Management Includes – Knee-chest position, intravenous volume, Na-bicarbonate, Morphine sulfate, phenylephrine continuous infusion to increase the systemic vascular resistance, Ketamine, Propranolol and if no response to the above management emergently may go the operating room for surgery. Giving oxygen helps only when pulmonary blood flow increases with the above measures. Medical management is to delay surgery for a few months and to prevent cyanotic spell. Parental education should include recognition of cyanotic spell. Many cardiologists prefer to put them on Beta-blocker (propranolol), Iron and keep them well hydrated. Dehydration may cause increased catecholamine release causing cyanotic spell [7]. Surgical management Currently Blalock-Tausig shunt is rarely done. Special indications are TOF with pulmonary atresia, unfavorable coronary artery anatomy in infant weighing less than 2.5 Kg. The indications may vary in different cardiac centers. Total repair of TOF is recommended at 3-6 months of age if clinical course permits [8]. It can be safely done at this age, avoids 2 surgeries (BT shunt and total repair) and BT shunt surgery complications. Also reduces length of hospital stay and cost. Early total repair restores pulmonary blood flow and therefore, enhances growth of the pulmonary arteries, less right ventricular hypertrophy and fibrosis. Resection of RVOT obstruction and VSD closure by atrial and trans pulmonary approach [9] is possible and also recommended in surgically important coronary artery anomalies.
Our experience with 45 patients with TOF since 1988
BT shunts in 10 patients within 2 wks of age. This is our earlier experience. Complete repair in 44 infants between 3-6 months of age One patient presented at 2 yrs of age when he had total repair. Trans-annular patch was placed in -10 RVOT patch and/or PA plasty in -34 RV to PA homograft in - 1 because of coronary artery anomalies LAD abnormal course over the RVOT. Disadvantages of RVOT trans-annular patch. Increased pulmonary regurgitation causing RV dilatation, Dysfunction, diminished exercise tolerance, cardiomegaly, prolonged QRS duration and ventricular arrhythmias.
Post-operative follow up of 45 patients: All had heart low grade murmur either from pulmonic stenosis or regurgitation One mortality who had uncontrolled cyanotic spell and went to operating room emergently. One developed complete heart block 2 wks after the surgery A 14 yr. old had sudden death while playing basketball 3 months after surgical pulmonary valve replacement. Five had isolated asymptomatic premature ventricular beats. No incidence of ventricular tachycardia Eight needed pulmonic valve placement. Pulmonic valve placement – 8 6 with trans-annular patch at primary repair 2 Two without trans-annular patch repair Surgical pulmonic valve placement in 6 Trans-catheter valve in 2. Stent placement in the pulmonary arteries in 6 for peripheral pulmonic stenosis
Indications for Pulmonic valve placement
Dilated RV: Cardiac MR showing RV end diastolic volume 140 ml/m2 body surface area, regurgitation fraction over 40%, decreased RV ejection fraction. Dilated RV with symptoms e.g. easy fatigue, palpitation, near syncope, poor exercise stress test. Ventricular or Atrial tachycardia with dilated RV Prolonged QRS duration over 180 ms
Conclusion
- Fetal echocardiogram diagnosis is relatively easy and it is very helpful for family counseling and delivery of the infant in a cardiac center for immediate attention.
- Total repair is recommended between 3-6 months of age.
- BT shunt is rarely indicated
- Avoid trans-annular patch if possible
- Percuteneous Pulmonic valve placement is gaining momentum in post operative patients with pulmonic regurgitation causing significant RV dilatation and dysfunction.
References
-
Mitchell SC, Korones SB, Berendes HW (1971) Congenital heart disease in 56,109 births. Incidence and natural history. Circulation 43(3): 323-332.
-
Anderson RH, Allwork SP, Ho Sy, Lenox CC, Zuberbuhler JR (1981) Surgical anatomy of tetralogy of Fallot. J Thorac Cardiovalsc Surg 81(6): 887-896.
-
Nora JJ, Nora AH (1976) Genetics and environmental factors in the etiology of congenital heart disease. South med J 69(7): 919-926.
-
Dabizzi RP, Teodori G, Barletta GA, Caprioli G, Baldrighi G, et al. (1990) Associated coronary and cardiac anomalies in tetralogy of Fallot. An Angiographic study. Eur Heart J 11(8): 692-704.
-
Dennis NR, Warren J (1981) Risk of the offspring of patients with some common congenital heart defects. J. med Genet 18(1): 8-16.
-
Sluysmans T, Neven B, Rubay J, Lintermans J, Ovaert C, et al. (1995) Early balloon dilatation of the pulmonary valve in infancy with tetralogy of Fallot. Risk and benefits. Circulation 91(5): 1506-1511.
-
Kothari SS (1992) Mechanism of cyanotic spell in tetralogy of Fallot the missing link? Int J Cardiol 37(1): 1-5.
-
Reddy VM, Liddicoat JR, McElhinney DB, Brook MM, Stanger P, et al. (1995) Routine primary repair of tetralogy of Fallot in neonates and infants less than three months of age. Ann Thorac Surg 60 (6): 592- 596.
-
Brizard CP, Mas C, Sohn YS, Cochrane AD, Karl TR (1998) Transatria-Transpulmonary tetralogy of Fallot repair is effective in the presence of anomalous coronary arteries. J Thorac Cardiovasc Surg 116(5): 770-779.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study