To Study Vitamin B12 Deficiency and Response to Treatment in Patients Presenting With Vasovagal Syncope
Objectives: Tilt table testing is widely used in the clinical evaluation of patients presenting with syncopal symptoms. As Vitamin B12 deficiency presents with various neurologic symptoms and signs including orthostatic hypotension and rarely syncope, it is hypothesized that Vitamin B12 deficiency may be related to the development of vasovagal syncope. Methods: 35 patients with recurrent syncope or first episode of syncope in whom vasovagal syncope was suspected were included. Results: A total of 153 patients with suspected vasovagal syncope were referred for Head-Up Tilt Test. Out of the 153 patients, 89 showed a ‘positive’ response to Tilt test and remaining 64 with ‘negative’ response were excluded. 50 of the 89 patients with a ‘positive’ response gave their written informed consent and were enrolled. Serum Vitamin B12 was measured at baseline in these 50 patients, of which 35 were found to be deficient and these were finally included. All deficient patients were supplemented with Vitamin B12 and Tilt test was repeated after 1 and 6 month periods after documenting Vitamin B12 sufficiency. At 1 month, 14 patients demonstrated a negative Tilt test with this number increasing to 17 on 6 month follow up. Conclusion: Supplementation of Vitamin B12 in deficient patients presenting with suspected Vasovagal syncope resulted in significant improvement in symptoms at 1 and 6 months of follow up. Vitamin B12 deficiency may be linked to Vasovagal syncope and all patients with suspected Vasovagal syncope should have their Vitamin B12 levels tested and supplementation given if found to be deficient.
Introduction
Syncope is defined as a transient loss of consciousness, with loss of posture (that is, falling). Commonly described as “fainting,” “passing out,” or “blackout,” syncope accounts for 3% of visits to emergency departments and 6% of all admissions to hospital [1, 2, 3].
It occurs relatively often in all age groups, ranging from 15% in children aged under 18 years to 23% in elderly patients aged over 70 years [4]. The prevalence and incidence of syncope increase with advancing age [5], with a 30% recurrence rate [3].
A reflex syncope is the most frequent cause of syncope in any setting and age group [6] representing 21% of all syncopes in the general population [7], 35%-48% of syncopes presenting to the emergency department [8] and 56% -78% of syncopes in a specialized syncope unit [8, 9]. The vasovagal syncope is by far the most common reflex syncope in young patients. Clinical studies reveal a peak incidence between 10 and 30 years of age [10, 11].
Reflex syncope is usually classified based on the efferent pathway most involved, i.e. sympathetic or parasympathetic. The term ‘vasodepressor type’ is commonly used if hypotension, due to a loss of upright vasoconstrictor tone, predominates. ‘Cardioinhibitory’ is used when bradycardia or asystole predominate, and ‘mixed’ is used if both mechanisms are present [12].
Tilt table testing has become a widely accepted tool in the clinical evaluation of patients presenting with syncopal symptoms. Currently, there is substantial agreement that tilt table testing is an effective technique for providing direct diagnostic evidence indicating susceptibility to vasovagal syncope [13].
The neurologic disorders associated with cobalamin (Cbl) deficiency are well described. Both the central nervous system and the peripheral nerves are affected. A wide variety of neurologic symptoms and signs are encountered including ataxia, loss of cutaneous sensation, muscle weakness, diminished or hyperactive reflexes, spasticity, urinary or fecal incontinence, orthostatic hypotension, loss of vision, dementia, psychoses, and disturbances of mood [14]. While orthostatic hypotension is well known in Vitamin B12 deficiency, syncope may also occur. Present study: The purpose to undertake this study was to evaluate Vitamin B12 levels in patients who present with vasovagal syncope and hence try to study the relationship between Vitamin B12 deficiency and vasovagal syncope and assess response to correction of Vitamin deficiency.
Aims and Objectives
- To assess serum Vitamin B12 levels in patients with suspected vasovagal syncope who are referred for Head-Up Tilt Test (HUTT).
- To study the effect of Vitamin B12 supplementation on response to Head-Up Tilt Test in patients with vasovagal syncope who were found to have Vitamin B12 deficiency.
Materials and Methods
Place of study: Care Hospital, Banjara hills, Hyderabad.
Study population
The study population consisted of all patients who presented to Cardiology department with recurrent syncope or first episode of syncope in whom vasovagal syncope was suspected and where other causes have been ruled out according to our inclusion and exclusion criteria. Study Period: 8 month period from June 2015 to January 2016. Study Design: Prospective, Observational Study.
Statistical method
The data was entered in Microsoft office excel 2007. 10% of the data was entered to correct for the data entry error. The data was analyzed using Epi-info software. The continuous variables were summarized as mean and standard deviation while categorical variables as percentage and proportion. Kolmogorov-Smirnov test was applied to test for normalcy of data, which showed that the data was normally distributed. Hence, parametric tests were applied. To show the difference between two independent categorical data chi-square test was applied. To show the difference in two dependent continuous data paired‘t’ test was applied. While for two dependent categorical data Mc-nemars Test was applied. We considered the test to be significant when the null hypothesis was disproved with a p-value less than 0.05. Sample Size: 35 patients
Inclusion Criteria
All patients with recurrent syncope or first episode of syncope in whom vasovagal syncope was clinically suspected and with a ‘positive’ Tilt test where other causes (eg: anaemia, postural hypotension) have been ruled out and with structurally normal heart (as evidenced by normal ECG and ECHO).
Exclusion Criteria
- Syncope with severe left ventricular outflow obstruction (for example, aortic stenosis)
- Syncope in presence of severe mitral stenosis
- Syncope in setting of known critical proximal coronary artery disease
- Syncope in setting of known critical cerebrovascular disease
- Syncope in patients with severe structural heart disease
- Patients with left ventricular dysfunction of any degree
- Syncope in the presence of arrhythmias
- Patients with diabetes mellitus
- Patients with bleeding or myocardial infarction as the cause of first episode of syncope
- Patients with seizure disorder
- Patients with postural hypotension
Methodology
All patients with recurrent syncope or first episode of syncope who presented to the Cardiology Outpatient department were evaluated with a detailed history and clinical examination. Patients in whom vasovagal syncope was suspected underwent relevant investigations to rule out other causes of syncope (eg. anaemia, postural hypotension) and ECG and ECHO were done to exclude structural heart disease. These patients with suspected vasovagal syncope were referred for Head-Up Tilt Test. Tilt test protocol Tilt testing aims to reproduce what happens when a person has neurally mediated syncope.
Tilt testing was carried out in a quiet, dim lit and temperature-controlled (23°C) room with the patient fasting for 2 hours before the test. The test was supervised by a technician and a doctor.
The following monitoring was carried out during a tilt test:
- Intermittent blood pressure every 5 minutes
- Continuous 3-lead ECG and heart rate monitoring The blood pressure and heart rate during the test was documented every 5 minutes. A crash trolley and resuscitation equipment was kept ready in the same room as the tilt test.
In the Tilt test protocol:
- Patients were asked whether they needed to empty their bladder
- Any support stockings was removed before the test
- The test was explained and consent taken
- Patients lay supine for 15 minutes and the monitoring equipment was attached
- Patients were tilted at 60-70° upright for 20 minutes
- If the test end points were not reached, Nitroglycerin was administered sublingually (0.4 mg) for an additional 15-min tilt duration.
- Oncoming syncope was aborted by means of tilt-back or counter-maneuvers, such as leg crossing, before a loss of consciousness set in Tilt test end points The tilt test was stopped and the patient laid flat immediately when:
- Systolic blood pressure fell below 80 mmHg - or was falling rapidly
- Heart rate fell below 50/min - or was falling rapidly
- Heart rate raised above 170/min
- Acute arrhythmia developed
- Patient complained of distress or discomfort
- The end of the protocol was reached Responses to Tilt testing:
The tilt test was considered ‘positive’ when the patient’s syncopal or pre-syncopal symptoms were reproduced and accompanied by hypotension, bradycardia (relative or otherwise) or both. Heart rate and blood pressure changes in isolation were not considered as a ‘positive’ test. ‘Positive’ response to tilt test in our study was classified as follows:
- Vasodepressor - The blood pressure falls but the heart rate does not fall by more than 10% from its peak.
- Cardio-inhibitory type A or ‘cardio-inhibition without asystole’ - The heart rate falls to less than 40/min for more than 10 seconds but asystole of more than 3 seconds does not occur.
- Cardio-inhibitory type B or ‘cardio-inhibition with asystole’ - There is asystole of more than 3 seconds.
- Mixed - A mixture of a vasodepressor response and cardio-inhibitory type A response.
All patients with a ‘positive’ response to Tilt test were included in our study. Due informed consent was taken. Serum Vitamin B12 level was tested using Chemiluminescence receptor assay by Cobas e 411 analyzer (Roche diagnostics; Normal reference range: 189
– 914 pg/ml) and those patients found to have Vitamin B12 deficiency were finally included in the study. Vitamin B12 deficiency was supplemented by Inj. Vitamin B12 (Cyanocobalamin 100 mcg/ 1ml) im once a day for 5 days followed by Inj. Vitamin B12 im once a week for 4 weeks and Vitamin B12 levels were repeated at the end of 4 weeks to demonstrate Vitamin B12 sufficiency. Head-Up Tilt Test was repeated at the end of 4 weeks to document any symptomatic benefit of therapy. Study patients were given oral Vitamin B12 supplementation and were followed up for a duration of 6 months. Tilt test was repeated after 6 months of supplementation to assess any improvement in symptoms.
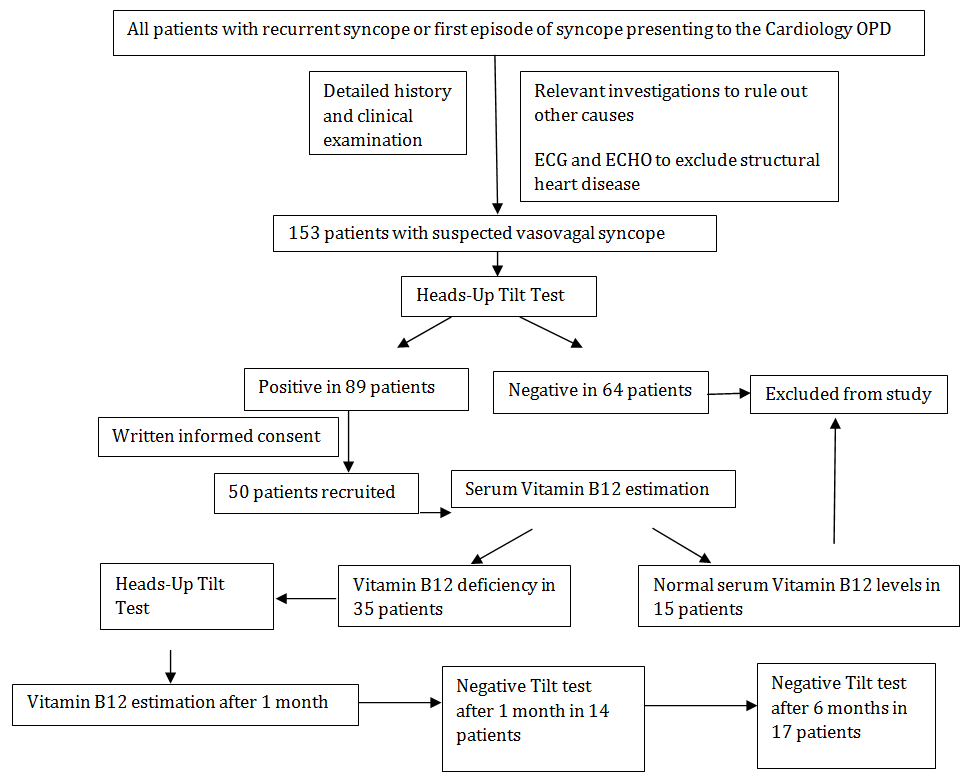
syncope who presented to the Cardiology outpatient department were evaluated with detailed history and clinical examination. Relevant investigations including ECG and ECHO were done to rule out other causes of syncope and to exclude structural heart disease. A total of 153 patients with suspected vasovagal syncope were referred for Head-Up Tilt Test. Out of the 153 patients who underwent Tilt test, 89 patients showed a ‘positive’ response to Tilt test and Tilt test was negative in 64 patients and these patients were excluded from the study. 50 of the 89 patients with a ‘positive’ response to Tilt test gave their written informed consent and were recruited for the study. Serum Vitamin B12 was measured at baseline in these 50 patients, out of which 35 were found to be deficient and these patients were finally included in the study. All deficient patients were supplemented with Vitamin B12 and Tilt test was repeated after 1 and 6 month periods after documenting Vitamin B12 sufficiency. At 1 month, 14 patients demonstrated a negative Tilt test with this number increasing further to 17 patients on 6 month follow up.
Observations and Results
We conducted the study at Care Hospital, Banjara Hills, Hyderabad. Required approval of Hospital Ethics committee and Scientific committee was taken before study. In the study period (June 2015 to January 2016), all patients with recurrent syncope or first episode of Flow Chart of the Study
There were a total of 35 study subjects, out of which 17 (48.5%) were male while 18 (51.5%) were females.
Maximum number, 13 (37.1%) of cases were in the 36 -50 years age group, followed by ≤ 20 years in 31.4% and 21 - 35 years in 28.6%. The mean age of the study participants was 29.8 years, mean age among male was 34.3 years while in female it was 25.6 years.
There were ≤ 5 episodes of vasovagal syncope in 22 (62.9%) of the subjects, in male it was 11 (64.7%) while in female 11 (61.1%). This difference in male to female distribution was found to be non - significant (p=0.89).
Maximum, 19 (54.3%) of the cases had once a week frequency of vasovagal syncope, followed by once a month in 13 (37.1%) cases. The difference in the frequency of episode among male and female was found to be non-significant (p=0.34).
Maximum, 21 (60%) of the subjects suffered vasovagal syncope both on sitting and standing. The difference in the position during which vasovagal syncope occurred among male and female was found to be non-significant (p=0.08).
All the study subjects suffered vasovagal syncope during rest. The most common predisposing condition for vasovagal syncope was found to be in crowded or warm places and with prolonged standing in 29 (82.9%). The most common precipitating event for vasovagal syncope was sleeplessness in 23 (65.7%), followed by intense pain and sight of blood which was 22 (62.9%) and 15 (42.9%) respectively. This difference among male and female was found to be non-significant (p=0.23).
The most common symptom at onset of vasovagal syncope was Nausea, vomiting and abdominal discomfort in 33 (94.3%), followed by feeling cold and blurring of vision which was seen in 29 (82.9%) each. This difference among male and female was found to be non-significant (p=0.71). Most common time of the day was afternoon for the vasovagal syncope in 20 (57.1%). The most common eyewitness account of the syncopal episode was slumping in all the subjects followed by pallor in 32 (91.4%). Most common symptom at end of vasovagal syncope was feeling cold and sweating in 30 (85.7%).
Most of the study subjects were vegetarian and this difference among males and females was found to be non- significant (p=0.63). This data also suggests that Vitamin B12 deficiency may be found in Non vegetarians.
All the subjects had normal systemic examination, ECG and ECHO findings and none had any co-morbidities, postural hypotension and anemia.
Serum Vitamin B12 levels in our study were tested using Chemiluminescence receptor assay by Cobas e 411 analyzer (Roche diagnostics; Normal reference range: 189-914 pg/ml) Mean serum Vitamin B12 level increased dramatically from 120.7 to 388.1 after supplementation and this mean difference was found to be statistically significant (p=0.001).
The most common ‘positive’ response to Tilt test elicited in our study was a Mixed response at baseline with almost similar frequencies of Cardioinhibitory type A, Vasodepressor and Mixed responses seen subsequently at 1 and 6 months.
The tilt table test improved significantly from none tilt negative at baseline vs 40% at end of 1 month post Vitamin B12 supplementation and this difference was found to be statistically significant (p=0.0001). This suggested that Vitamin B12 supplementation significantly improved the vasovagal syncope symptoms at end of 1 month.
The tilt table test improved significantly form none tilt negative at baseline vs 48.5% at end of 6 month post Vitamin B12 supplementation and this difference was found to be statistically significant (p=0.0001). This suggested that Vitamin B12 supplementation significantly improved vasovagal syncope symptoms even at the end of 6 months.
Discussion
A total of 35 patients were evaluated in our study, out of which 17 (48.5%) were male while 18 (51.5%) were females. Maximum number, 13 (37.1%) of cases were in the 36 -50 years age group, followed by 5 - 20 years in 31.4% and 21 - 35 years in 28.6%.The mean age of the study participants was 29.8 years, mean age among male was 34.3 years while in female it was 25.6 years.
In the study done by Wouter Wieling, et al. [15], incidence peak occurred around the age of 15 years, with females having more than twice the incidence of males. Syncope was an infrequent occurrence in adults. The incidence of syncope progressively increased over the age of about 40 years to become high in the older age groups. In a retrospective study of 1,180 patients referred for evaluation of syncope in a specialist unit, vasovagal syncope was diagnosed in 49% and 31% of subjects younger and older than 65 years, respectively [16]. A recent study into systematic evaluation of syncope of patients admitted to the emergency room diagnosed Vasovagal syncope in 190 (41%) of 465 patients, and the age distribution demonstrated 2 peaks at the ages of 20 to 29 years and older than 70 years [17].
In our study, there were ≤ 5 episodes of vasovagal syncope in 22 (62.9%) of the subjects, in male it was 11 (64.7%) while in female 11(61.1%) and this difference in male to female distribution was found to be non- significant (p=0.89). Maximum, 19 (54.3%) of the cases had once a week frequency of vasovagal syncope, followed by once a month in 13 (37.1%) cases. The difference in the frequency of episode among male and female was found to be non-significant (p=0.34).
These findings are consistent with the study done by Soteriades ES, et al. [18] which included 7814 study participants and which evaluated the incidence, specific causes, and prognosis of syncope among women and men participating in the Framingham Heart Study from 1971 to 1998. In that study, most individuals who were susceptible to reflex syncope had sporadic episodes; however, in a small percentage of the population vasovagal syncope presented as a chronic and recurrent disorder with a significant impact on quality of life. These patients suffered from recurrent syncopal or presyncopal attacks once a year to weekly or even daily.
In our study, maximum, 21(60%) of the subjects suffered vasovagal syncope both on sitting and standing. The difference in the position during which vasovagal syncope occurred among male and female was found to be non-significant (p=0.08). All the study subjects suffered vasovagal syncope during rest.
The most common predisposing condition for vasovagal syncope was found to be both crowded or warm places and prolonged standing in 29 (82.9%). The most common precipitating event for vasovagal syncope was sleeplessness in 23 (65.7%), followed by intense pain and sight of blood which was 22 (62.9%) and 15 (42.9%) respectively. This difference among male and female was found to be non-significant (p=0.23).
These are consistent with the findings of Gaggioli G, et al. [19] who described vasovagal syncope being precipitated by prolonged standing or sitting, hot environments, dehydration, systemic illness, emotional stress, fear, pain, venipuncture, sight of blood, and alcohol. Ruiter, et al. [20] identified that the types of environments in which vasovagal syncopes are more common are often hot, crowded and emotionally upsetting.
The most common symptom at onset of vasovagal syncope was nausea, vomiting and abdominal discomfort in 33 (94.3%), followed by feeling cold and blurring of vision which was seen in 29 (82.9%) each. This difference among male and female was found to be non-significant (p=0.71). Most common time of the day was afternoon for the vasovagal syncope in 20 (57.1%).
The most common eyewitness account was slumping in all the subjects followed by pallor in 32 (91.4%). These findings are similar to those described by Alboni P, et al. [21], who prospectively studied 341 patients presenting with syncope. They described three distinct phases of vasovagal syncope: a prodrome, loss of consciousness, and a postsyncopal phase. A precipitating event or situation (e.g., emotional stress, trauma, pain, sight of blood, prolonged standing) usually was identifiable. The prodrome, characterized by diaphoresis, epigastric discomfort, extreme fatigue, weakness, yawning, nausea, dizziness, and vertigo, resulted from increased parasympathetic tone and may last seconds to several minutes. Lying down or removing the stimulus may abort the syncopal episode. The postsyncopal phase may last hours or, rarely, days and may include protracted confusion, disorientation, nausea, dizziness, and a general sense of poor health.
Chen, et al. [1] described neurocardiogenic syncope being preceded by prodromata such as nausea, diaphoresis, lightheadedness, blurred vision, headaches, palpitations, paraesthesia, and pallor, which usually occurred in the upright position (with downward displacement of 300 - 800 ml of blood) and resolved almost immediately when the patient assumed the supine position. In addition, after recovery, patients with neurocardiogenic syncope may complain of a “washed out” and tired feeling.
In a study done by Parry SW, et al. [22] of vasovagal syncope in elderly, the prodrome of vasovagal syncope was more likely to be short or even nonexistent and the history of syncopal episodes in terms of length of time between symptom onset and presentation was also likely to be shorter. None of the above studies showed any evidence of severe traumatic injuries in patients with vasovagal syncope.
Although most patients display typical conditions and signs of a vasovagal syncope such as symptom onset during standing, light-headedness and full recovery after a few minutes, according to the study done by Grubb, et al. [23], up to 30% have an atypical presentation. In some cases syncope occurs without any prodromal symptoms.
Most of the study subjects were vegetarian and this difference was found to be non-significant (p=0.63). In a review study done by Pawlak R, et al. [24], higher rates of Vitamin B12 deficiency were reported among vegans compared with vegetarians and among individuals who had adhered to a vegetarian diet since birth compared with those who had adopted such a diet later in life. The main finding of this review was that vegetarians develop Vitamin B12 depletion or deficiency regardless of demographic characteristics, place of residency, age, or type of vegetarian diet. In the review of literature done by Pawlak R, et al. [25], the reviewed studies documented, with few exceptions, relatively high deficiency prevalence among vegetarians. Vegans who did not ingest vitamin In our study, after supplementation, mean Vitamin B12 serum level increased dramatically from 120.7 to 388.1 and this mean difference was found to be statistically significant (p=0.001) (Table 1).
B12 supplements were found to be at especially high risk.
All the study subjects had normal systemic examination, ECG and ECHO findings and none had any co-morbidities, postural hypotension and anemia. In a study done by Soteriades ES, et al. [18], which included 7814 study participants and which evaluated the incidence, specific causes, and prognosis of syncope among women and men participating in the Framingham Heart Study from 1971 to 1998, there was no increased risk of cardiovascular morbidity or mortality associated with vasovagal (including orthostatic and medication- related) syncope.
| Vitamin B12 Levels | Vitamin B12 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| P-value | |||||||||||
| (Normal reference range: 189 – 914 pg/ml) | Mean | SD | |||||||||
| Baseline | 120.7 | 28.1 | <0.001 | ||||||||
| Post supplementation | 388.1 | 130 |
Table 1: Effect of supplementation on mean serum Vitamin B12 level.
The tilt table test improved significantly from none tilt negative at baseline vs 40% at end of 1 month post Vitamin B12 supplementation and this difference was found to be statistically significant (p=0.0001). This suggested that Vitamin B12 supplementation significantly improved the vasovagal syncope symptoms at end of 1 month.
The tilt table test improved significantly form none tilt negative at baseline vs 48.5% at end of 6 month post Vitamin B12 supplementation and this difference was found to statistically significant (p=0.0001). This suggested that Vitamin B12 supplementation significantly improved vasovagal syncope symptoms even at the end of 6 months (Table 2 & Table 3).
| Tilt test | Cardioinhibitory type A | Cardioinhibitory type B | Vasodepressor | Mixed | Total | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 9 | 3 | 10 | 13 | 35 | ||||||||||||
| After 1 month | 7 | 2 | 7 | 5 | 21 | ||||||||||||
| After 6 months | 6 | 2 | 6 | 4 | 18 |
Table 2: Tilt test response.
| Variable | Positive Test | Negative Test | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Tilt table testing at baseline | 35 | 0 | 35 | |||||||
| Tilt table testing at 1 month | 21 | 14 | 35 (p=0.0001) | |||||||
| Tilt table testing at 6 months | 18 | 17 | 35 (p=0.0001) |
Table 3: Effect of Vitamin B12 supplementation on Tilt table test at 1 and 6 months.
In a study done by Moore A, et al. [26] where elderly patients over 70 years with Vitamin B12 deficiency (intervention group) were subjected to head up tilt and their response after replacement compared to those of matched patients with Idiopathic Orthostatic Hypotension and normal serum vitamin B12 concentrations (control group), initial Head-Up tilt produced a mean B.P decrease of 44/29 mmHg in the intervention group and 33/12 mmHg in the control group. Repeat Head-Up tilt 6 months after Vitamin B12 replacement produced a mean B.P decrease of 15/9 mmHg in the intervention group. The mean decrease in the control group was 30/12 mmHg. The difference in B.P decreases between groups was statistically significant for both systolic and diastolic B.P. Although only eight patients and eight controls were studied, the findings in this study suggested that replacing Vitamin B12 in older patients with Vitamin B12 deficiency is associated with improved orthostatic tolerance to head up tilt. A similar observation was also made in our study where Vasodepressor response to Head-Up Tilt test was seen in 10 of the 35 patients with Vitamin B12 deficiency at baseline, with this number reducing to 7 and 6 at 1 month and 6 months respectively after Vitamin B12 supplementation.
Beitzke, et al. [27] investigated hemodynamic and autonomic responses to 60 degrees passive Head-Up tilt in 21 patients with Vitamin B12 deficiency, 21 healthy age-matched control subjects and 9 age-matched patients with diabetes mellitus and established diabetic neuropathy. To systematically assess hemodynamic and autonomic nervous system function, they performed measurements of heart rate, beat-to-beat systolic and diastolic blood pressure, stroke index, cardiac index, total peripheral resistance index, total power, low (LF) and high (HF) frequency oscillatory component of heart rate variability, LF/HF ratio and spontaneous baroreflex sensitivity. As compared to controls, they found a significant fall of systolic blood pressure during 60 consecutive beats directly after head up tilt; furthermore, a significantly blunted fall of stroke index, cardiac index and a lack of increase of total peripheral resistance index for the duration of tilt in patients with diabetes mellitus and in patients with vitamin B12 deficiency. The results of this study suggested that Vitamin B12 deficiency causes autonomic dysfunction and defective sympathetic activation may be the cause for orthostatic hypotension, which is occasionally seen in patients with Vitamin B12 deficiency. They concluded that patients with orthostatic hypotension should be screened for cobalamin deficiency.
Thus, orthostatic hypotension is well reported in cobalamin deficiency as a manifestation of autonomic neuropathy, but concomitant bradycardia, which defines vagal response, is not well recognized. In our study the most common ‘positive’ response to Tilt test elicited was a Mixed response at baseline with almost similar frequencies of Cardioinhibitory type A, Vasodepressor and Mixed responses seen subsequently at 1 and 6 months. We also documented symptomatic benefit on Head-Up Tilt test at 1 and 6 months after Vitamin B12 supplementation suggesting that Vitamin B12 deficiency may be associated with vasovagal syncope and Vitamin B12 supplementation leads to improvement in symptoms.
In the year 2011, Sharada K, et al. [28] reported two patients from our institute with drug-refractory vasovagal syncope who had minimal clinical signs of cobalamin deficiency, in whom appropriate supplementation lead to prompt subjective and objective improvement. The positive results obtained then have paved the way for our current study evaluating the correlation between Vitamin B12 deficiency and vasovagal syncope and symptomatic response to treatment.
Leila Ganjehei, et al. [29] described a case of orthostatic hypotension in an elderly woman whose condition improved with vitamin B12 replacement therapy.
Recommendations
- Based upon our study results we recommend that patients presenting with suspected Vasovagal syncope should have their serum Vitamin B12 levels evaluated and if found to be deficient should be supplemented accordingly.
- Patients with Vitamin B12 deficiency at baseline tend to improve symptomatically over a period of 6 months after supplementation.
Limitations of the Study
- The measurement of Vitamin B12 deficiency by Chemiluminescence receptor assay is limited in sensitivity (90 – 95%) and specificity (<80%), missing many patients within the laboratory “gray zone” of deficiency. The sensitivity of detection of subclinical cobalamin deficiency ranges between 40 to 80% only (177). Measurements of serum methylmalonic acid (MMA) and homocysteine (tHcy) levels, which are surrogate biomarkers of Vitamin B12 deficiency, were not done in this study.
- Because a positive initial tilt test response may not be reproducible in ≈15% to 35% of patients, tilt testing may be less effective for predicting treatment efficacy than it is as a diagnostic tool.
• The follow-up period of patients after Vitamin B12
supplementation was only six months because of time constraints. However patients could be followed up for longer periods to assess persistence of symptomatic benefit.
- Patients with suspected vasovagal syncope and a ‘negative’ response to Tilt test were not included in the study.
- Patients with suspected vasovagal syncope with a ‘positive’ response to Tilt test and normal serum Vitamin B12 levels were not followed up clinically for symptom recurrence. Conflicts of Interest: None. We confirm that the manuscript has been read and approved by all the authors, that the requirements for authorship as stated earlier in this document have been met, and that each author believes that the manuscript represents honest work.
References
-
Chen-scarabelli C, Scarabelli TM (2004) Neurocardiogenic syncope. BMJ 329(7461): 336-341.
-
Kapoor WN (2000) Syncope. N Engl J Med 343(25): 1856-1862.
-
White CM, Tsikouris JP (2000) A review of pathophysiology and therapy of patients with vasovagal syncope. Pharmacotherapy. 20(2): 158- 165.
-
Brignole M, Alboni P, Benditt D, Bergfeldt L, Blanc JJ, et al. (2001) Guidelines on management (diagnosis and treatment) of syncope. Eur Heart J 22(15): 1256- 1306.
-
Kenny RA (2002) Neurally mediated syncope. Clin Geriatr Med 18(2): 191-210.
-
Moya A, Sutton R, Ammirati F, Blanc JJ, Brignole M, et al. (2009) Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J 30(21): 2631-2671.
-
Soteriades ES, Evans JC, Larson MG, Chen MH, Chen L, et al. (2002) Incidence and prognosis of syncope. N Engl J Med 347(12): 878-885.
-
Ammirati F, Colaceci R, Cesario A, Strano S, Della Scala A, et al. (2008) Management of syncope: clinical and economic impact of a Syncope Unit. Europace 10(4): 471-476.
-
Alboni P, Tomasi C, Menozzi C, Bottoni N, Paparella N, et al. (2001) Efficacy and safety of out-of-hospital self- administered single-dose oral drug treatment in the management of infrequent, well-tolerated paroxysmal supraventricular tachycardia. J Am Coll Cardiol 37(2): 548-553.
-
Ganzeboom KS, Colman N, Reitsma JB, Shen WK, Wieling W (2003) Prevalence and triggers of syncope in medical students. Am J Cardiol 91(8): 1006-1008.
-
Serletis A, Rose S, Sheldon AG, Sheldon RS (2006) Vasovagal syncope in medical students and their first- degree relatives. Eur Heart J 27(16): 1965-1970.
-
Tea SH, Mansourati J, L'heveder G, Mabin D, Blanc JJ (1996) New insights into the pathophysiology of carotid sinus syndrome. Circulation 93(7): 1411- 1416.
-
Wieling W, Krediet CT, Van dijk N, Linzer M, Tschakovsky ME (2007) Initial orthostatic hypotension: review of a forgotten condition. Clin Sci 112(3): 157-165.
-
Healton EB, Savage DG, Brust JC, Garrett TJ, Lindenbaum J (1991) Neurologic aspects of cobalamin deficiency. Medicine (Baltimore) 70(4): 229-245.
-
Wieling W, Ganzeboom KS, Saul JP (2004) Reflex syncope in children and adolescents. Heart 90(9): 1094-1100.
-
Colman N, Nahm K, Ganzeboom KS, Shen WK, Reitsma J, et al. (2004) Epidemiology of reflex syncope. Clin Auton Res 14(1): 9-17.
-
Alboni P, Brignole M, Degli uberti EC (2007) Is vasovagal syncope a disease?. Europace 9(2): 83-87.
-
Soteriades ES, Evans JC, Larson MG, Chen MH, Chen L, et al. (2002) Incidence and prognosis of syncope. N Engl J Med 347(12): 878-885.
-
Gaggioli G, Bottoni N, Mureddu R, Foglia-Manzillo G, Mascioli G, et al. (1997) Effects of chronic vasodilator therapy to enhance susceptibility to vasovagal syncope during upright tilt testing. Am J Cardiol 80(8): 1092-1094.
-
Ruiter JH, Barrett M (2008) Permanent cardiac pacing for neurocardiogenic syncope. Neth Heart J 16 (1): S15-19.
-
Alboni P, Brignole M, Menozzi C, Raviele A, Del Rosso A, et al. (2001) Diagnostic value of history in patients with syncope with or without heart disease. J Am Coll Cardiol 37(7): 1921-1928.
-
Parry SW, Kenny RA (2002) Vasovagal syncope masquerading as unexplained falls in an elderly patient. Can J Cardiol 18(7): 757-758.
-
Grubb BP (2005) Clinical practice. Neurocardiogenic syncope. N Engl J Med 352(10): 1004-1010.
-
Pawlak R, Parrott SJ, Raj S, Cullum-dugan D, Lucus D (2013) How prevalent is vitamin B(12) deficiency among vegetarians?. Nutr Rev 71(2): 110-117.
-
Pawlak R, Lester SE, Babatunde T (2014) The prevalence of cobalamin deficiency among vegetarians assessed by serum vitamin B12: a review of literature. Eur J Clin Nutr 68(5): 541-548.
-
Moore A, Ryan J, Watts M, Pillay I, Clinch D, et al. (2004) Orthostatic tolerance in older patients with vitamin B12 deficiency before and after vitamin B12 replacement. Clin Auton Res 14(2): 67-71.
-
Beitzke M, Pfister P, Fortin J, Skrabal F (2002) Autonomic dysfunction and hemodynamics in vitamin B12 deficiency. Auton Neurosci 97(1): 45-54.
-
Sharada K, Reddy G, Narasimhan C (2011) Cobalamin deficiency presenting as refractory vaso vagal syncope. Int J Cardiol 156(1): e7-8.
-
Ganjehei L, Massumi A, Razavi M, Wilson JM (2012) Orthostatic hypotension as a manifestation of vitamin B12 deficiency. Tex Heart Inst J 39(5): 722-723.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study