Myocardial Injury: an Umbrella Diagnosis of Confusion
The first description of myocardial infarction (MI) in the history of medical literature was in the late 19th century by Hammer, et al. It was not until the late 20th century, the first unified definition of MI was proposed by the working group of the World Health Organization based on electrocardiogram. Later, the definition of MI has advanced towards using both clinical and biochemical approaches after the development of more validated cardiac troponin (cTn).
Abbreviations
MI: Myocardial Infarction; cTn: Cardiac Troponin; UDMI: Universal Definition of Myocardial Infarction; NIMI: Nonischemic Myocardial Injury; URL: Upper Reference Level
Short Communication
The first description of myocardial infarction (MI) in the history of medical literature was in the late 19th century by Hammer, et al. [1]. It was not until the late 20th century, the first unified definition of MI was proposed by the working group of the World Health Organization based on electrocardiogram [2]. Later, the definition of MI has advanced towards using both clinical and biochemical approaches after the development of more validated cardiac troponin (cTn) [3]. In 2007 a Universal Definition of Myocardial Infarction (UDMI) consensus document introduced 5-subtypes of MI recognizing etiologically distinctive causes and was further refined in 2012 [4, 5]. In addition to the 5-subtypes of MI, many more categories have been identified with elevated cTn but without cardiac ischemia. To include those additional diversified groups of cohorts, in 2018, UDMI additionally introduced the terms “myocardial injury” and “Nonischemic myocardial injury” (NIMI) [6].
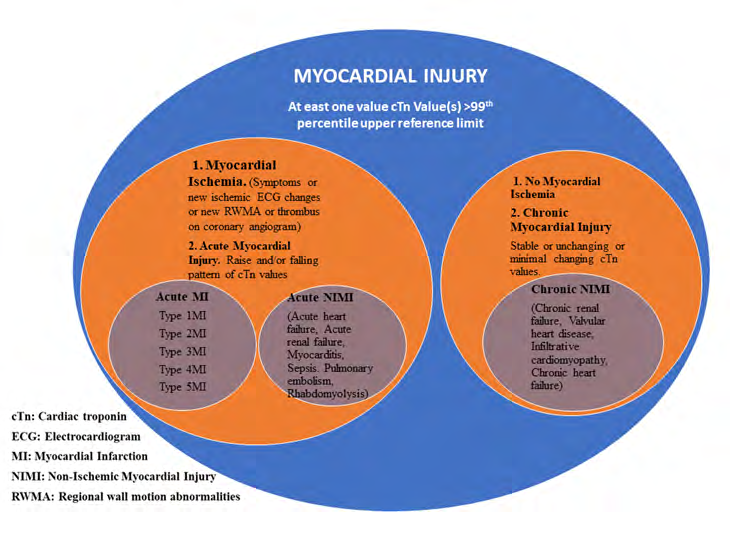
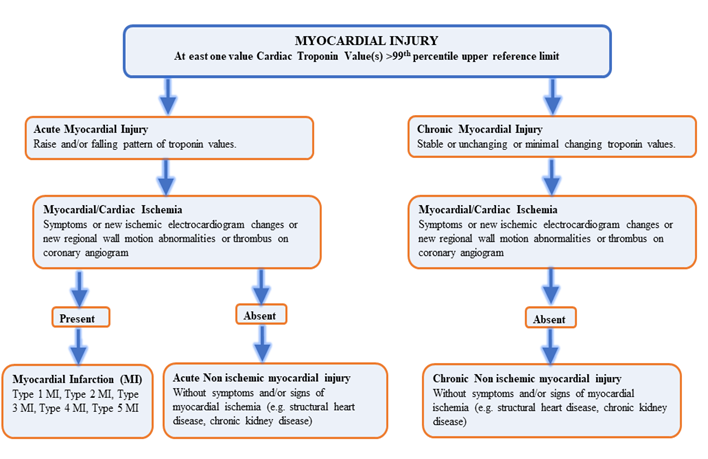
Myocardial injury is an umbrella term that broadly represents all the cases of elevated cTn with at least one value above the 99th percentile of the upper reference limit (URL) derived from a normal reference population. Myocardial injury is a large diagnostic category, and it does not specify any underlying pathophysiology or mechanism of the injury. The spectrum of myocardial injury is from no myocardial injury to myocardial injury itself to MI and NIMI. Myocardial injury may be acute; which manifests as a raising and/ or falling pattern, or chronic; in which cTn is persistently elevated or changes minimally with serial measurements. The diagnosis of MI is applied when there are any overt signs of clinical myocardial ischemia in patients with acute myocardial injury. Diagnosing myocardial ischemia is a crucial step in making distinctions among these categories. Diagnosis for myocardial ischemia is made if at least 1 of the following is observed: symptoms of myocardial ischemia, new ischemic electrocardiogram, new or presumably new regional wall motion abnormalities on echocardiogram, or acute coronary thrombus on coronary angiography [6]. MI is further subclassified based on underlying suspected pathophysiology as type 1-5. In those, Type 1 MI results from atherosclerotic plaque pathology, whereas type 2 MI from the conditions reflecting an imbalance between myocardial oxygen supply and demand, such as hypoxia, anemia, hypotension, bradyarrhythmia, tachyarrhythmias, and hypertension [6]. NIMI, on the other hand, is diagnosed when there is no evidence of overt myocardial ischemia [6, 7], and it may be acute NIMI; in the setting of dynamic raise and/or fall cTn pattern such as acute heart failure, pulmonary embolism, myocarditis, acute renal failure, sepsis, rhabdomyolysis, and extreme exertion, or chronic NIMI in the circumstances where cTn is persistently elevated without any signs or symptoms of cardiac ischemia, such as chronic heart failure, infiltrative cardiomyopathy, chronic renal failure, and valvular heart disease (Figures 1 & 2).
Over the last decade, cTn assays have become increasingly sensitive and improved its analytical performance. The higher tissue specificity, subsequently increased number of positive cTn patients with >99th percentile URL who had previously unrecognized myocardial injury [8, 9, 10]. However, the optimal approach to classify those patients into etiologically different categories remained uncertain until 4th UDMI introduced myocardial injury, acute NIMI, and chronic NIMI [6, 9]. Recent studies have reported that NIMI was not only found to be associated with an increased risk of all- cause mortality, cardiovascular mortality, MI, heart failure, and stroke [11, 12] but also its mortality was comparable to type 1 MI [13]. Data on optimal treatment in the NIMI is different from type 1 MI and limited due to heterogeneous nature with varying triggers [14, 15, 16, 17, 18, 19]. These groups urgently required protocols to attenuate the underlying injury. To improve the understanding of the mechanism of this distinct category, NIMI and myocardial injuries, and to compare the existing results across the relevant literature, it is vital to identify and classify NIMI patients accurately.
Disparities were noticed in categorizing these entities optimally across the literature both prior and after the 4th UDMI definition, which represents a significant opportunity for confusion [20]. Many studies have categorized patients experiencing NIMI as a myocardial injury category [11, 21, 22, 23, 24, 25, 26, 27, 28, 29]. In those, some of them were published before the fourth UDMI document release [11, 21, 22, 25, 26], and some even after 4th UDMI definition [24, 28]. This has brought vagueness among the researchers and clinicians. Studies have shown that a significant number of patients have been categorized inadvertently into different category; 24.5% of NIMI patients in Chapman, et al. [11] 69% of NIMI patients in Scotland study [26] 69% of NIMI patients in Sarkisian, et al. [21] 56% of NMI patients in Sandoval, et al. [22] were classified as myocardial injury. Similarly, 57.2% of non-acute coronary syndrome patients [25] were categorized as myocardial injury.
However, very few studies have defined myocardial injury correctly as any abnormally elevated cTn levels >99the percentile URL irrespective of underlying pathology, according to 4th UDMI definition [7, 13, 20, 30]. Even though optimal evaluation and treatment for these groups have yet to be defined [7, 13] nonetheless, it is imperative for the researchers and clinicians to diagnose and categorize these important entities appropriately.
Conflicts of Interest
The Author declares no potential conflict of interests.
References
-
Hammer A (1878) Ein Fall von thrombotischem Verschlusse einer der Kranzarterien des Herzens 28: 97- 102.
-
(1972) Working group on the establishment of ischemic heart disease registers. Report of the fifth working group, Copenhagen 8201(5).
-
Alpert J, Thygesen K, Antman E, Bassand JP (2000) Myocardial infarction redefined–a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol 36(3): 959-969.
-
Thygesen K, Alpert JS, White HD (2007) Universal definition of myocardial infarction. Circulation 116(22): 2173-2195.
-
Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, et al. (2012) Third universal definition of myocardial infarction. Circulation 126(16): 2020-2035.
-
Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, et al. (2018) Fourth Universal Definition of Myocardial Infarction. J Am Coll Cardiol 72(18).
-
McCarthy CP, Raber I, Chapman AR, Sandoval Y, Apple FS, et al. (2019) Myocardial Injury in the Era of High- Sensitivity Cardiac Troponin Assays: A Practical Approach for Clinicians. JAMA Cardiol.
-
Luepker RV, Duval S, Jacobs DR, Smith LG, Berger AK (2011) The effect of changing diagnostic algorithms on acute myocardial infarction rates. Ann Epidemiol 21(11): 824-829.
-
Reiter M, Twerenbold R, Reichlin T, Haaf P, Peter F, et al. (2011) Early diagnosis of acute myocardial infarction in the elderly using more sensitive cardiac troponin assays 32(11): 1379-1389.
-
Wu AH, Feng YJ, Contois JH, Pervaiz S (1996) Comparison of myoglobin, creatine kinase-MB, and cardiac troponin I for diagnosis of acute myocardial infarction. Ann Clin Lab Sci 26(4): 291-300.
-
Chapman AR, Shah ASV, Lee KK, Anand A, Francis O, et al. (2018) Long-Term Outcomes in Patients With Type 2 Myocardial Infarction and Myocardial Injury. Circulation 137(12): 1236-1245.
-
Eggers KM, Jernberg T, Lindahl (2019) Cardiac troponin elevation in patients without a specific diagnosis. J Am Coll Cardiol 73(1): 1-9.
-
DeFilippis AP, Chapman AR, Mills NL, de Lemos JA, Arbab ZA, et al. (2019) Assessment and Treatment of Patients with Type 2 Myocardial Infarction and Acute Non- Ischemic Myocardial Injury. Circulation 140(20): 1661- 1678.
-
Sandoval Y, Jaffe AS (2019) Type 2 Myocardial Infarction: JACC Review Topic of the Week. J Am Coll Cardiol 73(14): 1846-1860.
-
Mullis AH, Jogu HR, Ahmad MI, Feroz A, Mendapara V, et al. (2016) Abstract 16215: Statin Use in Asymptomatic Patients With Sepsis and Elevated Troponin is Associated With Lower Risk of Mortality 134(S1): A16215.
-
Jogu HR, Chevli PA, Bose A, Vasireddy A, Sompalli S, et al. (2017) Abstract 451: Beta Blocker Use in Asymptomatic Patients with Sepsis and Elevated Troponin is Associated with Lower Risk of Mortality 121(S1): A451.
-
Qureshi W, Jogu HR (2017) Use of Antiplatelets And Anticoagulants in Septic Patients with Troponin Elevation: Insights From Type Ii Mi Study 69(S11): 1025.
-
Chevli PA, Jogu HR, Islam T, Dutta A, Sunkara P, et al. (2019) Abstract 11511: Impact of Post-discharge Angiotensin-converting Enzyme Inhibitors/Angiotensin Receptor Blockers on Mortality in Patients With Asymptomatic Troponin Elevation in the Perioperative Period 140(S1): A11511.
-
Shenouda S, Dutta A, Jogu H, Brock J, Ahmad I, et al. (2019) Abstract 15000: Survival Effect of Beta-Blockers in Patients With Asymptomatic Perioperative Troponin Elevation 140(S1): A15000.
-
Goeddel LA, Hopkins AN, Fernando RJ, Nunez-Gil IJ, Ramakrishna H (2019) Analysis of the 4th Universal Definition of Myocardial Infarction-Key Concepts and Perioperative Implications. J Cardiothorac Vasc Anesth 33(12): 3486-3495.
-
Sarkisian L, Saaby L, Poulsen TS, Gerke O, Jangaard N, et al. (2016) Clinical Characteristics and Outcomes of Patients with Myocardial Infarction, Myocardial Injury, and Nonelevated Troponins. Am J Med 129(4): 446e5- 446e21.
-
Sandoval Y, Smith SW, Sexter A, Thordsen SE, Bruen CA, et al. (2017) Type 1 and 2 Myocardial Infarction and Myocardial Injury: Clinical Transition to High-Sensitivity Cardiac Troponin I. Am J Med 130(12): 1431-1439.
-
Jogu HR, Arora S, Vaduganathan M, Qamar A, Pandey A, et al. (2019) Wake Forest University long-term follow- up of type 2 myocardial infarction: The Wake-Up T2MI Registry. Clin Cardiol 42(6): 592-604.
-
Lee KK, Noaman A, Vaswani A, Gibbins M, Griffiths M, et al. (2019) Prevalence, determinants, and clinical associations of high-sensitivity cardiac Troponin in patients attending emergency departments 132(1): 110e8-110e21.
-
McFalls EO, Larsen G, Johnson GR, Apple FS, Goldman S, et al. (2011) Outcomes of hospitalized patients with non- acute coronary syndrome and elevated cardiac troponin level 124(7): 630-635.
-
Shah ASV, Anand A, Strachan FE, Ferry AV, Lee KK, et al. (2018) High-sensitivity troponin in the evaluation of patients with suspected acute coronary syndrome: a stepped-wedge, cluster-randomised controlled trial. Lancet 392(10151): 919-928.
-
Kadesjo E, Roos A, Siddiqui AJ, Desta L, Lundback M, et al. (2019) Acute Versus Chronic Myocardial Injury And Outcomes 73(9-S1): 105.
-
Januzzi JL, McCarthy CP (2019) Trivializing an Elevated Troponin. Adding Insult to Injury? J Am Coll Cardiol 73(1): 10-12.
-
Botto F, Alonso CP, Chan MT, Villar JC, Xavier D, et al. (2014) Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30- day outcomes 120(3): 564-578.
-
Ford I, Shah AS, Zhang R, McAllister DA, Strachan FE, et al. (2016) High-Sensitivity Cardiac Troponin, Statin Therapy, and Risk of Coronary Heart Disease. J Am Coll Cardiol 68(25): 2719-2728.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study