Pediatric Tricuspid Valve Infective Endocarditis- Insite into a Challenging Management
Pediatric tricuspid valve endocarditis is an uncommon entity which is now becoming prevalent owing to improved diagnostic methods and increase number of cardiac surgeries. Paediatric right sided infective endocarditis is mostly secondary to structural heart defects or indwelling venous catheters. We present a case of paeditric tricuspid valve endocarditis presenting with complete heart block, septic arthritis, pulmonary abscess with no structural heart defect diagnosed preoperatively. Intraoperatively a ventricular septal defect was diagnosed and managed. We present the difficult management of the case by medical and surgical intervention and management of secondary fungal infective endocarditis with repeated successful surgical intervention. We also emphasize on lack of established guidelines for management of right-sided infective endocarditis.
Introduction
Tricuspid valve infective endocarditis (TVIE) is very uncommon as compared to left-sided infective endocarditis. Right-sided infective endocarditis is about 5-10% of all cases of infective endocarditis [1]. In right-sided infective endocarditis cases tricuspid valve involvement estimated high up to 90%. The majority of tricuspid valve endocarditis cases are associated with IV drug abusers. Staphylococcus aureus is the most common organism found in TVIE. In comparison to adults IE is less common in children; however incidence is on the rise [2]. The treatment strategy for paediatric patients is also not well drafted. Here we present a pediatric case of patient with Tricuspid valve endocarditis with un-resolving vegetation despite antibiotic treatment warranting surgical intervention.
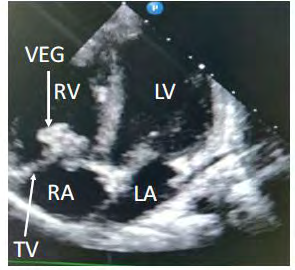
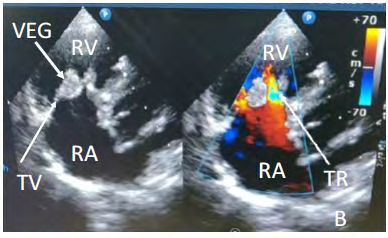
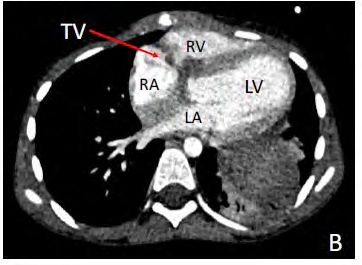
A 8 year old male child presented with history of fever for 20 days, arthritis of left knee and ankle for 15 days and 1 episode of syncope 5 days prior to admission. On echocardiography he was found to have vegetation on tricuspid valve 10×14 mm on anterior tricuspid leaflet and 10×6 mm on septal tricuspid leaflet with moderate tricuspid regurgitation, normal right ventricular function, mild LV dysfunction (EF= 45-50%) mild pulmonary regurgitation, no ASD, VSD, PDA, no pericardial effusion was found, rest valves were normal (Figures 1 & 2). Blood cultures revealed MRSA positive and a diagnosis was made of MRSA positive infective endocarditis. Patient had third degree AV block with junctional escape rhythm of 42 beats/min, right bundle branch block was also present. Patient was started on a combination of intravenous antibiotic vancomycin, ceftriaxone and gentamycin. Isoprenaline infusion was started in view of complete heart block. On serial echocardiography it was found that the vegetations were not resolving and clinically patient was having persistent pyrexia. Decision was taken for surgical intervention. Patient was taken up for tricuspid valve repair and epicardial pacemaker implantation.
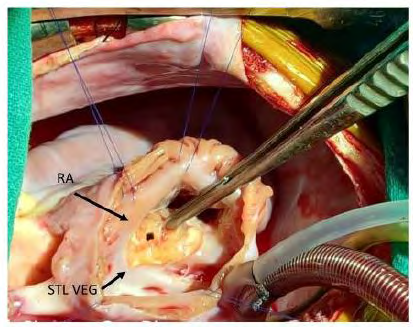
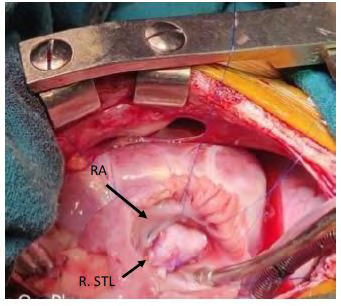
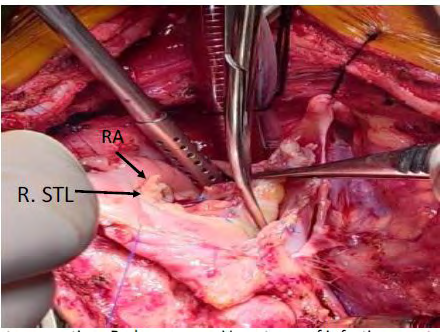
Patient underwent midline sternotomy, followed by splitting of thymus. Pericardium was harvested, patient was put on cardiopulmonary bypass and heart was arrested using delnido cardioplegia. Right atrium was opened and the tricuspid valve was examined. On table examination revealed that the septal leaflet of tricuspid valve was completely covered with vegetation and underneath the septal leaflet, (Figure 3) there was a presence of a perimembranous ventricular septal defect which was not earlier identified on echocardiography. After vegetectomy from the septal leaflet, ventricular septal defect was closed using an autologous untreated pericardial patch (Figure 4). Post VSD closure, the tricuspid valve check revealed severe tricuspid valve regurgitation. The septal leaflet reconstruction was done with autologous unfixed pericardium, the saline test now revealed mild central tricuspid regurgitation and a decision was taken to close the right atrium and patient was weaned off bypass and then epicardial pacemaker leads were placed and the pacemaker was connected. Patient was successfully weaned of cardiopulmonary bypass with minimal inotropic supports. Post operatively patient was continued on aforementioned antibiotics with addition of injection linezolid based on sensitivity pattern. 15 days latter patient developed severe left hip joint pain. Septic arthirits was ruled out and a diagnosis of reactive arthiritis was made which resolved with physiotherapy and nutritional rehabilitation. Patient recovered well and was discharged with adequate antibiotics for 3 months and was adviced for regular follow up. After 1 weak patient developed low grade fever, body ache and headache for which patient was given antipyretics and was screen with echocardiography which didn’t reveal any significant findings. The symptoms subsided for a week, then patient started having intermittent high grade fever which later evolved into continuous fever, patient was subjected to covid-19 screening with RT-PCR which was reported as negative. Patient was readmitted and thorough investigation was done. Patient had an episode of loss of consciousness with clenching of teeth. Patietn had no past history of seizure episode. Cardiac monitor data history revealed polymorphic VT. Blood cultures revealed Candida tropicalis and serum galactomannam was positive. Urine culture was positive for candida glabrata.
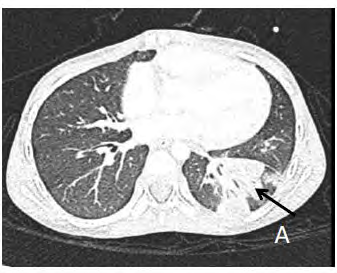
Echocardiography revealed no residual VSD, large vegetations on anterior tricuspid leaflet (2.4 cm×1.4 cm) and septal leaflet was thickened, moderate tricuspid regurgitation, rest valves normal with normal biventricular function. Antifungal liposomal amphotericin B was added along with caspofungin as per sensitivity pattern. Follow up echo after 1 week revealed increase in size of vegetations – ATL-24mm×12 mm, STL- 20mm×10mm, vegetations were freely mobile. Chest xray revealed lower lobe patch, which was further investigated with a high resolution computed tomography chest. HRCT revealed visualized lungs and mediastinum multiple centrally hypodense lesions with thin periphearally enhancing walls are seen in left lower lobe with largest one measuring 1.6x1.3cm likely to be abscesses (Figure 5,6), Patchy area of segmental collapse/ consolidation with volume loss seen in adjacent left lower lobe. Few subcentimetric nodular lesions are seen in bilateral lung parenchyma with at least two having pocket of air within. Few enlarged mediastinal lymph nodes are seen in pretracheal and precarinal region with largest one measuring 15mm.
Patient was not improving on medical management and a decision was taken for surgical intervention. Redo- sternotomy was done and patient put on cardiopulmonary bypass .Aorta was cross clamped and cardioplegia was given, right atrium was opened and tricuspid valve was inspected and it revealed large vegetations on prior reconstructed septal tricuspid leaflet and anterior tricuspid leaflet (Figure 7). Pericardial VSD patch was intact with no vegetations on it. On vegetectomy only posterior tricuspid was present and it was decided to put a bioprosthetic 25 # EPIC mitral valve in tricuspid position. Patient was weaned off cardiopulmonary bypass on high inotropic supports. Post operatively patient was kept on IV antibiotics and antifungals and patient recovered well over a period of time with antifailure drug treatment and other supportive measures.
Discussion
TVIE is an uncommon condition in pediatric patients with serious complications. Diagnosis of TVIE requires clinical finding, microbiological analysis, and imaging. The clinical features are often non-specific and may include fever, chills, fatigue or weight loss. Fever is the most common clinical manifestation present in about 95% to 100% of patients. The diagnosis of infective endocarditis is concluded on the basis of modified Duke Criteria. The presence of two major or one major and three minor, or five minor clinical criteria is diagnostic of IE. The complex nature of this disease demands accurate diagnosis and promotes treatment [3]. Pre-existing heart disease is the main predisposing factor for pediatric IE and cases of IE without underlying heart disease have been increasingly reported [4]. There is increasing number of surviving children following cardiac surgery which is considered as a risk factor for IE.
There are some differences in the characteristics of IE between children with normal heart and those with abnormal heart. Microorganisms causing endocarditis in children with normal heart may differ from those causing IE in children with abnormal heart [5]. Right-sided endocarditis can occur when there are intravenous catheters; therefore, microorganisms carried by the bloodstream enter the right side of the heart, potentially causing IE. It is known that the treatment of bacterial IE requires 4-6 weeks of antibiotics. The duration needed may be even longer in cases of fungal endocarditis. Surgical indications and timing of surgery in IE are subjects of debate [6]. It is important to consider early intervention in active IE to avoid progression to acute intractable heart failure, irreversible structural damage, persistent source for bacteremia and systemic infectious thromboembolic phenomena [6].
Numerous pulmonary infarcts and abcesses resulting from small septic emboli may be associated with right-sided bacterial endocarditis. Like in our case patient developed left lung lower lobe abcess secondary to tricuspid valve vegetation. Mansour, et al. reported regarding an 11-year-old child who had IE complicated with small septic pulmonary emboli originating from the tricuspid vegetation [7]. Although Shamszad, et al. mentioned that the lesions that are located in the left-sided heart were the most that needed surgical intervention, in our cases, the right-sided heart was the affected site and warranted a surgical intervention [8]. In our case we were met with the challenge for treating the patient twice with limited options as for valve substitutes as the initial repair failed in view of recurrent infective endocarditis and since the patient belonged to pediatric age group. Currently, in the absence of pediatric evidence- based data that favor prophylactic surgery for the prevention of primary thromboembolic events, decision of health care providers is difficult and individualized.
IE is a disease that needs a collaborative approach. European guidelines established criteria to transfer the patient to an ‘‘endocarditis team’’ [6]. Early consultations with infectious disease, cardiology, and cardiac surgery services are recommended for these patients. It is also important to define the patient populations that are at higher risk for IE or its complications and require an aggressive management like being subjected to surgical intervention.
Data Availability
All the data is available, if enquired about Statement of informed Consent- Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
References
-
Hussain ST, Witten J, Shrestha NK, Blackstone EH, Pettersson GB (2017) Tricuspid valve endocarditis. Ann Cardiothorac Surg 6(3): 255-261.
-
Baltimore RS, Gewitz M, Baddour LM, Beerman LB, Jackson MA, et al. (2015) American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young and the Council on Cardiovascular and Stroke Nursing. Infective Endocarditis in Childhood. Circulation 132: 1487-515.
-
Hansen JB, Jagt T, Gundtoft P, Sorensen HR (1973) Pharyngo-oesophageal diverticula. A clinical and cineradiographic follow-up study of 23 cases treated by diverticulectomy. Scand J Thorac Cardiovasc Surg 7(1): 81-86.
-
Dinubile MJ (1984) Heart block during bacterial endocarditis: a review of the literature and guidelines for surgical intervention. Am J Med Sci 287(3): 30-32.
-
Russell HM, Johnson SL, Wurlitzer KC, Backer CL (2013) Outcomes of surgical therapy for infective endocarditis in a pediatric population: a 21-year review. Ann Thorac Surg 96(1): 171-174.
-
Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, et al. (2015) 2015 ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European Society of Cardiology (ESC) endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 36(44): 3075-3128.
-
Mansour B, Habib A, Asli N, Geffen Y, Miron D, et al. (2016) A case of infective endocarditis and pulmonary septic emboli caused by Lactococcus lactis. Case Rep Pediatr 2016: 1024054.
-
Shamszad P, Khan MS, Rossano JW, Fraser CD (2013) Early surgical therapy of infective endocarditis in children: a 15-year experience. J Thorac Cardiovasc Surg 146(3): 506-511.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study