An Insight into Interventions after Previous Coarctation of Aorta Repair
After initial intervention for management of coarctation of aorta, recoarctation rates remain variable with different surgical approaches for repair of coarctation of aorta, ranging between 10-41 percent. Various techniques remain prevalent and preferable in different situations and patients of different ages. The most common reintervention is done for restenosis after endovascular balloon dilatation and open surgical repairs. Aneurysmal degeneration is another cause of reintervention, seen after surgical repair and endovascular repair. Endovascular procedures, balloon dilation, stent grafting, and open surgical repairs may be applicable for reintervention. There are specific challenges and risks related to reintervention using either endovascular procedures or open surgical repairs as strategies for restenosis and aneurysms after the previous coarctation of aorta repair.
Introduction
Coarctation of the Aorta is a common congenital abnormality accounting for up to 5-8% of all congenital heart defects [1, 2]. Without treatment, patients have a high mortality and risk of complications that include hypertension, aneurysms, and aortic dissections [3]. First surgical correction in 1945 by Crafoord C, et al. [4] paved the path for surgical correction to become a viable option with excellent early and long-term results [5]. Long-term survival after repair of Coarctation of the aorta is well established. However, due to the higher restenosis rate of the proposed excision and end-to-end anastomosis technique, many newer techniques involving either patch plasty using a Dacron patch or autologous subclavian artery turn down were introduced, all with their inherent advantages as well as drawbacks [6, 7]. Endovascular techniques evolved for the repair of coarctation in children and adults. Both the endovascular and open surgical techniques are associated with reinterventions.
The re-coarctation rates remain variable with different surgical approaches ranging between 10-41% [8, 9]. Various techniques are preferable in different situations and patients of different ages. Reinterventions are done for restenosis after endovascular balloon dilatation and open surgical repairs. Aneurysmal degeneration is another indication for reintervention, which is seen after surgical repair and endovascular repair. Endovascular procedures, balloon dilation, stent grafting, and open surgical repairs may be applicable for reintervention. There are specific challenges and risks related to reintervention using either endovascular procedures or open surgical repairs as strategies for restenosis and aneurysms after the previous coarctation of aorta repair [10, 11, 12]. Reintervention in cases of previous coarctation repair can be demanding technically and bear higher risk of mortality and morbidity.
Recoarctation after Previous Surgical Repair of Coarctation of Aorta
After repair of Coarctation of aorta, most reinterventions are done for restenosis or recurrence of Coarctation, usually at the site of previous coarctation repair. They have been reported more commonly in cases that are operated in infancy [2, 13, 14, 15]. This can be attributed to a high incidence of associated arch hypoplasia in cases presenting early in infancy. Re-coarctation after primary repair of aortic coarctation is indicated by persistence or recurrence of upper body hypertension and gradient of more than 20mm Hg between upper and lower limbs. Many methods have been used for confirmation of restenosis after the previous repair. Echocardiography can demonstrate persistent shelf at the previous repair site, arch dimensions, measurement of gradients across arch and repair site, Doppler flow dynamics, systolic flow velocity in DTA. CT angiography or MRI is also used as modalities to determine the anatomy of recurrent Coarctation. MRI can also provide gradients and was used as a gold standard investigation in one study of repaired coarctations in adults [16].
In adults, an exercise stress test with an abnormal hypertensive response indicated by Diastolic Blood Pressure higher than the 95 th percentile for that age and sex and 24-hour ambulatory BP monitoring has been used in some studies as indicators of recurrent Coarctation of aorta after the previous repair [16, 17, 18]. Operation in early infancy, Clamp related injury to proximal Descending aorta or arch, distal arch or isthmic hypoplasia, failure of growth of aortic arch after repair of Coarctation are reported as causes of recurrent Coarctation after previous surgical or endovascular interventions [19].
In their series Korn IL, et al. [15] reported a 21 percent incidence of reoperation for restenosis after previous Coarctation of aorta repair with excision and end to end anastomosis versus 9 and 3.6 percent respectively after Subclavian flap aortoplasty and Dacron patch aortoplasty. Many other reports point towards an even higher rate of restenosis after excision and end-to-end anastomosis, especially during infancy [8, 20, 21].
Dodge‐Khatami A, et al. [22] noted that the incidence of restenosis was highest with end-to-end anastomosis and subclavian flap aortoplasty, more so when there was arch hypoplasia associated. Extended resection and end-to-end anastomosis, first described by Amato JJ, et al. [23] in 1977 have shown excellent results regarding low mortality and fairly lower incidence of restenosis. One series noted higher restenosis rates with extended resection and anastomosis in preterm infants than in term infants [24]. Wright GE, et al. [25] observed that extended end-to-end anastomosis had a low (6percent) risk of recurrent Coarctation even in early infancy.
Subclavian flap aortoplasty also came up as a procedure to decrease the high recoarctation rate seen with excision and end to end anastomosis and the advantage of the flap’s growth potential. There are reports of a low (0-3%) restenosis rate with this procedure among older children [26]. However, when applied to patients in early infancy, the results are not as good, and high restenosis rates of up to 23% have been noted [27, 28]. One series of surgical repair of Coarctation of the aorta in 48 neonates (45 with subclavian flap aortoplasty and 3 PTFE patch plasty) reported an 18% recurrence rate [29].
Recoarctation after previous Endovascular Repair of Coarctation
Balloon angioplasty for aortic Coarctation has an attractive option in older children and adults and an acceptable alternative to surgery in this subgroup of patients. Application of balloon dilation in sick infants, even premature ones with low birth weight who present with Coarctation of the aorta, has acceptable early outcomes [2]. However, it is often associated with high recoarctation rates of up to 80% in various series. [30]. De Lenzo JS, et al. [31] found that balloon angioplasty had good outcomes in children and adults, especially those with discreet Coarctation. However, the results for long-segment Coarctation and arch involvement were not acceptable and showed high restenosis rates and even development of late aneurysms.
Another series has shown that balloon dilation, although having comparable early results and even lower mortality and hospital stay, has an unacceptably high recoarctation rate for coarctation repair than surgery, even in older children and adults. The balloon dilation subgroup had a higher aneurysm degeneration rate over a median follow-up of 3 years [32].
One series noted balloon dilation to be an acceptable alternative to surgery in older children and adults with results comparable to surgery in terms of restenosis but demonstrated a high (35 percent) aneurysm formation in the follow-up period. More than half of these aneurysms developed at an average follow-up of one year, and the rest developed as of late aneurysms [33]. Endovascular stent grafting has an advantage over simple balloon dilation. It provides some theoretical protection against restenosis and is for native coarctation repair and recoarctations in older children and adults. The recoarctation rates with stenting for native Coarctation have been found to be similar to open surgical repair. In some cases, acute aortic wall injuries were noted in one series, but they did not need any intervention. Aneurysmal degeneration occurred in 6 percent cases at a median follow-up of 2.5 years [34].
One multicenter report of stent grafting for native and recurrent coarctations, including over 500 cases and 15 years follow-up, noted good early outcomes of stenting for Coarctation of aorta. They noted excellent procedural success in up to 97% of cases, especially in discrete coarctations. Acute complications including dissections of aorta, tears, aneurysms, CVA, peripheral emboli, access vessel complications, and stent migration were noted in 14% of cases. They noted that patients more than 40 years were a high-risk group with up to 31 percent incidence of aorta-related complications [35]. Another multi-institutional observational study that compared the results of surgery, balloon dilation, and stenting for native Coarctation found that both the stent and surgery groups had good early outcomes in terms of hemodynamics and procedural success and were superior to balloon dilation. The stent group had the lowest acute complication rates. It was observed that the stent group had the highest number of unplanned reinterventions, most of which were for recurrent Coarctation [36]. A randomized controlled study to compare the results of surgery and balloon angioplasty in patients of 1 to 16 years age group found that the mortality, procedural success, immediate complications, and aneurysm formation were similar in both arms of the study. However, at follow up the balloon angioplasty group had statistically significant higher recoarctation rates at 50% and persistent hypertension at 49% versus 21% and 19% respectively in the surgery group [37].
Aneurysms after Previous Surgical and Endovascular Coarctation of Aorta Repair
Aneurysmal degeneration after surgical or endovascular repair of Coarctation of the aorta is a well-documented complication that often demands reintervention. In their series, Knyshov GV, et al. [38] found that over a period of up to 24 years after primary repair of aortic Coarctation, 5.4 percent of patients developed aneurysms at the site of the previous repair. They also noted that the longer the period after primary repair higher was the probability of developing an aneurysm. True as well as false aneurysms have been reported to develop at the site of coarctation repair. True aneurysms are usually observed in the aortic wall opposite to the prosthetic patch, and false aneurysms are generally associated with suture line dehiscence or infections [38, 39].
Many causes and risk factors for aneurysm formation after coarctation repair have been postulated and include- intimal damage due to excessive resection of coarctation ridge at primary repair, increased hemodynamic stress on the aortic wall opposite to the rigid synthetic patch, long- standing hypertension may be additive to this hemodynamic stress [40, 41, 42]. Some procedures, surgical and endovascular including, leave behind the abnormal tissue at the coarctation site can result in an aneurysm [43]. Some researchers have noted and pointed towards a congenital tendency and weakness in the aortic wall of patients with Coarctation of aorta and acquired issues such as atherosclerosis that predispose to the formation of an aneurysm in patients with repaired Coarctation of aorta [40, 44, 45]. Older age at primary operation of aortic Coarctation is also regarded as a risk factor of aneurysm formation, especially after patch aortoplasty [46].
Aneurysms after coarctation repair can often be asymptomatic suspected on routine imaging with chest X-ray and confirmed with cross-sectional imaging with CT or MRI. However, the aneurysms can also present with minor symptoms of chest or back discomfort and pain and occasionally fine streaks of blood in sputum or in an emergency with shock and unstable hemodynamic with hemothorax or massive hemoptysis due to ruptured aneurysm.
The incidence of the aneurysm after Coarctation of aorta repair has been highest between 6 to 16 years after primary repair [38]. It is reported most commonly with Synthetic patch aortoplasty with up to 9% incidence [38]. Different series have observed an incidence of 20-51% with patch aortoplasty [39, 47, 48]. Korn IL, et al. [15] observed no aneurysms after either excision and end to end anastomosis and Subclavian flap aortoplasty. They noted aneurysms in 16% of cases of synthetic patch aortoplasty and 14% cases of interposition graft repair for Coarctation of the aorta. Other series have reported aneurysmal degeneration after Subclavian flap aortoplasty and Interposition grafting in up to 17% of cases [39, 49]. In a long-term randomized study to compare the results of balloon angioplasty and surgery for Coarctation of aorta the researchers found that the balloon angioplasty arm had 35% aneurysms versus none in the surgical arm on long term follow up. They also noted that whereas more than 87% of surgical candidates were free from reintervention and aneurysm formation, only half of the balloon angioplasty group was free from such events [33].
Shaddy RE, et al. [50], in a randomized study of 36 patients, found that immediate procedural outcomes were similar in the surgical and angioplasty groups. There were no aneurysms in the surgery arm at follow-up, were 20% in the angioplasty arm developed aneurysms. Of these, they reported none required reintervention. Twenty-five percent cases in the angioplasty group and 6 percent cases in the surgery group developed restenosis. Fletcher SE, et al. [51] noted a 91% procedural success rate, 22% restenosis rate at follow-up of 86 months, and 1.9% rate of aneurysm formation after balloon angioplasty in a cohort of patients age three days to 29 years. In their series of seven cases that underwent endovascular stent grafting for Coarctation of the aorta Bulbul ZR, et al. [52] reported good procedural success in terms of increased diameter of the coarct segment and reduction in gradient. They noted that half the patients were normotensive and there were no recurrences of coarctations and no aneurysms at a median follow-up of 8 months.
In one series of 65 patients treated for primary Coarctation of the aorta by self-expandable nitinol stents, the author demonstrated the successful outcome of the procedure with reduced gradients in all patients. 4.6% of patients developed recoarctation at 16 to 18 months and were managed by endovascular balloon dilation. They reported no aneurysms at a mean follow-up of 45 months [53]. Pedra CA, et al. [54] compared a cohort of 21 adolescent and adult patients who underwent endovascular stenting with another cohort of 15 patients who had balloon angioplasty for native Coarctation of the aorta. They found that both the techniques were equally effective and safe in decreasing the gradients in discreet native Coarctation of aorta. In their study, both groups had similar reintervention rates. Two cases in the stenting group needed re-stenting at follow-up, one for aneurysm and another for stent fracture. One case in the balloon angioplasty group had restenosis who needed repeat angioplasty. They commented that although both groups’ outcomes were similar, stenting provided more predictable and uniform results.
A retrospective observational study compared the outcomes of surgery, balloon angioplasty, and stenting in various age groups. The rate of reinterventions was lowest for surgery up to 6 years and comparable for surgery and stenting in more than six years age group. The rate of reintervention after balloon dilatation was very high in all age groups. All reinterventions except one in less than six months were done surgically [55].
Management of Restenosis and Aneurysms after Coarctation of Aorta Repair
Many techniques have been used for management of restenosis after previous Coarctation of aorta repair. Balloon Angioplasty is the most favored modality of reintervention for restenosis in infants and children. It has good results and fewer complications than open repair [56, 57].
One study reported a series of 130 cases where reintervention was done after the previous Coarctation of aorta repair. The reinterventions were done at an average of 17 years after the primary procedure. Restenosis was the most common reason accounting for 94% of cases and aneurysms for the remaining. Seventy-three percent of patients underwent surgical correction, and 27% had either balloon dilation or stenting. They reported a 5 percent incidence of post-operative bleeding and vocal cord palsy in the surgery group. The surgery group had a lower second reintervention rate (4%) than the endovascular group (28%). Both the groups had good long-term survival [58]. Yetman AT, et al. [58, 59], Brown ML, et al. [60] both separately reported one case of aortic rupture during the endovascular intervention that needed conversion to an open procedure.
Although there is high rate of late aneurysm formation following balloon dilation [50, 51] for primary Coarctation of aorta, it has been observed that due to the presence of scar tissue at the recoarctation site the possibility of aneurysmal degeneration of aortic wall is less likely after balloon dilatation [2]. Restenosis after balloon dilation remains an issue that can be managed with repeat balloon dilation [9]. Hess J, et al. [61] reported that the systolic pressure gradient reduced to mean 12.5 mm Hg post-dilation from mean 27 mm Hg pre-procedure in their series. Brown JW, et al. [9] retrospectively reviewed a large series of more than a thousand cases that underwent Coarctation of aorta repair. Out of these, 10% had reintervention, either surgery or endovascular. They reported 98% long-term survival at 15 years for surgical reintervention versus 91% for the endovascular group. At a follow-up of 15 years, the second reintervention was needed in 4% and 18% surgery and endovascular group cases, respectively.
In infants and small children, synthetic patch aortoplasty and subclavian flap aortoplasty have been used for managing the recoarctation of the aorta. Dacron patch aortoplasty is associated with a high rate of late aneurysm and has fallen out of favor from the current clinical practice [15]. When balloon dilation cannot be performed for either non-availability or technical or anatomical reasons, most restenosis in infants and small children can be managed with subclavian flap aortoplasty. It has the advantage of a lower restenosis rate and can provide excellent long-term results [15]. In older children and adults who present with recoarctation where there feasibility of endovascular intervention for recurrent coarctation has been ruled out due to anatomic constraints such as involvement of arch of aorta in coarctation or long- segment coarctation, it is possible to avoid direct surgical anatomic repairs that are associated with higher morbidity and mortality by using one or other extra-anatomic bypass procedures. Grinda JM, et al. [62] reported 4 cases of recurrent coarctation among twelve other patients for primary coarctation that were treated using an extra- anatomic bypass between the left subclavian artery and descending thoracic aorta using side clamping technique via left lateral thoracotomy. There were no procedural mortality, no reoperation for bleeding, no paraparesis, and no left recurrent laryngeal or phrenic nerve palsy. They noted that this kind of bypass could be preferably in selected cases of coarctation of aorta and recoarctation to avoid the risks associated with the direct anatomic repair. Posterior Pericardial Ascending-to-Descending Aortic Bypass reported by Vijayanagar Ret al. in 1980 [63]. is another approach for managing recurrent Coarctation in older children and adults. This procedure is done under cardiopulmonary bypass. Using a Dacron graft of appropriate size, the distal anastomosis is performed on DTA by applying a side biting clamp after exposing it via posterior pericardium by retracting the heart. The proximal anastomosis to the side of ascending aorta is performed by applying a De Bakey clamp. Whereas many researchers [64, 65] have reported using this technique for complex coarctation of aorta, Connolly HM, et al. [66] identified recurrent coarctation as an indication for performing Posterior Pericardial Ascending-to-Descending Aortic Bypass in their series of 18 cases. Difficulty in direct anatomic repair and the need for other intracardiac procedures were other indications. Among the 10 cases of reintervention after previous coarctation repair was a case of post Coarctation false aneurysm, which they operated using this procedure in which they also excluded the diseased segment of DTA. One advantage of this procedure is that if indicated concomitant intracardiac procedure can also be performed. In their series, Connolly HM, et al. [66] reported early mortality and no paraplegia. There were no coarctation-related reoperations in the series over a period of 13 years follow up.
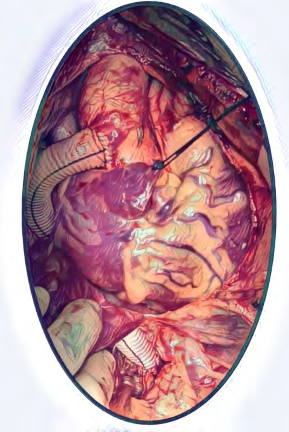
Delmo Walter EM, et al. [67] reported many approaches for extra-anatomic bypass between Ascending and Descending aorta. They documented that the use of cardiopulmonary bypass was especially helpful in the cases with anastomotic aneurysms, inadequate collaterals which they demonstrated by a fall of pressure below 50 mmHg in the aorta distal to the test clamp site or an increase in pressure proximal to the test clamp site. They reported using left heart bypass or femoro-femoral bypass for this purpose. Another extra-anatomic ascending aorta to DTA bypass for recurrent Coarctation of aorta is done via right thoracotomy without cardio pulmonary bypass. The DTA is exposed and clamped via right thoracotomy and distal anastomosis is performed and then passing the graft is passed anterior to right lung hilum and anastomosed to ascending aorta by applying a side biting clamp. Arakelyan V, et al. [68] [reported their series of cases where this procedure was performed and noted one mortality and five reoperations for lymphorrhea. They reported that all the patients became normotensive, and no complications were seen over a follow-up of average of 79 months. Ascending Aorta to Infra-diaphragmatic supra celiac aorta bypass (Ventral Aorta Repair) (Figure 1) is another extra-anatomic approach in recurrent Coarctation.
Median sternotomy is extended to upper midline laparotomy to expose the supra celiac aorta where the distal anastomosis is performed to a graft which is then brought through the diaphragm into pericardial cavity and passing by the side of right atrium it is anastomosed to ascending aorta end to side. The procedure does not include cardiopulmonary bypass, there is no dissection in the region of previous surgery, and even the usually large collateral vessels that are encountered in thoracotomy are avoided.
Kumar MV, et al. [69] reported using this technique in 25 cases of Coarctation for either of the following indications; balloon dilatation was not feasible due to associated arch hypoplasia, long-segment thoracic aorta narrowing due to nonspecific aortoarteritis or isolated long-segment Coarctation of the aorta. Three of their cases were of recurrent coarctation after surgical repair where balloon dilation was either not feasible or failed. They noted excellent results with this technique in terms of no early or late deaths and a statistically significant decrease in gradients, systolic blood pressure. Ascending to infrarenal aorta bypass is another approach where the distal anastomosis is performed to the infrarenal aorta, and proximal anastomosis is similarly performed to ascending aorta bypassing the graft through a created tunnel in the diaphragm into the pericardium. Delmo Walter EM, et al. [65] also reported adopting a combined median sternotomy and laparotomy approach with ascending aorta to abdominal aortic bypass when there is a long hypoplastic segment of aorta with recurrent aortic Coarctation. They further mentioned that this was the best approach especially in children who present with recurrent Coarctation with the largest possible graft between the ascending aorta and distal abdominal aorta, having an advantage even in children less than ten years.
Despite the high mortality and morbidity related to surgical reintervention in cases of post-coarctation aneurysms, surgical repair is indicated sometimes in cases when endovascular stenting fails or when endovascular stenting cannot be performed. Surgical repair is also indicated when there are complications related to previous endovascular stenting procedure like a persistent endo- leak or stent graft infection [2] Extra anatomic bypass are not a suitable option in these situations as there is a high risk of rupture of aneurysms, about 100 percent at 15 years, as reported by Knyshov GV, et al. [38] The surgical procedure includes replacement of the affected segment with a prosthetic graft via left lateral thoracotomy. For better exposure, single lung ventilation is used. A major concern during such an approach is spinal cord protection. Use of either Left heart bypass or full cardiopulmonary bypass via femoral artery and vein can be used. Additional measures, including topical cooling, CSF drainage, and in the post-operative phase, maintenance of adequate perfusion pressures are also helpful. In cases where it is not feasible to apply a proximal clamp on DTA either distal to LSCA or between LCCA and LSCA, open proximal anastomosis must be performed under DHCA [2].
Stenting in Recurrent Coarctation of Aorta and Aneurysms after previous Coarctation of aorta Repair TEVAR is now commonly indicated and performed for many descending thoracic aortic pathologies (Figure 2). Extension of TEVAR to native and recurrent Coarctation has been documented by many reports to be equally successful to surgical options. Forbes TJ, et al. [35] reported equally good results of stenting in native and recurrent coarctations and similar incidence of complications in the two groups. Magee AG, et al. [68] reported a series of 17 cases of Coarctation of aorta treated with expandable balloon stents. Among these there were 11 cases of recurrent Coarctation. They reported a post-stenting gradient below 10 mm Hg in all but two cases. There was access site complication in one case, the incidence of stent migration in two, and a late aneurysm degeneration at the stent site occurred in one case. They concluded that although a lower incidence in stenting is still associated with some incidence of aneurysm formation. They reported a need for re-dilation with the balloon in five cases at an average follow-up of 11 months. Surgical repair for aneurysm after previous coarctation is associated with significant mortality as high as 15 percent and morbidity including bleeding, recurrent laryngeal nerve paralysis and phrenic nerve injury. Gawenda M, et al. [69] reported a series of endovascular stenting for three cases of post-coarctation repair aneurysms. They noted good procedural success in all cases, no mortality, and exclusion of aneurysm in all. At a follow-up of 19 months, there were no stent complications.

A series of 4 cases of stenting for post-coarctation aneurysm Hormann M, et al. reported no procedural mortality and at a long-term follow-up of 71 months noted no endoleak or stent-related problems [70].
References
-
Dimitrakakis G, Challoumas D, Dimitrakaki IA (2014) eComment. Late complications after aortic coarctation repair. Interact cardiovasc Thorac surg 18(1): 133-134.
-
Beckmann E, Jassar AS (2018) Coarctation repair-redo challenges in the adults: what to do? J Vis Surg 4: 76.
-
Campbell M (1970) Natural history of Coarctation of the aorta. Br Heart J 32(5): 633-640.
-
Crafoord C, Nylin G (1945) Congenital coarctation of the aorta and its surgical treatment. J Thorac surg 14(5): 347-361.
-
Gross RE, Hufnagel CA (1945) Coarctation of the aorta: experimental studies regarding its surgical correction. New England Journal of Medicine 233(10): 287-293.
-
Waldhausen JA, Nahrwold DL (1966) Repair of Coarctation of the aorta with a subclavian flap. J Thorac Cardiovasc Surg 51(4): 532-533.
-
Vossschulte K (1961) Surgical correction of Coarctation of the aorta by an “Isthmusplastic” operation. Thorax 16(4): 338-345.
-
Kappetein AP, Zwinderman AH, Bogers AJ, Rohmer J, Huysmans HA (1994) More than thirty-five years of coarctation repair: an unexpected high relapse rate. J Thorac Cardiovasc Surg 107(1): 87-95.
-
Brown JW, Ruzmetov M, Hoyer MH, Rodefeld MD, Turrentine MW (2009) Recurrent Coarctation: is surgical repair of recurrent Coarctation of the aorta safe and effective? Ann Thorac Surg 2009 88(6): 1923-1930.
-
Yetman AT, Nykanen D, McCrindle BW, Sunnegardh J, Adatia I, et al. (1997) Balloon angioplasty of recurrent Coarctation: a 12-year review. J Am Coll Cardiol 30(3): 811-816.
-
Hijazi ZM, Fahey JT, Kleinman CS, Hellenbrand WE (1991) Balloon angioplasty for recurrent Coarctation of aorta. Immediate and long-term results. Circulation 84(3): 1150-1156.
-
Chessa M, Carrozza M, Butera G, Piazza L, Negura DG, et al. (2005) Results and mid–long-term follow-up of stent implantation for native and recurrent coarctation of the aorta. Eur Heart J 26(24): 2728-2732.
-
Serfontein SJ, Kron IL (2002) Complications of coarctation repair. In: Seminars in Thoracic and Cardiovascular Surgery: Pediatric Cardiac Surgery Annual 5(1): 206- 211.
-
Sade RM, Taylor AB, Chariker EP (1979) Aortoplasty compared with resection for Coarctation of the aorta in young children. The Annals of thoracic surgery 28(4): 346-353.
-
Kron IL, Flanagan TL, Rheuban KS, Carpenter MA, Gutgesell HP, et al. (1990) Incidence and risk of reintervention after coarctation repair. The Annals of thoracic surgery 49(6): 920-926.
-
Therrien J, Thorne SA, Wright A, Kilner PJ, Somerville J (2000) Repaired Coarctation: a “cost-effective” approach to identify complications in adults. J Am Coll Cardiol 35(4): 997-1002.
-
Marx GR (2000) “Repaired” aortic Coarctation in adults: not a “simple” congenital heart defect. J Am Coll Cardiol 35(4): 1003-1006.
-
Singh JP, Larson MG, Manolio TA, O’Donnell CJ, Lauer M, et al. (1999) Blood pressure response during treadmill testing as a risk factor for new-onset hypertension: the Framingham Heart Study. Circulation. 99(14): 1831- 1836.
-
Rao PS, Thapar MK, Kutayli F, Carey P (1989) Causes of recoarctation after balloon angioplasty of unoperated aortic coarctation. J Am Coll Cardiol 13(1): 109-115.
-
Williams WG, Shindo G, Trusler GA, Dische MR, Olley PM (1980) Results of repair of Coarctation of the aorta during infancy. JTCVS 79(4): 603-608.
-
Hesslein PS, McNamara DG, Morriss MJ, Hallman GL, Cooley DA (1981) Comparison of resection versus patch aortoplasty for repair of Coarctation in infants and children. Circulation 64(1): 164-168.
-
Dodge‐Khatami A, Backer CL, Mavroudis C (2000) Risk factors for recoarctation and results of reoperation: a 40‐year review. J Card Surg 15(6): 369-377.
-
Amato JJ, Rheinlander HF, Cleveland RJ (1977) A method of enlarging the distal transverse arch in infants with hypoplasia and Coarctation of the aorta. The Annals of thoracic surgery 23(3): 261-263.
-
Thomson JD, Mulpur A, Guerrero R, Nagy Z, Gibbs JL, et al. (2006) Outcome after extended arch repair for aortic Coarctation. Heart 92(1): 90-94.
-
Wright GE, Nowak CA, Goldberg CS, Ohye RG, Bove EL, et al. (2005) Extended resection and end-to-end anastomosis for aortic Coarctation in infants: results of a tailored surgical approach. Ann Thorac Surg 80(4): 1453-1459.
-
Pandey R, Jackson M, Ajab S, Gladman G, Pozzi M (2006) Subclavian flap repair: review of 399 patients at median follow-up of fourteen years. Ann Thorac Surg 81(4): 1420-1428.
-
Metzdorff MT, Cobanoglu A, Grunkemeier GL, Sunderland CO, Starr A (1985) Influence of age at operation on late results with subclavian flap aortoplasty. J Thorac Cardiovasc Surg 89(2): 235-241.
-
Beekman RH, Rocchini AP, Behrendt DM, Bove EL, Dick M, et al. (1986) Long-term outcome after repair of Coarctation in infancy: subclavian angioplasty does not reduce the need for reoperation. J Am Coll Cardiol 8(6): 1406-1411.
-
Ehrhardt P, Walker DR (1989) Coarctation of the aorta corrected during the first month of life. Arch Dis Child 64(3): 330-332.
-
Rothman A, Galindo A, Evans WN, Collazos JC, Restrepo H (2010) Effectiveness and safety of balloon dilation of native aortic Coarctation in premature neonates weighing≤ 2,500 grams. American Journal of cardiology 105(8): 1176-1180.
-
De Lezo JS, Pan M, Romero M, Segura J, Pavlovic D, et al. (2005) Percutaneous interventions on severe coarctation of the aorta: A 21-year Experience. Pediatr Cardiol 26(2): 176-189.
-
Rodés-Cabau J, Miró J, Dancea A, Ibrahim R, Piette E, et al. (2007) Comparison of surgical and transcatheter treatment for native Coarctation of the aorta in patients≥ 1 year old. The Quebec Native Coarctation of the Aorta Study. Am Heart J 154(1): 186-192.
-
Cowley CG, Orsmond GS, Feola P, McQuillan L, Shaddy RE (2005) Long-term, randomized comparison of balloon angioplasty and surgery for native Coarctation of the aorta in childhood. Circulation 111(25): 3453-3456.
-
Qureshi AM, McElhinney DB, Lock JE, Landzberg MJ, Lang P, et al. (2007) Acute and intermediate outcomes, and evaluation of injury to the aortic wall, as based on 15 years’ experience of implanting stents to treat aortic Coarctation. Cardiology in the young 17(3): 307-318.
-
Forbes TJ, Garekar S, Amin Z, Zahn EM, Nykanen D, et al. (2007) Procedural results and acute complications in stenting native and recurrent Coarctation of the aorta in patients over 4 years of age: A multi‐institutional study. Catheter Cardiovasc Interv 70(2): 276-285.
-
Forbes TJ, Kim DW, Du W, Turner DR, Holzer R, et al. (2011) Comparison of surgical, stent, and balloon angioplasty treatment of native Coarctation of the aorta: an observational study by the CCISC (Congenital Cardiovascular Interventional Study Consortium). J Am Coll Cardiol 58(25): 2664-2674.
-
Hernández-González M, Solorio S, Conde-Carmona I, Rangel-Abundis A, Ledesma M, et al. (2003) Intraluminal aortoplasty vs. surgical aortic resection in congenital aortic coarctation: A clinical random study in pediatric patients. Arch Med Res 34(4): 305-310.
-
Knyshov GV, Sitar LL, Glagola MD, Atamanyuk MY (1996) Aortic aneurysms at the site of the repair of Coarctation of the aorta: a review of 48 patients. Ann Thorac Surg 61(3): 935-939.
-
Von Kodolitsch Y, Aydin MA, Koschyk DH, Loose R, Schalwat I, et al. (2002) Predictors of aneurysmal formation after surgical correction of aortic Coarctation. J Am Coll Cardiol 39(4): 617-624.
-
Hehrlein FW, Mulch J, Rautenburg HW, Schlepper M, Scheid HH (1986) Incidence and pathogenesis of late aneurysms after patch graft aortoplasty for Coarctation. J Thorac Cardiovasc Surg 92(2): 226-230.
-
Rheuban KS, Gutgesell HP, Carpenter MA, Jedeikin R, Damman JF, et al. (1986) Aortic aneurysm after patch angioplasty for aortic isthmic Coarctation in childhood. Am J Cardiol 58(1): 178-180.
-
Williams WG, Wilson GJ, Coles JG, Moes CA, Hosokawa YU, et al. (1986) Synthetic patch angioplasty for repair of Coarctation of the aorta: experience with aneurysm formation. Circulation 74(3 Pt 2): I32-136.
-
Isner JM, Donaldson RF, Fulton DA, Bhan I, Payne DD, et al. (1987) Cystic medial necrosis in Coarctation of the aorta: a potential factor contributing to adverse consequences observed after percutaneous balloon angioplasty of coarctation sites. Circulation 75(4): 689- 695.
-
Heikkinen L, Sariola H, Salo J, Ala-Kulju K (1990) Morphological and histopathological aspects of aneurysms after patch aortoplasty for Coarctation. The Annals of Thoracic surgery 50(6): 946-948.
-
McGoldrick JP, Brown IW, Ross DN (1988) Coarctation of aorta: late aneurysm formation with Dacron onlay patch grafting. Ann Thorac Surg 45(1): 89-90.
-
Ala-Kulju K, Heikkinen L (1989) Aneurysms after patch graft aortoplasty for Coarctation of the aorta: long-term results of surgical management. Ann Thorac Surg 47(6): 853-856.
-
Bromberg BI, Beekman RH, Rocchini AP, Snider AR, Bank ER, et al. (1989) Aortic aneurysm after patch aortoplasty repair of Coarctation: a prospective analysis of prevalence, screening tests and risks. J Am Coll Cardiol 14(3): 734-741.
-
Krieger E, Stout K (2010) The adult with repaired coarctation of the aorta. Heart 96(20): 1676-1681.
-
Martin MM, Beekman RH, Rocchini AP, Crowley DC, Rosenthal A (1988) Aortic aneurysms after subclavian angioplasty repair of Coarctation of the aorta. Am J Cardiol 161(11): 951-953.
-
Shaddy RE, Boucek MM, Sturtevant JE, Ruttenberg HD, Jaffe RB, et al. (1993) Comparison of angioplasty and surgery for unoperated Coarctation of the aorta. Circulation 87(3): 793-799.
-
Fletcher SE, Nihill MR, Grifka RG, O’Laughlin MP, Mullins CE (1995) Balloon angioplasty of native Coarctation of the aorta: midterm follow-up and prognostic factors. J Am Coll Cardiol 25(3): 730-734.
-
Bulbul ZR, Bruckheimer E, Love JC, Fahey JT, Hellenbrand WE (1996) Implantation of balloon‐expandable stents for Coarctation of the aorta: implantation data and short‐ term results. Cathet Cardiovasc Diagn 39(1): 36-42.
-
Haji Zeinali AM, Sadeghian M, Qureshi SA, Ghazi P (2017) Midterm to long‐term safety and efficacy of self‐ expandable nitinol stent implantation for Coarctation of aorta in adults. Cathet Cardiovasc Interv 90(3): 425-431.
-
Pedra CA, Fontes VF, Esteves CA, Pilla CB, Braga SL, et al. (2005) Stenting vs. balloon angioplasty for discrete unoperated Coarctation of the aorta in adolescents and adults. Cathet Cardiovasc Interv 64(4): 495-506.
-
Früh S, Knirsch W, Dodge-Khatami A, Dave H, Prêtre R, et al. (2011) Comparison of surgical and interventional therapy of native and recurrent aortic Coarctation regarding different age groups during childhood. Eur J Cardiothorac Surg 39(6): 898-904.
-
Rao PS, Galal O, Smith PA, Wilson AD (1996) Five-to nine-year follow-up results of balloon angioplasty of native aortic Coarctation in infants and children. J Am Coll Cardiol 27(2): 462-470.
-
Yetman AT, Nykanen D, McCrindle BW, Sunnegardh J, Adatia I, et al. (1997) Balloon angioplasty of recurrent Coarctation: a 12-year review. J Am Coll Cardiol 30(3): 811-816.
-
Brown ML, Burkhart HM, Connolly HM, Dearani JA, Hagler DJ, et al. (2010) Late outcomes of reintervention on the descending aorta after repair of aortic Coarctation. Circulation 122(11 S): S81-S84.
-
Hess J, Mooyaart EL, Busch HJ, Bergstra A, Landsman ML (1986) Percutaneous transluminal balloon angioplasty in restenosis of Coarctation of the aorta. Heart 55(5): 459-461.
-
Grinda JM, Macé L, Dervanian P, Folliguet TA, Neveux JY (1995) Bypass graft for complex forms of isthmic aortic Coarctation in adults. Ann Thorac Surg 60(5): 1299- 1302.
-
Vijayanagar R, Natarajan P, Eckstein PF, Bognolo DA, Toole JC (1980) Aortic valvular insufficiency and postductal aortic Coarctation in the adult. Combined surgical management through median sternotomy: a new surgical approach. JTCVS 79(2): 266-268.
-
Wu Q, Chen X, Li H, Wang L, Xue H (2009) Ascending‐to‐ Descending Aortic Bypass via Posterior Pericardium for Complex Coarctation of Aorta. J Card Surg 24(2): 167- 169.
-
McKellar SH, Schaff HV, Dearani JA, Daly RC, Mullany CJ, et al. (2007) Intermediate-term results of ascending– descending posterior pericardial bypass of complex aortic Coarctation. The Journal of thoracic and cardiovascular surgery 133(6): 1504-1509.
-
Connolly HM, Schaff HV, Izhar U, Dearani JA, Warnes CA, et al. (2001) Posterior pericardial ascending-to-descending aortic bypass: an alternative surgical approach for complex Coarctation of the aorta. Circulation 104(12): 133-137.
-
Delmo Walter EM, Javier MF, Hetzer R (2017) Extra- anatomical bypass in complex and recurrent aortic Coarctation and hypoplastic arch. Interact Cardiovasc Thorac Surg 25(3): 400-406.
-
Arakelyan V, Spiridonov A, Bockeria L (2005) Ascending- to-descending aortic bypass via right thoracotomy for complex (re-) coarctation and hypoplastic aortic arch. Eur J Cardiothorac Surg 27(5): 815-820.
-
Kumar MV, Choudhary SK, Talwar S, Gharde P, Sahu M, et al. (2016) Extraanatomic bypass to supraceliac abdominal aorta for complex thoracic aortic obstruction. The Annals of Thoracic Surgery 101(4): 1552-1557.
-
Magee AG, Brzezinska-Rajszys G, Qureshi SA, Rosenthal E, Zubrzycka M, et al. (1999) Stent implantation for aortic coarctation and recoarctation. Heart 82(5): 600-606.
-
Gawenda M, Aleksic M, Heckenkamp J, Krüger K, Brunkwall J (2005) Endovascular repair of aneurysm after previous surgical coarctation repair. The Journal of thoracic and cardiovascular surgery 130(4): 1039-1043.
-
Hormann M, Pavlidis D, Brunkwall J, Gawenda M (2011) Long-term results of endovascular aortic repair for thoracic pseudoaneurysms after previous surgical coarctation repair. Interact Cardiovasc Thorac Surg 13(4): 401-404.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study