Effect and Significance of Electrocardiographic Changes on Standing and Hyperventilation Prior to Exercise Electrocardiographic Testing
Electrocardiographic changes on standing from supine position and subsequent hyperventilation were studied in 100 persons. Changes were correlated with any evidence of myocardial ischemia during stress and/or recovery phase of treadmill stress testing. 15 individuals showed electrocardiographic changes on standing from supine position. Increase in heart rate of more than 30 beats per minute without a fall of more than 20 mm Hg in systolic blood pressure was seen in three cases. Two of them developed ischemic changes during exercise. Decrease in R wave amplitude in leads V2 to V6 was seen in one individual who developed ischemic changes during exercise. New inversion of T waves in leads V2 to V4 in a case with pre-existing RBBB and inverted T wave becoming positive in lead V2 were also associated with electrocardiographic evidence of myocardial ischemia during exercise testing. Mild change in QRS axis, decrease in R wave amplitude in leads II, III, aVF and/or V3 to V5 , ST segment depression of less than 1 mm and decrease in amplitude or inversion of T waves in leads II, III, aVF and V1 to V6 did not have any correlation with evidence of myocardial ischemia during exercise. Fourteen persons showed new electrocardiographic changes during hyperventilation after standing. Three cases had decrease in heart rate. All the three had evidence of myocardial ischemia during treadmill testing. Increase in amplitude of R wave in lead V4, normalization of pre-excitation with unmasking of old myocardial infarction and ST segment depression of more than 2 mm in inferior and lateral precordial leads with ST segment elevation in lead aVR were also associated with development of ECG evidence of myocardial ischemia during treadmill testing. Decrease in R wave amplitude in leads II, III, aVF and/or V4 - V6 , ST segment depression of less than 1mm in inferior or lateral precordial leads and inversion of T waves did not have any significant correlation with development of electrocardiographic signs of myocardial ischemia during treadmill stress test.
Introduction
A treadmill stress test is performed in the standing position and the respiratory rate of patients increases linearly with increasing duration of exercise. Standing from supine position and hyperventilation are known to produce electrocardiographic changes that may mimic or mask myocardial ischemia [1, 2]. Clinical significance of changes in supine versus upright body position is not clear [1, 3]. Markendorf, et al. did not exclude patients with cardiac disease and excluded leads III, aVR and V1 from the analysis. Khare and Chawla, [3] studied only 30 adults aged 18 to 25 years and studied only limb leads. In both the studies, exercise stress test was not performed to find any correlation of observation with exercise-induced ischemia. There is no consensus regarding the utility of hyperventilation prior to exercise. Some authorities feel that it does not provide additional useful information [4, 5]. Others, however, feel that a period of hyperventilation prior to the stress test can distinguish the ST segment changes caused by hyperventilation induced alkalosis from those resulting from ischemia due to coronary artery disease [6]. We, therefore, evaluated the electrocardiographic effect of standing from supine position and hyperventilation prior to exercise and correlated them with the results of the exercise stress test in the same patients [7]. Material and Methods All patients presenting for treadmill stress test over a period of six months were evaluated.
Exclusion Criteria
Following patients were excluded from study
- Patients with any contraindication for the exercise stress test.
- Abnormalities are suggestive of myocardial ischemia in resting electrocardiogram.
- Presence of left bundle branch block in resting ECG.
- Patients who could not perform hyperventilation.
- Patients who could not perform the adequate exercise. Electrocardiogram was recorded after lying in the supine position for five minutes, after standing and again after hyperventilation for one minute. A treadmill test was performed using Bruce protocol [8]. Symptom limited exercise was used as the endpoint rather than targeting at attaining a target heart rate [9, 10].
Electrocardiographic Analysis
One hundred patients (56 males and 44 females) were included in the final electrocardiographic analysis. Changes in the following electrocardiographic parameters were analysed.
- Heart rate
- Configuration and amplitude of P wave specially in lead II and V1
- P-R segment
- P-R interval
- QRS- mean frontal plane axis, R wave amplitude specially in leads III, aVR and V5, S wave depth specially in leads V1 and V2, the new appearance of any bundle branch block.
- ST-segment - elevation or depression (configuration of ST-segment depression and magnitude of depression at J point and 80 milliseconds after J point).
- T wave - especially change in T wave polarity and change in amplitude of T wave in leads V1 and V2.
- U wave polarity.
- Only manually measurable changes were recorded. Computerised analysis was not performed
Following Parameters were not Analysed
- Change in P wave duration. It needs computerized signal average ECG and several times magnification of ECG [10].
- Change in QT interval - Manual measurement of the correct QT interval is challenging because of correct identification of end of T wave, determining which lead to use and connecting the measured interval for heart rate, QRS duration and sex [11, 12]. Further the QT interval varies from lead to lead by as much as 50 to 60 milliseconds (QT dispersion) [12]. Automated ECG systems measure QT interval from a composit of all leads. Such facility is not available in currently available treadmill stress test systems
- Change in QRS axis was considered mild if it was less than 300 T wave inversion of 1 mm or less was considered “shallow”. ST-segment depression of less than 1mm was labelled as mild.
- Changes were correlated with any change in the ST segment during exercise or recovery, which was considered diagnostic of myocardial ischemia.
- 1 mm of horizontal or downsloping ST-segment depression or an upsloping ST segment that was depressed >1.5 mm below the isoelectric line 80 milliseconds after the J point, during exercise or recovery, were considered indicative of exercise-induced ischemia [11].
Results
Fifteen patients (Eight males and seven females) showed electrocardiographic changes on standing from the supine position. Fourteen patients (Seven males and seven females) showed electrocardiographic changes after hyperventilation.
Electrocardiographic Changes on Standing from the Supine Position
Heart Rate: It increased in all cases. The increase in heart rate ranged from 2 beats/minute to 28 beats per minute. The magnitude of increase in heart rate decreased with advancing age. There was no relation to sex. The magnitude of increase in heart rate had no relation to ischemic changes during exercise. P Wave, P-R Segment and P-R Interval: There was no appreciable change in any patient.
QRS • Mean Frontal Plane QRS Axis: Three patients showed mild deviation to left. Representative
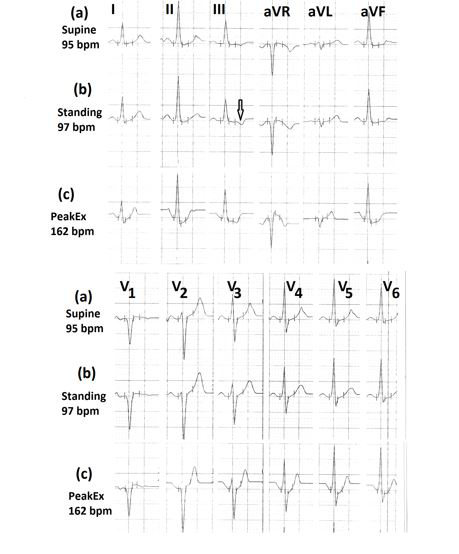
electrocardiographic tracing from one patient is shown in Figure 1b. This patient showed ST-segment depression suggestive of myocardial ischemia during exercise (Figure 1c). • Amplitude of the R Wave: Seven patients showed a decrease in height of R waves in leads II, III, aVF and/ or leads V5 to V6 (Figure 2 marked ). Only one of these patients showed ischemia changes during exercise (Figure 2a,b,c). Two cases showed an increase in R
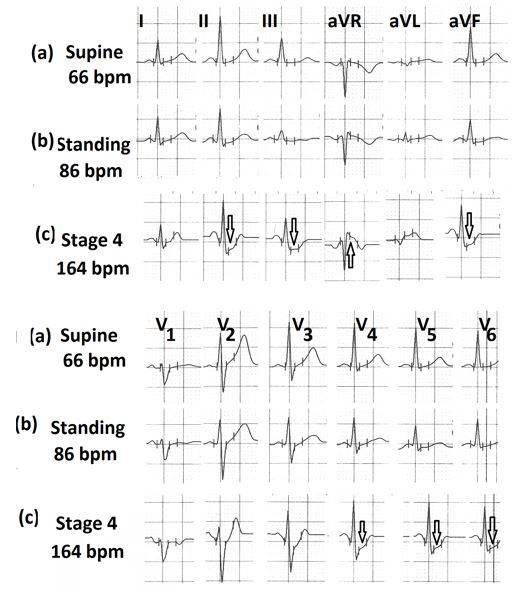
wave amplitude in leads I and /or aVL, in addition, to a decrease in amplitude of R wave in leads III, aVF and V2 to V6. One had a negative exercise electrocardiogram and one had a positive exercise electrocardiogram (Figure 1). One patient had a decrease in R wave amplitude only in leads V2 to V4 (Figure 3b, marked⇓). He developed downsloping ST-segment depression during recovery (Figure.3c, marked∗).
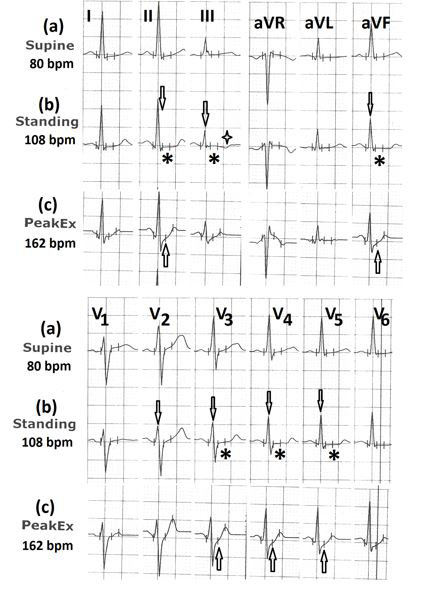
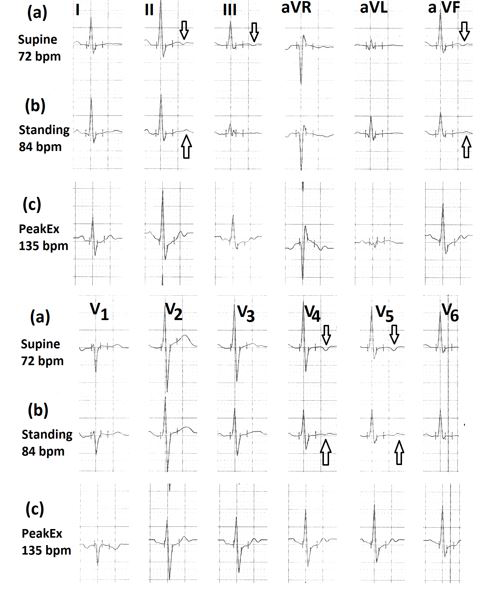
Figure 2: Electrocardiograms (a) In the supine position; (b) In standing position showing the decrease in amplitude of R wave (marked⇓ ) with horizontal ST segment (marked∗ ) in leads II, III, aVF and V2 to V5 and T wave inversion in lead III (marked ⇑); (c) during peak exercise showing upsloping ST-segment in leads II, aVF, V3 to V5 (marked ).
ST-Segment: In one patient ST-segment becomes horizontal in leads I, II, aVF, V4, V5 and V6. However, there were no signs of ischemia on exercise (Figure 2). One patient developed minimal (less than 1mm) ST-segment depression in leads I,
V3, V4, V5 (Figure 4b, marked⇓). On exercise, there was an increase in ST-segment depression in leads V2 to V4 (Figure 4c, marked∗).
T Wave: One patient had mild T wave inversion in lead III in the supine position which increased on standing. The exercise was negative. One patient developed increased T wave inversion in lead III (Figure 5b, marked⇓) which persisted during hyperventilation and exercise. There was no evidence of ischemia on exercise (Figure 5c). Two
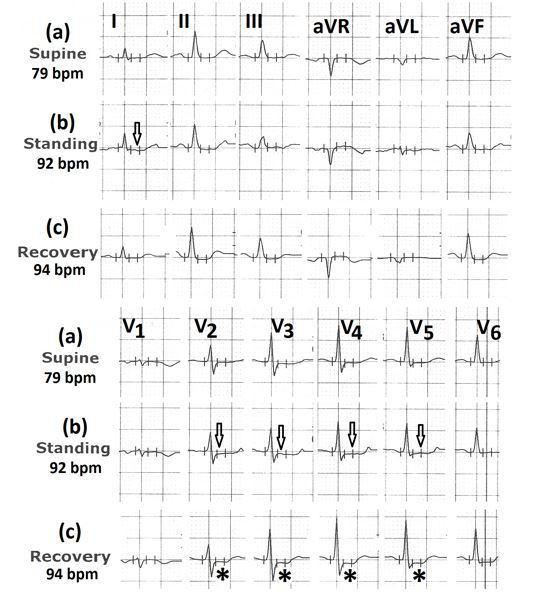
patients developed T wave inversion in inferior leads and leads V4 to V6. In one patients (39 years old female) T wave become normal on exercise (Figure 6c, marked⇑) without any ST-segment depression (Figure 6d). Another patient (30 years old female) who developed T wave inversion in leads II, III, aVF and V3 to V6 on standing (Figure 7b, marked⇓) developed ST-segment depression in leads I, II, III, aVF, V4, V5 and V6 (Figure 7c, marked∗) with ST-segment elevation in lead aVR (Figure 7 marked⇑) and partial normalization of T wave inversion in lead V1 (Figure 7, marked ) at peak exercise. Changes normalized in less than one minute (Figure 7d). In one patient, a supine electrocardiogram showed T wave inversion in leads V1 to V3. On standing T wave inversion also
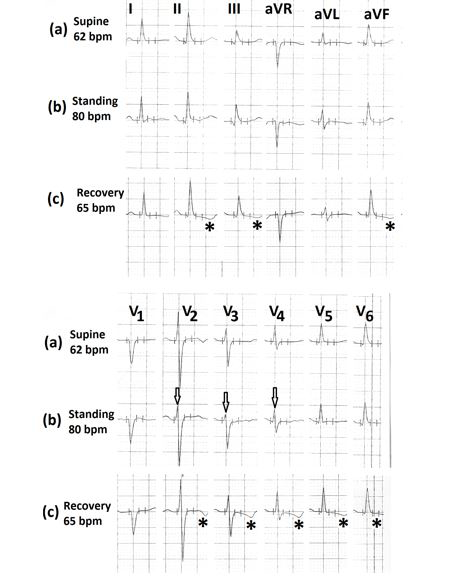
appeared in lead V4. There was no fresh change in exercise. One patient had a right bundle branch block with T wave inversion in leads aVR and V1 in the supine position (Figure 8a). On standing new T wave inversion appeared in leads V2, V3 and V4 (Figure 8b marked⇓) with horizontal ST segment in leads V5 and V6. During the third minute of recovery, patient developed a downsloping ST-segment in leads V4 to V6 (Figure 8c marked∗). Two patients had shallow T wave inversion in inferior and lateral precordial leads (Figure 9a, marked⇓) which normalised on standing. (Figure 9b, marked⇑). There was no evidence of ischemia on exercise (Figure 9c) Figure 5: Electrocardiograms (a) in supine position showing mild inversion of T wave in lead III; (b) in standing position showing the increase in the magnitude of T wave inversion in lead III (marked⇓); (c) during peak exercise showing absence of any ST-segment depression.
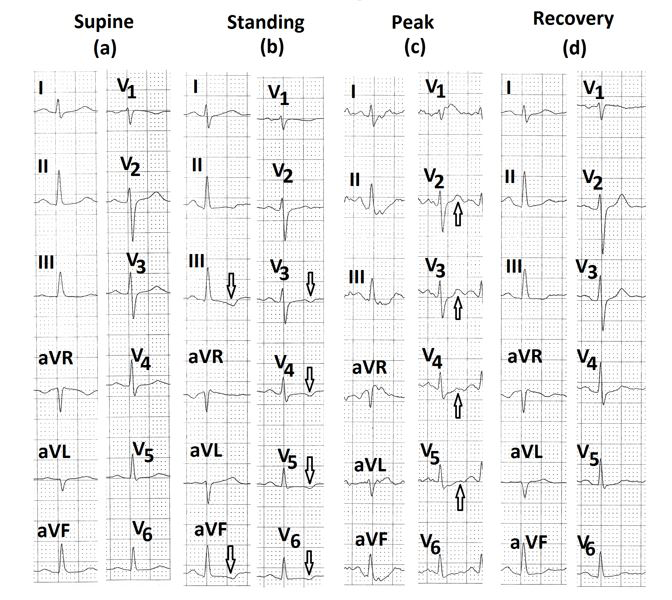
Figure 6: Electrocardiograms (a) in the supine position; (b) in standing position showing less than 1mm T wave inversion in leads III, aVF and V2 to V6 (marked⇓); (c) during stage 3 of Bruce protocol showing normalization of T waves in leads V2 to V5 (marked⇑); (d) during the third minute of recovery showing absence of any ST-segment depression.
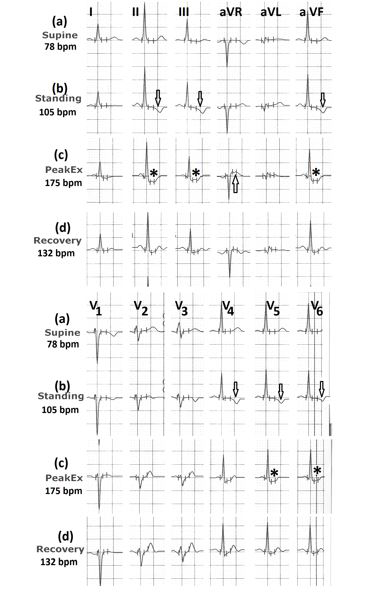
Figure 7: Electrocardiograms (a) in the supine position; (b) in standing position showing T wave inversion up to 2mm in leads II, III and V3 to V6, marked ⇓; (c) during peak exercise showing significant ST-segment depression in leads II, III, aVF, V5, V6 (marked ∗) with ST-segment elevation in lead aVR (marked⇑); (d) showing normalization of ST-segment changes within one minute of recovery.
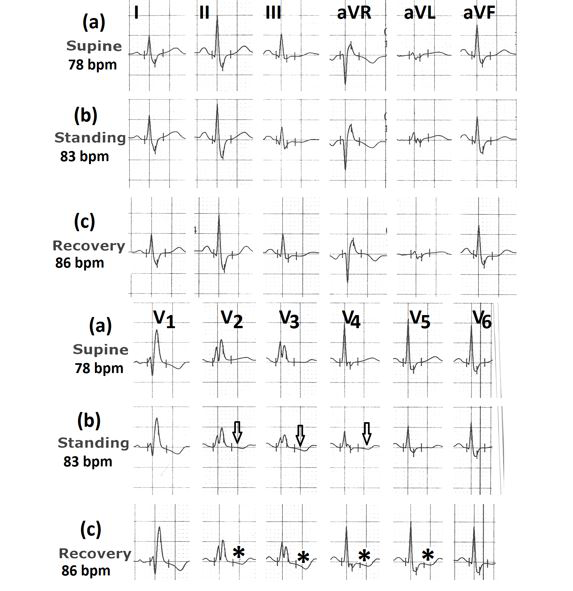
Figure 8: Electrocardiograms (a) in supine position showing RBBB with T wave inversion in lead V1 and positive T waves in leads V2 to V6; (b) in standing position showing T wave inversion in leads V2 to V4 (marked⇓) and horizontal ST segment in leads V5 and V6; (c) during 3rd minute of recovery, showing downsloping ST-segment depression in leads V2 to V5 (marked
U Wave: U wave was visible in two cases in supine ECG. There was no change in standing. The number of patients showing various electrocardiographic changes on standing from supine position and their correlation with the presence or absence of significant ST-segment depression during exercise is shown in Table 1.
| Electrocardiographic Change (Total patients-15) | Number of patients showing ischemic ST-segment depression during exercise | |
|---|---|---|
| Increase in heart rate (beats/Minute) | Absent | Present |
| < 5 | 2 | 1 |
| 5 to 10 | 1 | 1 |
| 10 to 20 | 5 | 2 |
| > 20 | 1 | 2 |
| Change in mean frontal plane QRS axis | ||
| Mild LAD | 2 | 1 |
| Change in R wave amplitude | ||
| Decrease in leads II, III,aVF and/or V3toV5 | 6 | 1 |
| Increase in lead I and/or aVL with decrease in inferior leads | 1 | 1 |
| Decrease in leads V2 to V4 | 0 | 1 |
| ST-segment depression less than 1mm in leads I, aVL, V4 to V6 | 1 | 0 |
| Horizontal ST in leads I, II, aVF, V4 to V6 | 1 | 0 |
| Change in T wave | ||
| Decreased amplitude or inversion in leads | 3 | 1 |
| II, III, aVF, V1 to V6 | ||
| Increased inversion in lead III | 1 | 0 |
| Shallow inversion in leads V5, V6 | 2 | 0 |
| RBBB- new inversion in leads V2 to V4 | 0 | 1 |
| Inverted T wave in lead V2 becoming positive | 0 | 1 |
| Normalization of shallow inversion in leads | 2 | 0 |
| II, III, aVF, and V4 to V6 |
Table 1: Correlation of electrocardiographic changes on standing from a supine position with ischemic ST-segment depression durin
Electrocardiographic Changes during Hyperventilation
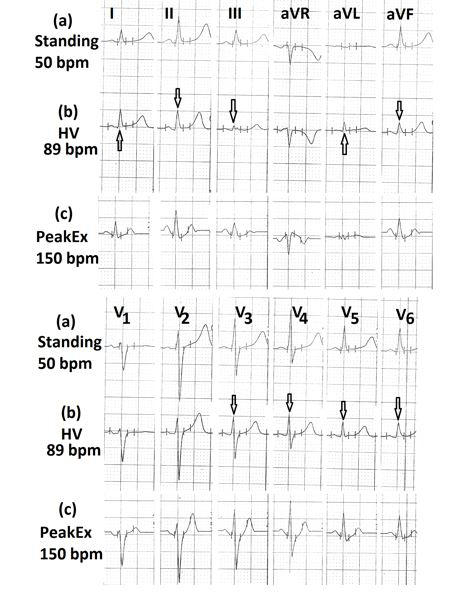
Heart Rate: Three patients had a mild decrease in heart rate (3 beats/minute in one patient and 5 beats/minute in another two patients). All showed ischemic ST-segment depression during exercise - two in leads V3 to V5 (Figure 10c, marked ∗ ) and one in inferior leads with (Figure 11c marked⇓) and ST-segment elevation in lead aVR (Figure 11c marked⇑).

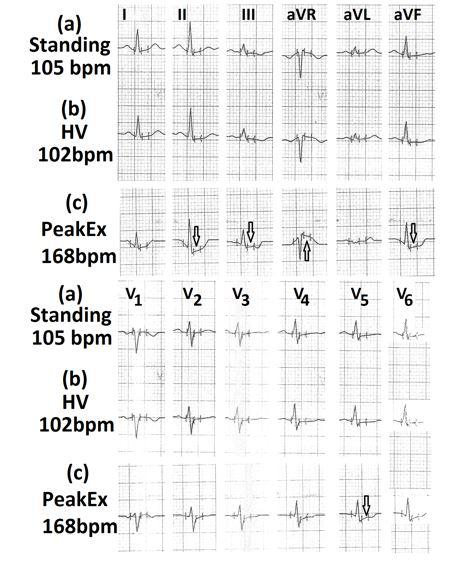
One patient had an increase in heart rate by seven beats/ minute. He developed an increase in the amplitude of R wave and T wave inversion in lead V4 during hyperventilation (Figure 12b, marked⇓). During exercise, he developed ischemic ST-segment depression in leads V4 to V6 (marked ∗) and shallow T wave inversion in inferior leads (Figure 12c, marked ) In one patient heart rate increased by fifty- one beats/minute (from 102 beats/minute in the standing position to 153 beats/minute during hyperventilation). It exceeded the age-adjusted target heart rate of 143 beats/ minute. The patient developed significant ST-segment depression in leads I, II, III, aVF and V2 to V6 (Figure 13c, marked⇓) and ST-segment elevation in lead aVR (Figure 13c marked⇑). Changes increased during exercise (Figure 13d, marked∗). In the remaining nine patients, heart rate increased by 8 beats/minute to 39 beats/minute during hyperventilation. Three patients had ischemia ST-segment depression during exercise.
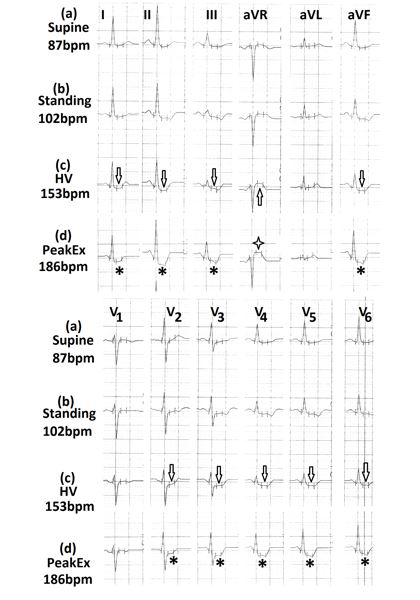
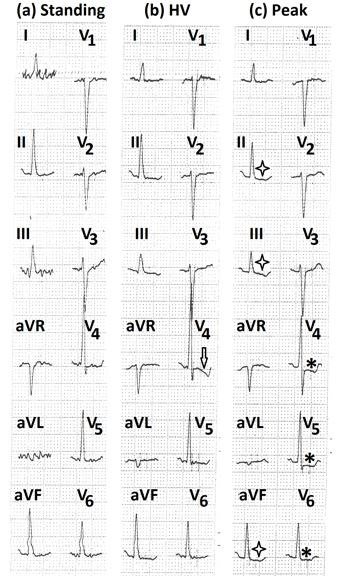
Figure 13: Electrocardiograms (a) in the supine position, showing minimal ST-segment depression in leads II, III,aVF, V4 to V6; (b) in standing position showing the increase in heart rate by 15 beats/minute and mild ST- segment depression and shallow T wave inversion in leads II, III,aVF, V3 to V6; (c) during hyperventilation, showing a further increase in heart rate by 51 beats/minute with the increase in ST-segment depression in leads I, II, III, aVF V2 to V6 (marked ⇓), and ST-segment elevation in lead aVR (marked⇑ ); (d) during peak exercise, showing a further increase in ST-segment depression in leads I, II, III, aVF, V2 to V6 (marked∗ ) and elevation in lead aVR (marked $$ + $$ ).
P Wave, P-R Segment and P-R Interval: There was no appreciable change in any patient. QRS Mean Frontal Plane QRS Axis: One patient had mild deviation to left and another patient had mild deviation to right. Both the patients did not have evidence of ischemia during exercise or recovery. One patient had pre- excitation in supine ECG (Figure 14a) which disappeared in hyperventilation (Figure 14b). During recovery, the patient developed deep symmetrical T wave inversion in leads II, III, aVF and V6 (Figure 14c, marked⇓) with significant ST segment depression in leads V5 and V6 (Fig.14 c, marked∗). R wave amplitude increased in lead V4 in one patient (Figure 12). On exercise, there was ST-segment depression in leads V4 to V6. In one patient R wave amplitude increased slightly in leads III, aVF and decreased slightly in lead aVL. There was no evidence of ischemic on exercise. In seven patients R wave
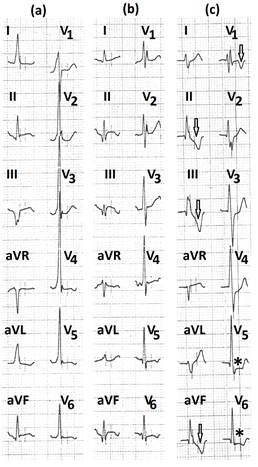
Figure 14: Electrocardiograms (a) in supine and standing position, showing pre-excitation; (b) during hyperventilation, showing the disappearance of pre-excitation and appearance of Q wave with ST-segment elevation in leads II, III, aVF; (c) during recovery, showing deep symmetrical T wave inversion in leads II, III, aVF, V1 (marked ⇓) and significant ST-segment depression in leads V5 and V6 (marked ∗).
amplitude decreased in inferior and/or precordial leads (Figure 15). Only two patients had evidence of ischemia on exercise.
ST-Segment: Two patients had less than 1mm ST-segment depression during hyperventilation. There was no evidence of ischemia during exercise. One patient had ST-segment depression in inferior leads (II, III,aVF) and lateral precordial leads (V3 to V6) on standing (Figure 16a). ST-segment depression increased during hyperventilation (Figure 16b marked⇓). ST-segment became elevated in lead aVR (Figure 16b marked⇑) He developed increased ST-segment depression during exercise (Figure 16c, marked∗) with the elevation of ST-segment in lead aVR (Figure 16c, marked ). One patient had ST-segment depression in leads II, III,aVF, V3 to V6 with ST-segment elevation in lead aVR in the supine position. Changes increased during hyperventilation but there was no further change during exercise.
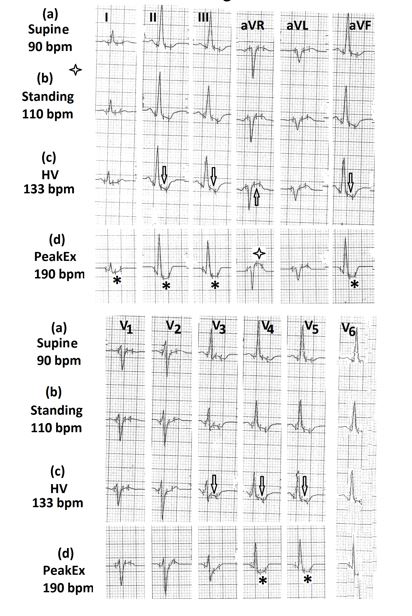
Figure 16: Electrocardiograms (a) in supine position showing mild ST-segment depression and T wave inversion in leads II, III, aVF, V5 to V6; (b) in standing position, showing the mild increase in T wave inversion; (c) during hyperventilation, showing a further increase in ST-segment depression in leads II, III, aVF, V4 to V6 (marked⇓) and ST-segment elevation in lead aVR (marked⇑); (d) during exercise, showing significant ST-segment depression in leads I, II, III, aVF, V4 to V6 (marked∗ ) and ST-segment elevation in lead aVR (marked $$ + $$ ) T Wave: In one patient, fresh, shallow T wave inversion appeared in leads III, aVF, V3 to V5 during hyperventilation (Figure 17b, marked ⇓ ). The polarity of T waves become normal during exercise (Figure 17c, marked⇑) but ST- segment depression appeared in leads V2 to V5 during recovery (Figure 17c, marked ∗ ). Another patient who developed shallow T wave inversion in leads V3 and V4 during hyperventilation also developed downsloping ST-segment depression during recovery. One person developed shallow T wave inversion in leads V1 only. No new changes appeared during exercise.
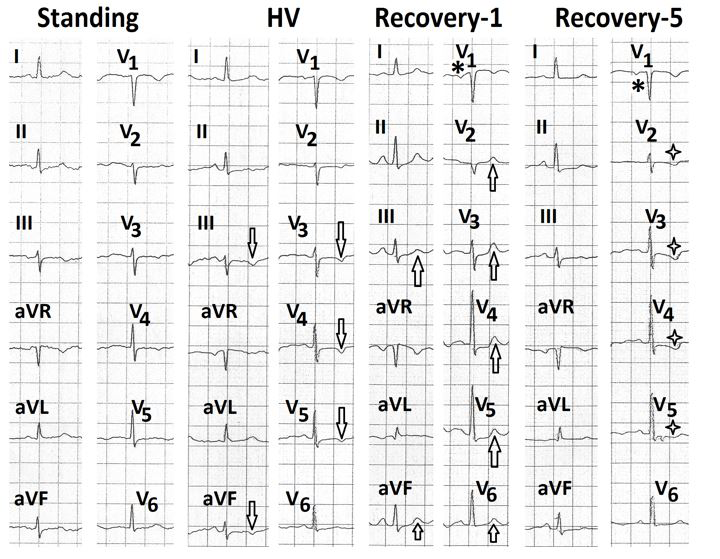
Figure 17: Electrocardiograms (a) during standing position, (b) during hyperventilation showing shallow T wave inversion in leads III, aVF, V2 to V5 (marked⇓); (c) during the first minute of recovery showing positive T waves in leads III, aVF, V2 to V5 (marked⇑) and negative terminal deflection of P wave in lead V1 (marked∗); (d) during 5th minute of recovery showing inverted P wave in lead V1 (marked∗) and downsloping ST-segment depression in leads V2 to V5 (marked U Wave: U wave was visible in two cases in the supine position. There was no change during hyperventilation. The number of patients showing various electrocardiographic $$ + $$ ).
changes during hyperventilation and their correlation with the presence or absence of significant ST-segment depression during exercise is summarised in Table 2.
| Electrocardiographic Change (Total patients 14) | Number of patients showing ischemic ST- segment depression during Exercise | |
|---|---|---|
| Change in heart rate (beats/Minute) | Absent | Present |
| Increase | ||
| 5 to 10 | 1 | 1 |
| 10 to 20 | 3 | 1 |
| 20 to 30 | 0 | 2 |
| > 30 | 2 | 1 |
| Decrease | 0 | 3 |
| Change in Mean Frontal Plane QRS axis | ||
| Mild RAD | 1 | 0 |
| Mild LAD | 1 | 0 |
| Change in R Wave Amplitude | ||
| Decrease in leads II, III,aVF and/or V4-V6 | 5 | 2 |
| Increase in lead V4 | 0 | 1 |
| Increase in leads III,aVF and decrease in lead aVL | 1 | 0 |
| Normalization of pre-excitation with unmasking of old inferior infarction | 0 | 1 |
| ST-Segment Depression | ||
| less than 1mm in leads II, III,aVF | 1 | 0 |
| less than 1mm In leads V4-V6 | 1 | 0 |
| More than 1mm in inferior and lateral precordial leads with elevation in aVR | 0 | 2 |
| Change in T Wave | ||
| Inversion in inferior and/or lateral precordial lead | 4 | 2 |
| Shallow T wave inversion in lead V1 | 1 | 0 |
Table 2: Correlation of new electrocardiographic changes during hyperventilation after standing with ischemic ST-segment depressi
Sum of Electrocardiographic Changes Observed During Standing and/or Hyperventilation
Heart Rate: A total of twenty-six cases had an increase in heart rate. Out of these eleven cases had significant ST- segment depression during exercise. Three cases had a decrease in heart rate during hyperventilation. All three had significant ST-segment depression during exercise. Change in Mean Frontal Plane QRS Axis: A total of five patients had a deviation of less than 300. Only one case had significant ST-segment depression on exercise. P wave, P-R Segment, P-R Interval: None of the patients had any measurable change. Change in R Wave: A total of fourteen patients had a decrease in R wave amplitude in leads II, III, aVF and/or leads V3 to V6. Only three cases had significant ST-segment depression during exercise. Two patients had a decrease in R wave amplitude in leads II, III, aVF with the increase in R wave amplitude in leads I and/or aVL. One patient had significant ST-segment depression during exercise. One patient had an increase in R wave amplitude in leads III, aVF with the decrease in lead aVL. There was no significant ST-segment depression on exercise. One patient had a decrease in R wave amplitude only in leads V2 to V4. There was no ST-segment depression during exercise. In one patient pre-excitation disappeared during hyperventilation with the unmasking of old inferior myocardial infarction there was significant ST- segment depression during exercise. ST-Segment: One patient developed a horizontal ST segment in leads V4 to V6. There was no ST-segment depression during exercise. A total of three patients developed ST-segment depression of less than 1mm. None of these developed significant ST-segment depression during exercise. Two cases developed ST-segment depression of more than 1 mm in inferior and lateral precordial leads with ST-segment elevation in lead aVR during hyperventilation. Both had significant ST-segment depression during exercise. T Wave: A total of fourteen patients showed decreased amplitude or inversion of T waves in inferior and/or precordial leads. Only three of these patients developed significant ST-segment depression during exercise. In one patient negative T wave in lead V1 became positive on standing. This patient had significant ST-segment depression during exercise. In one patient with the right bundle branch block, fresh T wave inversion appeared in leads V2 to V4 on standing. This patient had significant ST-segment depression during exercise. U Wave: U wave was visible in the supine position in two cases. There was no change during standing or hyperventilation. Observations are summarized in Table 3.
| New electrocardiographic findings | Total Number of Cases Showing Change During Dtanding and/or Hyperventilation | Number of Cases with Positive Exercise ECG | Number of the Case with Negative Exercise ECG |
|---|---|---|---|
| Increase in heart rate | 26 | 11 | 15 |
| Decrease in heart rate during hyperventilation | 3 | 3 | 0 |
| Decrease in R wave amplitude in leads II, III, aVF and/or V to V 3 6 | 14 | 3 | 11 |
| Increase in R wave amplitude with T wave inversion in lead V 4 | 1 | 1 | 0 |
| ST-segment depression in leads II, III, aVF, V to 3 V with ST-segment elevation in aVR 6 | 3 | 3 | 0 |
| Decreased amplitude or inversion of T wave in inferior and/or precordial leads | 14 | 3 | 11 |
| Normalization of shallow T wave inversion in leads II, III, aVF, V to V 4 6 | 2 | 0 | 2 |
| Pre-excitation - the unmasking of old inferior MI | 1 | 1 | 0 |
| RBBB - new T wave inversion in leads V to V 2 4 | 1 | 1 | 0 |
Table 3: Correlation of sum of important electrocardiographic changes during standing and/or hyperventilation with significant ST
Discussion
Electrocardiographic Changes on Standing from the Supine Position
Heart Rate: Heart rate increased on standing from the supine position. Previous workers have also observed this finding [1, 14, 15]. On standing, there is a gravity-mediated pooling of about 300 to 800 ml of blood in the lower extremities and inferior mesenteric area. Venous return and stroke volume decrease. This result in a transient fall in blood pressure. It leads to a reflex increase in sympathetic activity which causes peripheral vasoconstriction and an increase in heart rate to maintain cardiac output. Normally, the heart rate increases by 10 to 15 beats/minute [15]. Failure of compensatory vasoconstriction results in a greater increase in heart rate on standing from the supine position. This results in inter- individual variability in the increase in heart rate on standing from the supine position. An increase of more than 30 beats/minute in absence of a fall of more than 20 mm Hg in systolic blood pressure is considered abnormal [16, 17]. We observed that persons with a heart rate increase of more than 20 beats/minute were more likely to have significant ST-segment depression during exercise. Previous workers have not correlated change in heart rate with any evidence of ischemia [1, 14, 15]. It is however important to remember that anxiety, inappropriate sinus tachycardia and postural orthostatic tachycardia syndrome are more common causes of abnormal increase in heart rate on standing from the supine position [16]. P Wave, P-R Segment and P-R Interval: We did not find any measurable difference in these parameters on standing from the supine position. Khare and Chawla [15] also did not find any significant difference in mean P wave axis and amplitude on standing from the supine position. There is no literature on the effect of standing on the P-R segment. Madias [18] also observed that standing did not affect the P-R interval. Mean Frontal Plane QRS Axis: Only three patients showed less than 300 deviations to left in the mean frontal plane QRS axis. One person had a positive exercise ECG. This number is too small to make any useful conclusion. Standing position is expected to result in a rightward shift of the QRS axis due to the relatively vertical anatomical position of the heart. However, previous workers have also observed no significant difference in the mean frontal plane QRS axis on standing from the supine position [15, 18]. Change in R Wave Amplitude: Nearly 50% of patients showed a decrease in amplitude of R wave in inferior and/or lateral precordial leads. One of them showed significant ST- segment depression during exercise. Two patients showed an increase in R wave amplitude in leads I and aVL. One patient had significant ST-segment depression during exercise and recovery. One patient had a decrease in R wave amplitude in leads V2 to V4. This patient had significant ST-segment depression during exercise. Changes in R wave amplitude in lead V5 during exercise and recovery have been correlated with the presence or absence of ischemia [13]. However, these changes have not been found to have any predictive value [19]. There is no literature about the effect of standing on R wave amplitude in different leads and its clinical significance. We do not have any satisfactory explanation about these changes in R wave amplitude on standing. These can not be explained by any change in the anatomical position of the heart for two reasons. Firstly, there is no true change in anatomical position of the heart with posture and even if it occurs, it is minimal [20]. Secondly, if the changes were related to the anatomical position of the heart (i.e. heart becoming more vertical in standing position, R wave voltage should increase rather than decrease in inferior leads and standing. We feel that these changes reflect changes in direction of ventricular depolarization ant its relation to different leads in a given individual. These changes in R wave amplitude do not correlate with the presence or absence of underlying myocardial ischemia. ST-Segment Changes: We observed mild (<1mm) ST- segment depression in leads I, aVL and V3 to V6 in one patient. There was no evidence of myocardial ischemia on exercise. Markendorf, et al. [1] also observed ST-segment depression in 0.2% of their patients on standing from the supine position. They also did not observe increased ischemic potential in these patients. Other authorities have also observed such mild ST-segment depression on change of posture [12]. It is advised that such changes should not be over-interpreted [12]. Significance of such changes should be decided only in the context of protest probability of ischemic heart disease [11]. Sympathetic overdrive and neurocirculatory asthenia can also cause mild ST-segment depression on standing. Changes in T Waves: Decreased amplitude or inversion of T waves in inferior leads (II, III, aVF) and /or lateral precordial leads (V3 to V6) was seen in seven cases. Only one patient had significant ST-segment depression during exercise. Markendorf, et al. [1] observed T wave inversion in leads I, II, aVL, aVF and V2 to V6 in 14.7% of their patients. They excluded changes in leads III, aVR and V1 from the analysis. They felt that these changes could mimic ischemic heart disease. However, they did not perform exercise stress tests or coronary angiography to find any correlation. In two of our cases, shallow T wave inversion became upright on standing. In 5.4% of patients studied by Markendorf, et al. [1] inverted T waves became upright. Chawla and Khare [15] analyzed only mean T wave amplitude. They did not study precordial leads and did not study T wave changes in each of the limbs leads separately. It appears that T wave changes on standing are usually nonspecific and do not perse suggest myocardial ischemia. One patient had a right bundle branch block with T wave inversion in lead V1 in the supine position. On standing new T wave inversion appeared in leads V2, V3 and V4 with horizontal ST segment in leads V5 and V6. During the third minute of recovery, there was downsloping ST-segment depression in leads V4 to V6. In the context of the right bundle branch block, ST depression in leads V1 to V3 during exercise is not associated with ischemia [21]. However, ST-segment depression in leads II, aVF and V4 to V6 is considered suggestive of ischemia [5, 19]. There is no literature on the effect of standing on T waves and their significance in patients with right bundle branch block. This area needs to be explored.
Electrocardiographic Changes During Hyperventilation over those Observed on Standing
Change in Heart Rate: There was a further increase in heart rate during hyperventilation over the heart rate in standing position. The increase ranged from less than 5 beats/minute to more than 30 beats/minute. One patient crossed his age-adjusted predicted maximal heart rate. He developed ST-segment changes diagnostic of myocardial ischemia. Enger, et al. [22] have also observed sinus tachycardia during hyperventilation. Hyperventilation syndrome is also associated with sinus tachycardia [2]. Release of excitatory neurotransmitters from the brain is probably responsible. Lowered arterial carbon dioxide concentration also results in splanchnic vasodilation via inhibition of the vasomotor centre [23]. Resulting drop in venous return results in reduced ventricular filling, decreased stroke volume and a reflex increase in heart rate. We observed significant inter-individual variation in heart rate response to hyperventilation. This is probably related to inter-individual variation in rate and depth of respiration. Three of our patients had a decrease in heart rate during hyperventilation. All had significant ST-segment depression during exercise. Wasserburger, et al. [24] have shown that hyperventilation can produce a vagal reflex in the thorax, similar to the Hering-Bruer reflex. Ardissino, et al. [25] have also suggested that hyperventilation can cause a vagally mediated reduction in coronary flow. This mechanism could contribute to the higher incidence of significant ST-segment depression during exercise amongst a patient who had a reduction in heart rate during hyperventilation. Changes in Mean Frontal Plane QRS Axis: Only two patients had deviation in mean frontal plane QRS axis. The change was less than 300 in both cases. This change had no clinical significance. Changes in R Wave Amplitude: Nine patients had a new change in R wave amplitude. Seven had a decrease in R wave amplitude in leads II, III, aVF and/or leads V4 to V6. This could be due to hyperinflation of the lungs during deep breathing. Out of these seven patients, two had significant ST-segment depression during exercise. The heart rate of these patients during hyperventilation was 133 beats/ minute and 153 beats/minute respective. In the remaining five patients, heart rate during hyperventilation ranged from 85 to 120 beats/minute during hyperventilation. One patient had an increase in R wave amplitude in leads III, aVF and a decrease in R wave amplitude in lead aVL. There was no change during exercise. One person had an increase in R wave amplitude in lead V4. During exercise, there was significant ST-segment depression. Thus we observed that decrease in R wave amplitude in leads II, III, aVF and V4 to V6 was frequent during hyperventilation but had low specificity for diagnosing ischemia. The only patient who had an increase in R wave height in lead V4 had evidence of ischemia on exercise. His heart rate during hyperventilation was 101 beats/minute. Balady and Morise [26] have concluded that R wave amplitude normally increases during exercise. On the other hand, Thomas, et al. [13] observed that R wave amplitude in lead V5 decreases if a heart rate of 120 to 130 beats/minute was achieved. There is no literature on the effect of hyperventilation on R wave amplitude in different leads. We did not observe any relation of heart rate with change in R wave amplitude during hyperventilation. Changes in ST-Segment: We observed ST-segment depression of less than 1mm in inferior leads or lateral precordial leads in two cases. Both cases did not have any evidence of ischemia during exercise. Thus we observed that ST-segment depression of less than 1mm in inferior or lateral precordial leads during hyperventilation is a nonspecific finding. Previous workers have also observed that hyperventilation can produce ST-segment changed in subjects with or without coronary artery disease [2, 5, 10, 25, 27, 28]. Exact pathogenesis of these changes is not clear. Hyperventilation reduces coronary flow [25, 29, 30]. Low concentration of carbon dioxide [31] and vagal stimulation [24] could contribute to this effect. The exact significance of ST-segment depression seen during hyperventilation is not clear. These changes can be seen in subjects with or without significant obstruction on coronary angiography [10, 13, 27]. Some authorities, therefore, feel that hyperventilation does not help in identifying false responders [10]. It does not increase test accuracy [4] and is, therefore, not recommended [13]. However, hyperventilation does reduce coronary flow [25, 30]. In patients with decreased coronary reserve or those with coronary microvascular disease, hyperventilation could reduce coronary flow relative to myocardial oxygen demand [29], even in absence of significant obstructive lesion on coronary angiography. This could produce myocardial ischemia in either watershed zones or downstream from otherwise insignificant lesions [6]. A period of hyperventilation prior to stress test can identify such patients [6]. Long term follow up of such persons is needed to find the correct significance of such ST-segment changes. Two patients had ST-segment depression in inferior and lateral precordial leads with ST- segment elevation in lead aVR. Both cases had a positive stress test. ST-segment elevation in lead aVR during exercise in combination with ST-segment depression in other leads suggests left main or severe LAD disease [10, 13, 19, 26]. Our observation suggests that any ST-segment elevation in lead aVR during hyperventilation is also significant. There is no literature about the effect of hyperventilation on lead aVR. Changes in T Waves: Hyperventilation produced new T wave inversion in inferior and/or lateral precordial leads in six cases. Two of them had significant ST-segment depression during exercise. T wave inversion during hyperventilation has also been observed by previous workers [2, 13, 24]. These could be related to reduce carbon dioxide concentration or to reduce coronary flow as discussed above. Wasserburger, et al. [24] evaluated the effect of breathing various concentrations of carbon dioxide and oxygen, vagal blockade with propantheline and potassium ion in abolishing hyperventilation induced T wave inversion in normal adults without any clinical evidence of coronary artery disease or significant cardiovascular disease. They observed that hyperventilation induced T wave inversions were blocked by propantheline. They concluded that these T wave inversions were produced by vagal reflex arising in the thorax. Shallow T wave inversion may or may not correlate with the presence of significant ST-segment depression during exercise. However, T waves that are deep, symmetrical, sharply pointed and arrowhead in appearance should not be ignored. One of our patients developed shallow inversion of T wave in lead V1. There was no ST-segment depression on exercise. An increase in T wave inversion in lead V1 is not significant. Any peaking of T wave in lead V1 and V2 should be considered abnormal.
Conclusions
Changes on Standing from the Supine Position
There is a variable increase in heart rate. An increase of more than 30 beats/minute, in absence of a fall of more than 20 mm Hg in systolic blood pressure, is abnormal. It is usually due to autonomic dysfunction but may be associated with significant ST-segment depression during exercise. There is no significant change in the P wave, P-R segment, P-R interval and mean frontal plane QRS axis. R wave amplitude may decrease in inferior and/or lateral precordial leads. It does not have any clinical significance. An increase in R wave amplitude in leads I, aVL, V3 to V6 is unusual and may be associated with significant ST-segment depression during exercise. Some persons can develop less than 1mm ST- segment depression. The significance of such change should be decided only in the context of the pretest probability of coronary artery disease. Some persons can develop shallow T wave inversion in inferior and/or lateral precordial leads. These changes are usually non-specific. Change of negative T wave to positive T wave in leads V1 and V2 is associated with significant ST-segment depression during exercise.
New Changes Appearing During Hyperventilation after Standing
The magnitude of changes varies depending on the rate, depth and duration of hyperventilation. There is a variable increase in heart rate. It does not have any clinical significance. Rarely heart rate may decrease. It is probably due to vagal stimulation and may be associated with significant ST-segment depression during exercise. There is no significant change in the P wave, P-R segment and P-R interval. R wave amplitude is usually reduced in inferior and/or lateral precordial leads. Uncommonly there is some increase in R wave amplitude. Their findings do not correlate with ischemic changes during exercise. A small number of patients develop ST-segment depression of less than 1mm in inferior and/or lateral precordial leads. These are not significant. ST-segment elevation in lead aVR is associated with ischemic changes during exercise. Some patients develop shallow T wave inversion in inferior and or lateral precordial leads. These are not associated with ischemic changes during exercise.
References
-
Markendorf S, Lucher TF, Gerds-Li JH, Schonrath F, Schmid CM (2018) Clinical impact of repolarization changes in supine versus upright body position. Cardiol J 25(5): 589-594.
-
Kern B (2021) Hyperventilation syndrome. Med scope.
-
Khare S, Chawla S (2016) Effect of change in body position on resting electrocardiogram in young healthy adults. Nig J Cardiol 13(2): 125-129.
-
Detrano R, Giatrossi R, Froelicher V (1989) The diagnostic accuracy of the exercise electrocardiogram: a meta-analysis of 22 years of research. Prog Cardiovasc Dis 32(3): 173-206.
-
Gibbans RJ, Balady GJ, Bricker JT, Chaitman BR, Fletcher GF, et. al. (2002) ACC/AHA 2002 guideline update for exercise testing: a report of the American College of Cardiology/American Heart Asociation Task Force on Practice Guidelines (Committee on Exercise Testing). J Am Coll Cardiol 40(8): 1531-1540.
-
Rowan CJ (2018) Metabolic abnormalities and drugs. _In_: Thomas GS, et al. (Eds.), Ellestad’s Stress Testing. Oxford, UK, pp: 446-469.
-
Mason RE, Likar I (1966) A new system of multiple lead exercise electrocardiography. Am Heart J 71(2): 196- 205.
-
Bruce R, Blackman J, Jones J, Strait G (1963) Exercise testing in adult normal subjects and cardiac patients. Pediatrics 32: 742-756.
-
Jain M, Nikonde C, Lin BA, Walker A, Wacker FJ (2011) 85% of maximal age-predicted heart rate is not a valid end point for exercise treadmill testing. J Nucl Cardiol 18(6): 1026-1035.
-
Thomas GS, Ellested MH (2017) Electrocardiographic Exercise Testing. _In:_ Fuster V, et al. (Eds.), Hurst’s The Heart. Mc Graw Hill, New York, pp: 318-334.
-
De Luna AB, Goldwasser D, Fiol M, Genis BA (2017) Surface electrocardiography. _In:_ Fuster V, et al. (Eds.), Hurst’s The Heart. Mc Graw Hill, New York, pp: 252-317.
-
Mirvis DM, Goldberger AL (2019) Electrocardiography. _In:_ Zipes DP, et al. (Eds.), Braunwald’s Heart disease. Elsevier, Philadelphia, pp: 117-151.
-
Thomas GS, Samtani SR, Ellestad MH (2018) Interpretation of the ECG during exercise and recovery. _In:_ Thomas GS, et al. (Eds.), Ellestad’s Stress Testing. Oxford, UK, pp: 160-198.
-
Huang MH, Epey J, Wolf S (1991) Heart rate- QT interval relationship during postural change and exercise. A possible connection to cardiac contractility. Integi Physiol Behav Sci 26(1): 5-17.
-
Grubb BP (2017) Diagnosis and management of syncope. _In:_ Furter V, et al. (Eds.), Hurst’s The Heart. Mc Graw Hill, New York, pp: 2098-2112.
-
Tomaselli GF, Zipes DP (2019) Approach to the patient with cardiac arrhythmias. In_:_ Zipes DP, et al. (Eds.), Braunwald’s Heart Disease. Elsevier, Philadelphia, pp: 597-603.
-
Freeman R, Wieling W, Axelrod FB, Benditt DG, Benarroch E, et al. (2011) Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndromes. Clin Auton Res 21(2): 69-72.
-
Madias JE (2006) Comparability of the standing and supine standard electrocardiogram and standing, sitting and supine stress electrocardiogram. J Electrocardiol 39(2): 142-149.
-
Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, et al. (2013) Exercise standard for testing and training: a scientific statement from the American Heart Association. Circulation 128(8): 873-943.
-
Schamroth L (1982) Basic principles. _In:_ Schamroth C, et al. (Eds.), An introduction to Electrocardiography. Blackwell Science, France 5: 33.
-
Whinnery JE, Froelicher VF, Lango MR, Triebwasser JH (1977) The electrocardiographic response to maximal treadmill exercise in asymptomatic men with right bundle branch block. Chest 71(3): 335-340.
-
Engel GL, Ferris EB, Logan M (1947) Hyperventilation: Analysis of clinical symptomatology. Annals of Internal Medicine 27(5): 683-704.
-
Lewis BI (1953) The hyperventilation syndrome. Annals of Internal Medicine 43: 918-927.
-
Wasserburger RH, Siebecker KL, Lewis WC. Lloyd CJ (1956) The effect of hyperventilation on the normal adult electrocardiogram. Circulation 13(6): 850-855.
-
Ardissino D, De Servi S, Barberis P, Demicheli G, Falcone C, et al. (1989) Significance of hyperventilation induced ST segment depression in patients with coronary artery disease. J Am Coll Cardiol 13(4): 804-810.
-
Balady GJ, Morise AP (2019) Exercise electrocardiographic testing. In: Zipes DP, et al. (Eds.), Braunwald’s Heart Disease. Elsevier, Philadelphia, pp: 154-173.
-
Lary D, Goldschlager N (1974) Electrocardiographic changes during hyperventilation resembling myocardial ischemia in patients with normal coronary angiograms. Am Heart J 87: 383-390.
-
Gallagher LA (1995) Effect of submaximal exercise and hyperventilation on ECG components in healthy young adult men with recording leads typically used for evaluation of ischemic heart disease. A thesis submitted for the degree of Master of Science in Education to Virginia Polytechnic Institute and State University 1995.
-
Pribble A, Kusumi F, Bruce RA (1987) Dyskinemia associated with hyperventilation. Journal of Cardiopulmonary Rehabilitation 7: 570-577.
-
Rowe GG, Castillo CA, Crumpton CS (1962) Effects of hyperventilation on systemic and coronary hemodynamics. Am Heart J 63: 67-77.
-
Case RB, Felix A, Wachter M, Kyriakidis G, Castellona F (1978) Relative effect of CO2 on canine coronary vascular resistance. Circ Res 42(3): 410-418.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study