Cardiac Surgery and Covid-19 Insight into Peri-Operative Management
Background: Health care is seriously affected by the corona virus disease 2019 (COVID-19) pandemic with alarming effects upon conduct of cardiac surgery. The initial resource conservation strategy has to modify for handling the surging case load due to deference of routine care in the face of pandemic. Methods: The cardiac surgical practice during the lockdown period (from 25th March till 30TH November 2020) at a tertiary care centre was observed. The cardiac diagnosis of the ones operated, conduct algorithm, and working policy were analyzed. Descriptive statistics was applied to calculate the percentages of different case subsets in both adult and pediatrics groups. Results: Total of 333 emergency cases were operated on during the time frame from 25thMarch 2020 to 30thNovember 2020. Cases were divided into adult and pediatric cases. Total adult cases were 160 (48%) in number. Adult cases were further classified into aortic cases, coronary artery disease, valvular pathologies and miscellaneous ones. Total 11 aortic cases (6.8%), 43 CABG cases (26.8%), 42 valvular cases (26.2%) and 83 miscellaneous cases (51.8%) were operated. In the pediatric population, a total of 173 cases (52%) were operated, with 42 cases (24.2%) being arterial switch operations, one case of ALCAPA repair (0.5%), 25 cases (14.4%) of TAPVC repair and others (60.6%). All cases were preoperatively COVID-19 negative. However postoperatively 10 patients (3%) showed symptoms of COVID-19 and on testing turned out to be COVID-19 positive. 8 patients (80%) were transferred to dedicated COVID-19 facility for management and later 6 (60%) were discharged after successful management. There was no COVID-19-related mortality and none of the health-care workers developed COVID-19 in the entire study period. Conclusion: The initial phase of resource conservation has undermined the routine cardiac surgical practice. The study showed that strict adherence to management algorithm is necessary for persisting smooth continuation of cardiac surgical practice with provision of optimum critical care. The strategic comeback against COVID-19 would urge institutional development of protocols to aid the post-surge period.
Introduction
COVID-19 has established itself as a global pandemic affecting global economy and healthcare practices worldwide. The pandemic has affected more than 190 countries around the world. The COVID-19 pandemic in India is a part of the worldwide pandemic of corona virus disease 2019 (COVID-19) caused by severe acute respiratory syndrome corona virus 2 (SARS-CoV-2). The first case of COVID-19 in India was reported on 30th January 2020. In a few months, it rampantly escalated paralyzing the health care services globally. Nationwide lockdown was introduced to manage this pandemic in India in various phases. On 24th March 2020, the Government of India under Prime Minister Narendra Modi ordered a nationwide lockdown for 21 days, limiting movement of the entire 1.3 billion population of India as a preventive measure against the COVID-19 pandemic in India [1].
The emphasis on conservation of critical care resources with suspension of elective surgical procedures was enforced in liaison with this mitigation strategy to prepare for the upcoming surge. Cardiac surgical practices are not in the frontline providing care to COVID-19 patients; however, COVID-19 has caused a deep impact on cardiac surgical practices by limitation of staff, intensive care unit beds, ventilation sites and other necessary resources required for an effective conduct. Our center is a high volume center for cardiac surgery, catering to the needs of the entire country and performing approximately 3000 to 4000 cases per year.
The impact of COVID-19 on cardiac surgery at our center has been profound too. We have conducted a survey analyzing the various procedures done at our center amidst this COVID-19 outbreak [2]. Amidst the pandemic, safeguarding of critical resources has been regarded as the prime matter for concern. However, though delaying elective surgeries is feasible, certain groups of cardiac patients require emergent intervention in order to decrease morbidity as well as mortality, and catering to such a population is unavoidable to an extent unethical. Cardiovascular diseases are the leading cause of mortality in the world. Though cardiovascular diseases can be avoided for a period of time they cannot be completely ignored as the burden of disease on the society is massive and complete withdrawal of services is not an adequate answer. Therefore, this study was conducted to see the cases being catered to at a tertiary care cardiac surgical center amidst this massive medical crisis with attention being paid to the challenges faced which may guide in strategizing an effective comeback.
Methodology
A cross sectional study was performed taking the period of lockdown from 25thMarch 2020 to 30thNovember 2020 as time frame. All surgical cases performed at a tertiary care center in the above stated period were noted and analyzed [3]. The admission policy, comprehensive cardiac diagnosis, ICU preparedness and mitigation strategy was described showing the change in conduct of cardiac surgical practice during the ongoing COVID-19 pandemic time.
Statistical Analysis
All the data was entered in Microsoft Excel and analyzed in STATA 12.0. The statistical analysis was descriptive. Cases were stratified into adult and pediatric cases and were further sub categorized. Percentages of different cases were derived [4].
Results
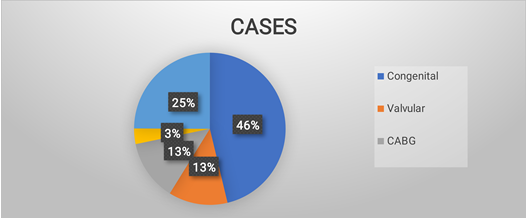
Total of 333 emergency cases were operated on during the time frame from 25thMarch 2020 to 30thNovember 2020. Cases were divided into adult and pediatric cases (Figures 1 & 2).
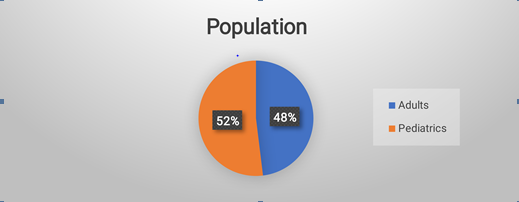
Total adult cases were 160 (48%) in number. Adult cases were further classified into aortic cases, coronary artery disease, valvular pathologies and miscellaneous ones (Table 1).
| Total | Male | Female | Adults | Pediatrics | Congenital | Valvular | CABG | Aortic | Miscellaneous |
|---|---|---|---|---|---|---|---|---|---|
| 333 | 229 (68.7%) | 104 (31.2%) | 160 (48%) | 173 52%) | 154 (46%) | 42 (26.2%) | 43 (26.8%) | 11 (6.8%) | 83 (51.8%) |
Table 1: Total 11 aortic cases (6.8%), 43 CABG cases (26.8%), 42 valvular cases (26.2%) and 83 miscellaneous cases (51.8%) were o
All cases were preoperatively COVID-19 negative. However postoperatively 10 patients (3%) showed symptoms of COVID-19 and on testing turned out to be COVID-19 positive. 8 patients (80%) were transferred to dedicated COVID-19 facility for management and later 6 (60%) were discharged after successful management.
Discussion
The phasic transition in lockdown has been accompanied with phasic shift in hospital strategy for re-allocation of limited critical care resources for those in dire need. The number of operated cases has witnessed a significant decline since the beginning of the lockdown which was imposed from 24th March, 2020. In the initial phase, emphasis was on the preservation of critical care resources, so all the cases were deferred; however, emergency case were continued with adequate precaution [5, 6]. With the overwhelming pandemic still surging, waiting further may have led to increased mortality, hence, appropriate strategy was required to resume cardiac surgical practice. Multidisciplinary team efforts in conjugating a management plan with a list of the cases prioritizing the emergent ones and deferring those which can be delayed without significantly increasing the morbidity or mortality was required.
The formation of a pre-operative screening area for the RT-PCR testing of the patients being admitted with lowest threshold for repeat testing in case of strong clinical suspicion was done. The cases were transferred to cardiac surgical pre-operative wards after confirmed negative report wherein social distancing norms with respect to distance between successive beds was maintained and in separate isolation areas where clinical suspicion prevailed in spite of negative report. An infectious disease surveillance team was formed in the department for intra-departmental screening in both pre and post-operative patients. The tests were done as close as possible to the time of the patients’ scheduled surgeries [7].
The routine elective ORs were closed and only 2 of 8 were functional during this time of crisis for maintenance of work force and critical care resources. Donning and doffing areas were established in OR complex for personal protective equipments. The addition of double filters in anesthesia ventilators with the use of face shield during intubation was practiced thoroughly in intubation drills carried out by the department.
Cardiac Surgery Amidst Pandemic
COVID-19 has created havoc in the world and continues to be a threat to health as well as all the heath care facilities around the world and has invariably diverted much of our resources to its management. Due to existence of such grave conditions, there was requirement to establish a meticulously drafted multidisciplinary plan for resumption of cardiac surgery amidst this chaos [8].
How we planned our surgical activity during COVID-19 period? Lockdown lead to suspension of all elective surgeries and routine outpatient services at our institute in order to prepare ourselves for the upcoming pandemic and curb its spread and adverse effects. Following conditions which came under the emergency criteria were accommodated but with a newly formulated protocol:
Adults
- Type A aortic dissection.
- Coronary artery disease (CAD) spectrum-Severe unstable angina/severe left main disease angioplasty complications, acute coronary syndrome with mechanical complications.
- Stuck prosthetic valves, thrombolysis unresponsive, class IV.
Pediatrics
- Obstructed total anomalous pulmonary venous return, refractory spells, cardiac tamponade patients.
- Some other congenital heart problems, which if delayed, may deteriorate beyond a point to cause lifelong morbidity (Transposition of great arteries (TGA) with regressing ventricle).
Pre-operative consideration
- Emergency department- Every patient in requirement of an emergency surgery was tested for SARS COV-2 via RT-PCR test (30-50% false negative) in the emergency department and kept in emergency ward until the results of test came back [9, 10]. Along with that, they were screened for temperature, and history of contacts with COVID-19 patients and travel from hotspot areas, if any, was documented.
- If the patient turned out positive then he/she was treated for COVID-19 in the COVID dedicated hospital sections.
- If the patient tested negative, patient was shifted to COVID dedicated step down ward if the patient was stable and if the patient required more critical care, then to the ICU setting.
- If patient required critical care and the test results were still awaited, then the patient was shifted to dedicated CTVS COVID-19 ICU, equipped with ventilatory support, round the clock doctors and nursing staff with level-3 personal protective gear. If the patient tested negative, patient was shifted to CTVS NON-COVID ICU. If the patient tested positive, then patient was shifted to dedicated COVID section of our center.
- Two cubicles in step down ward had been allocated to admit all new patients. A single nursing staff with proper PPE was allocated in each cubicle. Senior resident on duty had to wear appropriate PPE (N95 mask, face shield and gloves) before interacting with the isolated patients. COVID-19 swabs were taken on Day 0 and Day 5 by the emergency ID team.
- Blood sampling was done with adequate precautions. The blood bank was informed beforehand about sending of these samples.
- If positive, surgery was postponed as per hospital/ department policy for 2-4 weeks (not be done on these patients) unless it was an emergency.
- If patient was declared COVID-negative/cleared for surgery by ID team, they were taken up for surgery.
- Consent was taken regarding any surgical procedure, unexpected delays, minimal visitor entry, teleconferencing as a mode of communication about patient status while in ICU and wards during treatment and also for follow ups post discharge.
- Thorough psychological counseling was done (Figure 3).
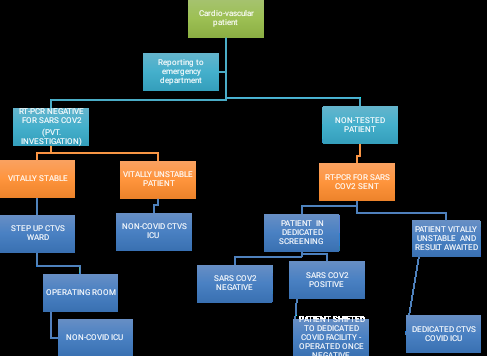
Figure3: Patient Triage Algorithm.
Intra-Operative Considerations
- Precautions outlined during peri-operative period include anesthesia induction to be done with minimum staff wearing full PPE gear.
- Operating team was limited in number to decrease resource utilization and exposure risk.
- Proper personal protective gear as per institution protocol was used.
- It was kept in mind that sternotomy and airway manipulation will generate aerosol.
- There were designated PPE donning and doffing areas for all personnel.
- The staff disposing off the discarded PPE was made fully conversant with the correct procedure and trained to perform the task without error.
- Due to COVID-19, limited number of operation rooms were functional, being reduced from normally 8 rooms to 2 rooms.
- After a week of utilization of the two operating rooms, the operating rooms were disinfected and other available operating rooms were used in a similar fashion.
- Post-surgery patients were shifted to non-Covid CTVS ICU for post-operative management.
- Currently COVID-19 positive patients are not being operated in our institution and once the patient is declared negative, the patient is taken up for surgery after patient is stabilized and optimized for surgery.
ICU Modifications in COVID-19 Times
- Avoid transferring confirmed cases to the non-Covid ICU.
- Transfer confirmed cases to dedicated COVID ICU with pressure and oxygen supply, emergency intubation cart.
- Disinfect high touch surfaces like anesthesia machine and anesthesia work area with an Environmental Protection Agency (EPA)-approved hospital disinfectant.
- Allow time for aerosols in isolation to be washed out [11].
- Surgical mask provided to awake and stable patients.
- Distance of 1 meter between patient beds.
- Daily assessment of temperature and respiratory symptoms.
- New onset fever or cough to be isolated and investigated.
- Avoid high flow oxygen, NIV, or nebulized medications.
- Postoperative rounds, medications and wound management to be performed under full PPE.
- No entry of attendants of the patient in the ICU in order to avoid any transfer of COVID-19 infection to susceptible patient and health care workers.
- Amidst pandemic there is a surge of sicker variety of patients, who require meticulous care and have a much difficult post-operative course and require a longer ICU stay.
Post-Operative Considerations
Immediate Post-Operative Period
- Patient receiving checklist cleared.
- Patient allowed entering the ICU.
- One person at head end and two other persons by the side of bed while shifting.
- One person for attaching monitors and any drugs, if required.
- Patient connected to ventilator.
- Optimization of inotropes and medications as per patient requirement.
- While attending a patient or performing a procedure level 2 PPE mandatory.
- Emphasis on fast tracking of the post-operative period via early extubation, early mobilization and early shifting of the patient to dedicated non-Covid ward wherever possible.
- Low threshold kept for COVID-19 testing in patients showing features of COVID-19 and repeated testing done in view of moderate sensitivity of test (50-70%) [12].
- All healthcare personnel vigilant about any symptoms of COVID infection and if symptomatic, the clinical algorithm followed fully by them (reporting to emergency COVID screening area, getting appropriate advice and triage as per symptom severity and report positivity).
- If a patient’s test result for COVID-19 comes as positive, patient immediately transferred to COVID dedicated CTVS ICU.
- Contact tracing done by the nodal officer; contacts stratified into high risk or low risk contacts based upon the type, time of exposure and the level of PPE kit donned by the exposed personnel.
- Once patient is stabilized then patient is shifted to non- Covid CTVS ward from where patient is discharged.
Modified Approach for Post-Operative Outpatient Follow Up
- Technology now allows people to connect anytime, anywhere, to anyone in the world, from almost any device.
- This has dramatically changed the face of medical practice and has come in as one of the forerunners in providing necessary facilities to patients, reducing resource consumption.
- It has provided a safe and easy method for the most important component in medical practice that is “communication” while eliminating the risk of transfer of infection.
- Patients are attached to telemedicine OPD as regular OPD services are suspended.
- Patients are provided with tele-OPD numbers and can call during fixed days and time periods.
- Patients interaction also done with the use of digital communication using video conferencing, image exchanges on messengers (inspection of post-operative wound etc.), soft copy exchange of reports and advised to visit emergency department if required.
- Late post-operative period. Patients discharged are advised the following: a) Fluid restriction if required. b) Follow diet restriction. c) Report immediately if: Fever more than 2 days
- Bleeding/ discharge from wound.
- Decreased urine output.
- Worsening of symptoms.
- Shortness of breath.
- Giddiness, intense headache. a) In case of emergency, contact the nearest hospital or emergency department of our institute. b) Daily bath and maintenance of personal hygiene. c) For patients with mechanical heart valves and on anticoagulation, always follow strictly:
- The correct dose of warfarin (blood thinner) to be taken as prescribed to prevent clot formation and dysfunction of valve.
- PT- INR range to be maintained as per the valve placed.
- Dose to be remembered by patient as well as patient bystander every time.
- Warfarin to be taken astutely at a fixed time every day.
- PT-INR blood testing to be fortnightly or as advised. Patients are explained in detail about symptoms of COVID -19 and taught as to how to approach the hospital in case of suspected COVID infection.
Conclusion
The secret of change is to focus all of your energy, not on fighting the old, but on building the new.” -Socrates. “Losing your head in a crisis is a good way to become a crisis.” - C.J Redwine COVID-19 has challenged the medical field in every way possible, from absence of a cure to exposing malfunctioning health care infrastructures. It has diverted our attention from other important diseases like cardiovascular diseases in which the management and outcome is ever changing, depending upon the time of intervention. Safe cardiac surgery in view of the ongoing pandemic is possible, with consideration of optimal utilization of resources.
References
-
Times F (2020) Coronavirus tracked: the latest figures as the pandemic spreads. Financ Times.
-
Coronavirus in India (2020) How the Covid-19 pandemic affects India. Pharmaceutical Technology.
-
User S (2020) Cardio-Thoracic & Vascular Surgery. AIIMS New.
-
(2020) The top 10 causes of death.
-
(2020) Coronavirus in India: Modi Orders Total Lockdown of 21 Days. The New York Times.
-
(2020) Covid-19 in Delhi: AIIMS, RML and Lady Hardinge to suspend non-essential surgeries. Delhi News, Times of India.
-
Xiao AT, Tong YX, Zhang S (2020) False‐negative of RT‐ PCR and prolonged nucleic acid conversion in COVID‐19: rather than recurrence. J Med Virol 92(10): 1755-1756.
-
West CP, Montori VM, Sampathkumar P (2020) COVID-19 testing: the threat of false-negative results. In: Mayo Clin Proc 95(6): 1127-1129.
-
Winichakoon P, Chaiwarith R, Liwsrisakun C, Salee P, Goonna A, et al. (2020) Negative nasopharyngeal and oropharyngeal swabs do not rule out COVID-19. J Clin Microbiol 58(5): e00297-e00320.
-
(2020) Aide memoire for Levels of Personal Protective Equipment (PPE) for Healthcare Workers when providing patient care.
-
Hote M, Gupta SS (2020) Cardiothoracic surgery practice at a tertiary center during the COVID-19 pandemic.
-
(2020) Postoperative Care in Covid-19 Patients. AIIMS Covid Information Portal.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study