Assessment of Cardiac Function during First Pregnancy Using Speckle Tracking Echocardiography
Background: Pregnancy is a dynamic process associated with significant and thorough hormonal and hemodynamic changes that directly or indirectly influence cardiac function. However, the effect of these alterations on left ventricular myocardial contractile function has not been fully illustrated. Objective: To assess the maternal cardiac function during the third trimester of first pregnancy using Speckle Tracking echocardiography. Results: This cross sectional study was carried out in Baghdad teaching hospital in the time period from November 2020 to June 2021. A total of 100 women were studied, they were classified into two groups: 50 non pregnant women with mean age (24.6 ±4.60 years) served as control group, and 50 pregnant women with normal singleton pregnancy (30-40 weeks of gestation) with mean age (23.6±3.63 year) served as study group. The left ventricular systolic function was assessed using transthoracic echocardiography to measure LV ejection fraction EF%. Furthermore, the left ventricular contractile function evaluated with speckle tracking echocardiography (STE) by measuring LV global longitudinal strain (GLS). The left ventricular ejection fraction shows no significant difference between pregnant and control group (p= 0.214), while the left ventricular global longitudinal strain (GLS) shows significant decrease in the pregnant females in their third trimester (p=0.001). Conclusion: left ventricular global longitudinal strain (GLS) shows significant reduction during the third trimester of normal first pregnancy.
Introduction
Pregnancy is a dynamic process associated with significant and thorough hormonal and hemodynamic changes that directly or indirectly influence cardiac function. The increased metabolic demands of the mother and fetus are the cause behind these changes. Maternal inability to adapt to these physiological changes can expose underlying, previously silent, cardiac disease; furthermore de novo cardiac dysfunction may also be induced. Actually, cardiac diseases complicate 1–4% of pregnancies in women without previously diagnosed cardiovascular abnormalities [1, 2]. The maternal hemodynamic physiological adaptations involving increase in circulating blood volume, increasing in stroke volume, cardiac output and heart rate with a concomitant decrease in systemic vascular resistance and blood pressure [3].
The most important technique used in the evaluation of pregnant women heart is echocardiography. Furthermore, the assessment of left ventricular systolic function could be done using the traditional echocardiographic measures such as LV ejection fraction or using speckle tracking echocardiography, which is new technique measure the regional rate, strain and strain rate from 2D grayscale visualizations [4]. However, the effect of these alterations on left ventricular (LV) myocardial contractile function has not been fully illustrated and different studies reporting LV systolic function as being normal, enhanced or depressed during pregnancy [5, 6].
The application of speckle-tracking echocardiography (STE) gives us more comprehensive assessment of LV myocardial contractility and has allowed better mechanistic insights into cardiac alterations in many disease states [7].
Ejection fraction gives us an impression about the function of myocardium as a whole. Further studying of the cardiac mechanics shown that it is a multi-layered phenomenon, and left ventricular wall is composed of three layers of fibers. Deterioration in the function of one layer is compensated by others so the numerical value of ejection fraction is not compromised in the beginning [8]. And this necessitate the need for another parameter more sensitive than EF, this parameter is the myocardial strain which defined as the ratio of change in length (DL) to resting length (Lo) after application of force to a muscle, it expressed as percentage and symbolized by Epsilon as shown in the formula bellow:
$$ \varepsilon = \frac {\Gamma^ {0}}{\Gamma - \Gamma^ {0}} = \frac {\Gamma^ {0}}{\nabla \Gamma}, $$ Where, Î = strain, L0 = baseline length and L = instantaneous lengths at the time of measurement. The term “strain” in echocardiography it used to describe “deformation” in cardiac muscle while, in language it means “stretching”. While, the strain rate (SR) it is defined as the rate by which the deformation occurs (deformation or strain per time unit) [9].
Aims of Study
To assess the maternal cardiac function during pregnancy using Speckle Tracking echocardiography.
Subjects and Methods
This cross-sectional study was carried out in Baghdad teaching hospital. A total of 100 women were studied, they were classified into two groups: 50 non pregnant women with mean age (24.6 ± 4.60 year) served as control group, and 50 pregnant women with normal singleton pregnancy (30-40 weeks of gestation) with mean age (23.6± 3.63 year) served as study group.
Inclusion criteria
- First Singleton uncomplicated pregnancy (Primi).
- Age 20-35-year-old.
- During the third trimester (30-40 week).
- BP < 140/90 mmHg measured in the left lateral decubitus position.
- Normal fetal parameters and amniotic fluid index (confirmed by ultrasound in the same hospital). While,
Exclusion criteria
- All complications of pregnancy (congenital fetal abnormalities, placenta previa, accreta etc).
- Essential hypertension.
- Ischemic heart diseases.
- Diabetes mellitus DM.
- Valvular heart disease.
- Anemia.
- Dyslipidemia.
- Thyroid dysfunction.
- Smoking.
All participants were submitted to a detailed medical history and physical examination, their blood pressure was measured in the left lateral decubitus position and their body weight and height were measured to calculate body mass index and body surface area.
Echocardiographic examination was performed for all women using (Vivid E9; GE Healthcare, Horten, Norway) equipped with 2.5 MHz S5-1 transducer. ECG leads were placed over the chest and women were examined in the left lateral decubitus position, to bring the heart forward to the chest wall and lateral to the sternum, with dimmed light room as recommended by the American society of echocardiography [10]. The LV ejection fraction was measured using 2D guided M mode echocardiography by placing the transducer in the 3rd intercostal space with the indicator pointing to the right shoulder to obtain parasternal long axis view. In addition, the left ventricular contractile function assed using speckle tracking echocardiography by measuring LV global longitudinal strain (GLS). Three standard apical 5C, 4C, and 2C views were acquired and for each view, 3 consecutive cardiac cycles were acquired. Gray- scale images were obtained at a frame rate of 60–70 frames/ s using harmonic (1/3 MHz) B-mode imaging. The peak systolic longitudinal strain for each segment is displayed based on a 17-segment model for each plane, and the results of all 3 planes were combined in a single bull’s eye summary. Normal range of GLS = (-15.9%) _ (- 22.1%) [11]. Informed consent was obtained from all individual participants included in the study.
Statistical analysis
In this cross-sectional study, statistical analysis was performed using the statistical package SPSS for windows (version 23, SPSS Inc., Chicago, IL, USA). Data were shown as mean ± SD. Continuous variables were compared using independent sample t tests. Relationship between two parameters was analyzed using Pearson correlation coefficient. A P value < 0.05 was adopted to indicate statistical significance [12].
Results
This study included 100 women, 50 of them represent no significant difference with (p= 0.214) study group and the rest are control group, as shown in (Table 1).
| Age (years) | Weight (Kg) | Height (meters) | BMI (Kg/m²) | BSA (m²) | |
|---|---|---|---|---|---|
| Control group | 24.6 ±4.6 | 65.1±5.61 | 160.56±3.93 | 25.2±3.08 | 1.7±0.25 |
| Study group | 23.6±3.63 | 80.8±11.38 | 161.93±5.64 | 30.7±3.49 | 1.9±0.25 |
| P-value | 0.22 (NS) | 0.001 | 0.37(NS) | 0.001 | 0.001 |
Table 1: Demographic characteristic of women involved in study.
The results show significant increase in the heart rate of pregnant females with (p value of 0.001), while the systolic blood pressure (SBP) and the diastolic blood pressure (DBP) decreased in pregnant females in comparison to the control non-pregnant females with (p value 0.001 and 0.011), respectively as shown in (Table 2).
| Heart rate Beat\min | SBP (mmHg) | DBP (mmHg) | |
|---|---|---|---|
| Control group | 75.9 ± 6.23 | 120.3 ± 8.09 | 70.0 ± 8.91 |
| Study group | 95.9 ± 10.24 | 106.8 ± 16.59 | 64.1 ± 6.08 |
| P-value | 0.001 | 0.001 | 0.011 |
Table 3: Comparison of Heart rate & Blood pressure findings.
On other hand, the global longitudinal strain (GLS) shows significant decrease in the pregnant females in their third trimester in comparison to control non pregnant women (p= 0.001) as shown in (Table 3).
| EF % | GLS % | |
|---|---|---|
| Control group | 65.83 ± 4.58 | -19.03 ± 0.80 |
| Study group | 64.70 ± 4.40 | -17.63±1.87 |
| P-value | 0.214 (NS) | 0.001* |
Table 4: Assessment of LV systolic function cases and controls.
Studying the correlation between LV ejection fraction and global longitudinal strain shows no significant relation with P-value of 0.19 and Correlation coefficient (r) equal to 0.24 as shown in (Figure 1).
| variable | Correlation coefficient (r) | P - value |
| value | 0.24 (NS) | 0.19 (NS) |
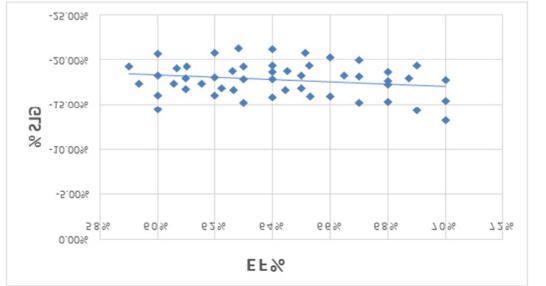
*NS = not significant Figure 1: Correlation between LV ejection fraction and global longitudinal strain.
Discussion
Major cardiovascular adaptive mechanisms take place during pregnancy, the most remarkable changes include: increased cardiac output and blood volume expansion associated with a decline in the systemic vascular resistance and blood pressure leading to left ventricular remodelling [13]. In the current study, we find significant increase in the body weight of pregnant women along with BMI & BSA, the increased weight gain during pregnancy is considered among the risk factors for maternal and fetal complications, including the risk of future cardiovascular diseases [14]. Similar results were found by [15, 16]. Regarding cardiovascular changes in the healthy pregnancy in comparison with control non-pregnant women the heart rate shows significant rise in pregnant women within physiological range this comes in agreement with previous studies of [17, 18], whereas the systolic & diastolic blood pressure decreases also within physiological range which mention that despite the sympathetic hyperactivity and increased plasma volume, most normal pregnancies are associated with normal or decreased blood pressure. Regarding the LV systolic function, numerous studies have been evaluated it during pregnancy, but they have reported conflicting results [19, 20]. Here in our study we used speckle tracing echocardiography (STE) and more specifically tracking of speckles in the longitudinal direction because the longitudinal strain is determined by the vertically arranged subendocardial fibers that are more susceptible to alterations in loading conditions such as pregnancy and to myocardial pathologies [21]. mention in this study that Global longitudinal strain (GLS) is the first one to get impaired in most of disease states, while the Global circumferential strain (GCS) and Global Radial Strain (GRS), which are determined mainly by the radially arranged mid-myocardial and subepicardial fibers both are relatively late to get involved, with radial strain being the last one to be affected furthermore GRS may even be paradoxically increased during the early course of disease aiming to compensate for the loss of long-axis function [21]. In this study the left ventricular ejection fraction not significantly changed when compare the control group with pregnant women, whereas the global longitudinal strain (GLS) exhibit significant decrease in pregnant women, this is similar to the previous studies of [22, 23, 24]. The reduction of GLS during pregnancy explained by Sengupta and his colleagues to be the result of changed loading condition and geometric changes in the left ventricular shape such as increasing sphericity [23], in his study measure all three STE parameters : GLS, GCS and GRS, and he find that GRS increased during pregnancy so he suggest that this augmentation in the GRS is an adaptation method supposing the myocardium is inherently normal and the impairment of contractile function in one direction is associated with counterbalancing changes in the other directions that helps maintain normal LV ejection performance and meet the increased circulatory needs of pregnancy [23]. Studying the correlation between GLS (as an early predictor of myocardial remodelling) with left ventricular ejection fraction (LVEF) shows no correlation between LVEF and the left ventricular global longitudinal strain GLS, this goes in agreement with [23, 24], who mention in their studies on pregnant women in their third trimester that despite normal LVFF there is reduction in the LVGLS.
Conclusion
Left ventricular global longitudinal strain (GLS) shows significant reduction during the third trimester of normal pregnancy, while the LV EF still within normal ranges.
The authors declared no conflict of interest.
References
-
Camm AJ, Lüscher TF, Serruys PW (2009) The Esc Textbook of Cardiovascular Medicine. Oxford University Press.
-
AL Kareem ZHA, Hamzah MI, Kader HAA (2021) Evaluation of Pregnancy Associated Plasma Protein A (pappa) Antioxidant Tocopherol and Kinetic Study of Paraoxonase 1 (pon 1) in Preeclamptic pregnant women. Biochem Cell Arch 21(1): 1011-1019.
-
Meah V, Cockcroft Jr, Backx K, Shave R, Stohr EJ (2016) Cardiac output and related haemodynamics during pregnancy: A series of meta analyses. Heart 102(7): 518- 526.
-
Amundsen BH, Helle Valle T, Edvardsen T, Torp H, Crosby J, et al. (2006) Noninvasive Myocardial Strain Measurement by Speckle Tracking Echocardiography: Validation against Sonomicrometry and Tagged Magnetic Resonance imaging. J Amer Coll Cardiol 47(4): 789-793.
-
Schannwell CM, Zimmermann T, Schneppenheim M, Plehn G, Marx R, et al. (2002) Left ventricular hypertrophy and diastolic dysfunction in healthy pregnant women. Cardiology 97(2): 73-78.
-
Savu O, Jurcut R, Giusca S, Van Mieghem T, Gussi I, et al. (2012) Morphological and functional adaptation of the maternal heart during pregnancy. Circulation Cardiovascular Imaging 5(3): 289-297.
-
Mor Avi V, Lang RM, Badano LP, Belohlavek M, Cardim NM, et al. (2011) Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. Europ J Echocardiography 24(3): 277-313.
-
Estensen ME, Beitnes O, Grindheim G, Aaberge L, Smiseth OA, et al. (2013) Altered maternal left ventricular contractility and function during normal pregnancy. Ultrasound in Obstetrics & Gynecol 41(6): 659-666.
-
Hameed I (2020) Speckle tracking echocardiography: Basic concepts and clinical applications. Pak Heart J 53(1).
-
Lang RM, Badano LP, Mor Avi V, Afilalo J, Armstrong A, et al. (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: An update from The American Society of Echocardiography and The European Association of Cardiovascular Imaging. Journal of the American Society of Echocardiography 28(1): 1-39.
-
Lancellotti P, Cosyns B (2015) The Eacvi Echo Handbook. Oxford University Press.
-
Daniel WW, Cross CL (2018) Biostatistics: A foundation For Analysis in the Health Sciences. Wiley pp: 720.
-
Troiano NH (2018) Physiologic and hemodynamic changes during pregnancy. Aacn Advanced Critical Care 29(3): 273-283.
-
Umesawa M, Kobashi G (2017) Epidemiology of hypertensive disorders in pregnancy: Prevalence, risk factors, predictors and prognosis. Hypertension Res. 40(3): 213-220.
-
Villamor E, Tedroff K, Peterson M, Johansson S, Neovius M, et al. (2017) Association between maternal body mass index in early pregnancy and incidence of cerebral palsy. JAMA 317(9): 925-936.
-
Kutchi I, Chellammal P, Akila A (2020) Maternal obesity and pregnancy outcome: In perspective of new Asian Indian guidelines. The J Obstetrics and Gynecology of India 70(2): 138-144.
-
Kreiner VK, Moertl MG, Papousek I, Zalaudek KS, Lang U, et al. (2018) Maternal cardiovascular and endothelial function from first trimester to Postpartum. PloS One 13(5): e0197748.
-
Garg P, Yadav K, Jaryal AK, Kachhawa G, Kriplani A et al. (2020) Sequential analysis of heart rate variability, blood pressure variability and baroreflex sensitivity in healthy pregnancy. Clinical Autonomic Res 30(5): 433-439.
-
Charkoudian N, Usselman CW, Skow RJ, Staab JS, Julian CG, et al. (2017) Muscle Sympathetic Nerve Activity and Volume-Regulating factors in Healthy Pregnant and Nonpregnant women. Amer J Physiology Heart and Circulatory Physiol 313(4): H782-H787.
-
Ngene NC, Moodley J (2019) Physiology of blood pressure relevant to managing hypertension in pregnancy. The J Maternal Fetal Neonatal Med 32(8): 1368-1377.
-
Sengupta SP, Jaju R, Nugurwar A, Caracciolo G, Sengupta PP (2012) Left ventricular myocardial performance assessed by 2-dimensional speckle tracking echocardiography in patients with sickle cell crisis. Indian Heart J 64(6): 553-558.
-
Cong J, Wang Z, Jin H, Wang W, Gong K, et al. (2016) Quantitative evaluation of longitudinal strain in layer- specific myocardium during normal pregnancy in China. Cardiovascular Ultrasound 14(1): 45.
-
Sengupta SP, Bansal M, Hofstra L, Sengupta PP, Narula J (2017) Gestational changes in left ventricular myocardial contractile function: New insights from two- dimensional speckle tracking echocardiography. The Int J Cardiovascular Imag 33(1): 69-82.
-
Selma ARI, Hasan ARÝ, Yilmaz M, Bozat T (2020) Evaluation of myocardial function in pregnant women with speckle-tracking echocardiography. The Europ Res J 6(6): 615-623.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study