Correlation of Heart Rate Response during Exercise and Recovery with Severity of Myocardial Ischemia as Judged by Electrocardiographic Findings during Treadmill Testing: Increase in Heart Rate during Recovery Suggest Severe Ischemia with Exercise Induced Left Ventricular Dysfunction
We evaluated eighty one patients complaining of angina or angina equivalent symptoms on effort. Treadmill tests were performed using Bruce protocol. All confounding factors were excluded. Severity of exercise induced myocardial ischemia was decided by clinical and electrocardiographic findings during exercise and recovery. Heart rate response during exercise and recovery was correlated with severity of myocardial ischemia. Chronotropic incompetence had low sensitivity but high specificity in diagnosing severe myocardial ischemia. Decreased magnitude of reduction in heart rate during the first minute of recovery also correlated with severe exercise induced myocardial ischemia. Combining the two parameters increased sensitivity with mild reduction in specificity. Increase, rather than decrease, in heart rate during recovery period strongly correlated with severe myocardial ischemia with possibility of exercise induced left ventricular dysfunction.
Introduction
Heart rate response during exercise and recovery is considered important in interpretation of exercise electrocardiographic testing [1, 2]. Both, failure of adequate increase in heart rate during exercise as well as delayed heart rate recovery have been shown to be associated with higher incidence of all-cause mortality [3, 4, 5, 6, 7, 8]. These studies have, however, not excluded various confounding factors [9], and the reason for increased all cause and cardiovascular mortality is not clear.
Thomas & Ellestad have observed higher incidence of coronary artery disease in subjects with chronotropic incompetence [10]. Brener SJ, et al. [11] have also observed that chronotropic response to exercise predicts angiographic severity in patients with suspected or stable coronary artery disease. Lipinski MJ, et al. [12] correlated heart rate recovery with presence of angiographically significant coronary artery disease. These authors considered 50% diameter narrowing as abnormal. It is now known that correlation between angiographic diameter narrowing of 40-70% and presence of myocardial ischemia is poor [13]. Extent of actual myocardial ischemia in their patients is, therefore, not clear. Gera N, et al. [14] has observed that abnormal heart rate recovery was associated with high risk findings on single photon emission computed tomography myocardial perfusion imaging in men.
All these studies, however, suffer from the limitations of coronary artery narrowing in predicting ischemia at the level of myocytes. Fractional flow reserve, intravascular ultrasound and optical coherence tomography have shown disparity in magnitude of obstruction on coronary angiography and presence of myocardial ischemia [15]. Failure of appropriate vasodilatation [16], impairment of microvasculature [16], increased late inward sodium current and metabolic dysfunction at tissue level [17], also contribute to myocardial ischemia.
Electrocardiogram is very sensitive to changes produced in action potential of the cardiac myocytes by ischemia [18, 19], We, therefore, correlated heart rate response during exercise and recovery with electrocardiographic evidence of myocardial ischemia during treadmill stress test.
Material and Methods
Inclusion Criteria
- Patients who complained of angina or angina equivalent symptoms on effort were included irrespective of age and gender.
- Absence of any history of use of antiaginal drugs.
- Normal clinical examination. Absence of systemic hypertension.
- Normal 2-dimensional and colour Doppler echocardiographic examination.
- Normal resting twelve lead electrocardiogram i.e. normal sinus rhythm and absence of any old myocardial infarction, any ST-segment or T wave changes, any evidence of ventricular hypertrophy, intraventricular conduction defect, pre-excitation or paced rhythm.
- Absence of unstable angina or rest angina.
- Absence of history of old myocardial infarction, coronary angioplasty or coronary artery bypasses grafting.
- Absence of any new electrocardiographic changes on standing and during active hyperventilation prior to exercise [20].
- Absence of any chronic systemic illness that could hamper exercise capacity e.g. debility, orthopaedic problems, haemoglobin concentration less than 10gm%, chronic pulmonary disease or pulmonary artery hypertension.
- Absence of any evidence of autonomic neuropathy.
- Resting heart rate more than 55 beats per minute. Resting sinus bradycardia could be due to intrinsic disease of the sinoatrial node or inherently increased parasympathetic tone. This condition could affect the heart rate response during exercise or recovery.
- Absence of any contraindications for exercise testing [21, 22].
Exercise Test Protocol
- Mason-Likar lead system was used. All twelve leads were recorded simultaneously [23].
- Bruce protocol was followed [24].
- Exhaution rather than age adjusted target heart rate was taken as the end point to achieve maximal heart rate [24, 25].
- Exercise was terminated if there was development of angina, any magnitude of ST-segment elevation in leads aVR and/or V1 or any lead without previous infarction. > 1mm of horizontal or downsloping ST-segment depression.
- Patients were immediately placed in supine position without any cool down walk. It is a regular practice in the center.
- Recovery was recorded for nine minutes. Recovery period was extended if indicated.
Exclusion Criteria
- Patients who could not perform adequate exercise for nonischemic reasons.
- New appearance of any intraventricular conduction defect, pre-excitation, bradyarrhythmia, tachyarrhythmia or frequent premature beats during exercise.
- ST-segment depression localized only to inferior leads and associated with rapidly downsloping Pq-segment as such changes could be falsely position [22] Finally eighty one patients qualified for analysis
Evaluation of Heart Rate
Computer derived heart rate was used for analysis. Heart rate was calculated for a period of 3 seconds by the computer. Heart rate was calculated manually if we felt that there was some error in computer calculation of heart rate. Age predicted maximal heart rate was calculated by the formula of Fox et al i.e. 220-age [26]. Heart rate recovery was calculated as heart rate at peak exercise minus heart rate at a particular time during recovery. Recovery heart rate was analysed at the end of first minute, third minute, fifth minute, seventh minute and ninth minute.
Evaluation of ST-Segment Depression
Worst degree of ST-segment depression was considered in deciding the type of abnormality [27]. ST-segment depression was measured 80 msec after the J point. It was measured 60 msec after the J point when the heart rate was more than 130 /minute [2].
Division of Patients in Different Groups According to Electrocardiographic Signs of Myocardial Ischemia during Exercise and/or Recovery
Patients were divided into following groups depending on the severity of ischemia
Group 1- Mild Ischemia Patients with following electrocardiographic changes were included in this group.
- Horizontality of the ST-segment with sharp angled ST- segment - T wave junction (Figure 1) [28].
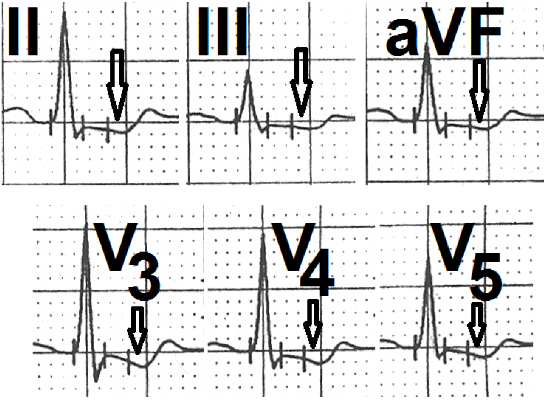
- Upsloping ST-segment depression of 1.5 mm (Figure 2) [1, 29, 30].
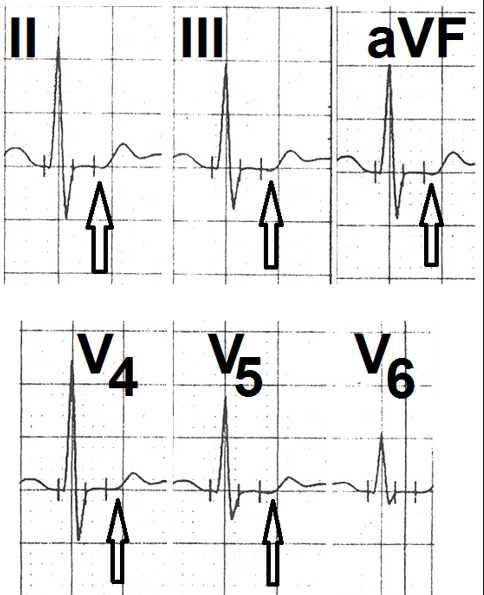
- Horizontal ST-segment depression of more than 1 mm but less than 2mm (Figure 3) [1, 27, 31].
- ST-segment changes appearing after 7 METs of work load [32].
- Normalization of the ST-segment changes within first minute of recovery [33].
Group 2- Moderate Myocardial Ischemia
- Patients with following electrocardiographic changes were included in this group.
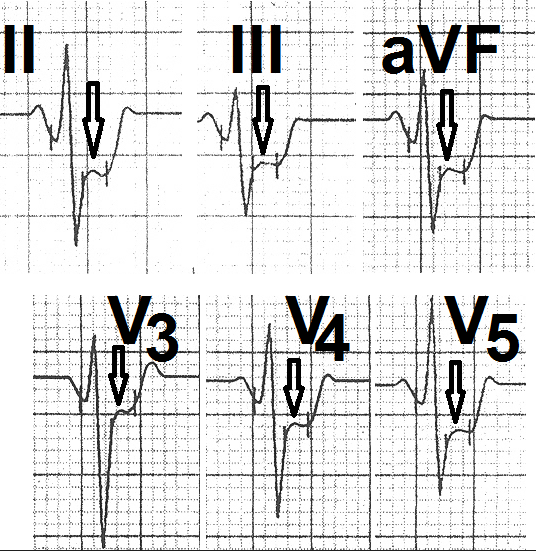
- Horizontal ST-segment depression of more than 2 mm (Figure 4) [29].
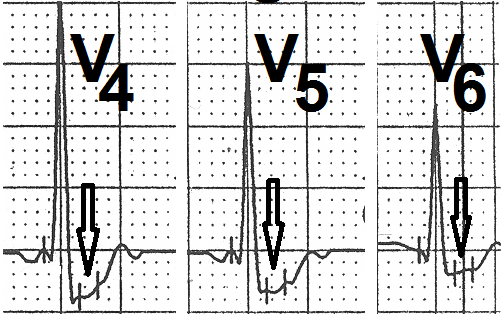
- Downsloping ST-segment depression of less than 2mm (Figure 5) [27].
- Changes appearing between 5-7 METs of work load [32].
- Normalization of the ST-segment in three minutes of recovery [33].
Group 3- Severe Myocardial Ischemia
- Patients with following electrocardiographic changes were included in this group.
- Downsloping ST-segment depression of more than 2mm in five or more leads [29].
- ST-segment elevation in leads aVR and/or V1 (Figures 6a&b) [34, 35, 36].
- Any magnitude of ST-segment elevation in leads without previous infarction [37].
- Changes appearing at a workload of less than 4 METs [32].
- Changes persisting for more than eight minutes during recovery [38].
- Appearance of angina or systolic hypotension [39, 40, 41].
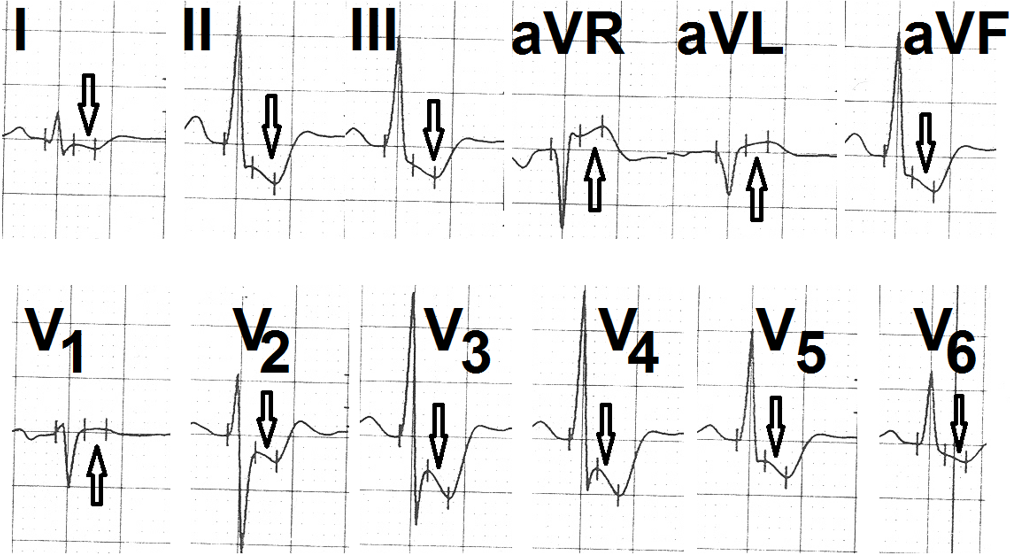
Figure 6a: Leads I, II, III, aVF, V2, V3, V4, and V5 during fifth minute of recovery showing down sloping ST-segment depression (marked as ↓) and ST-segment elevation in leads aVR, aVL and V1 (marked as ↑).
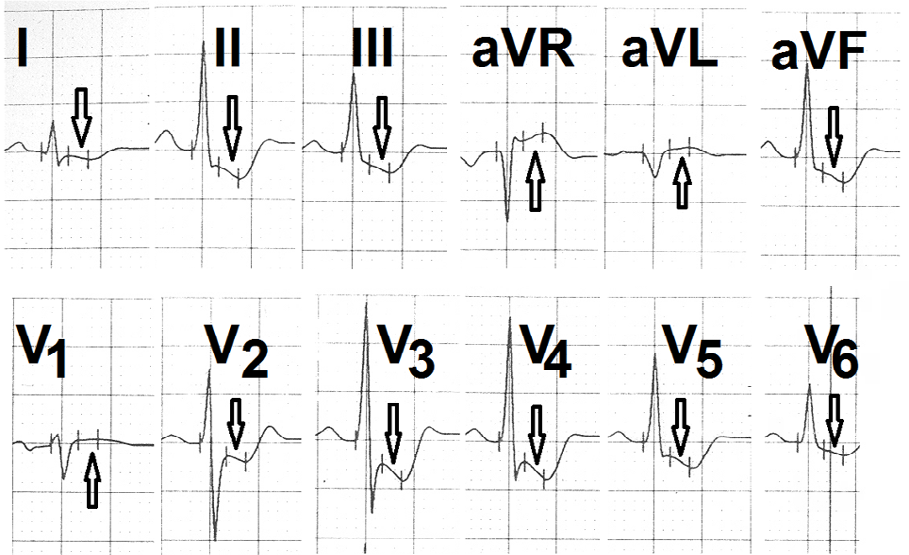
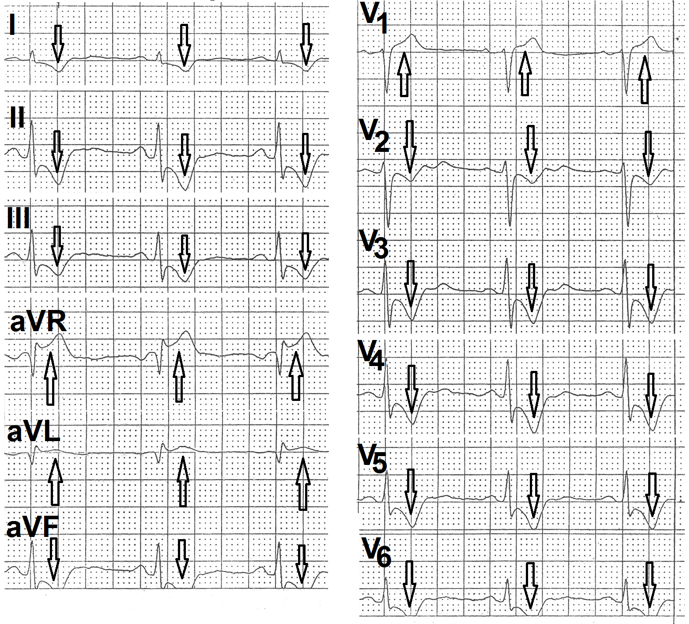
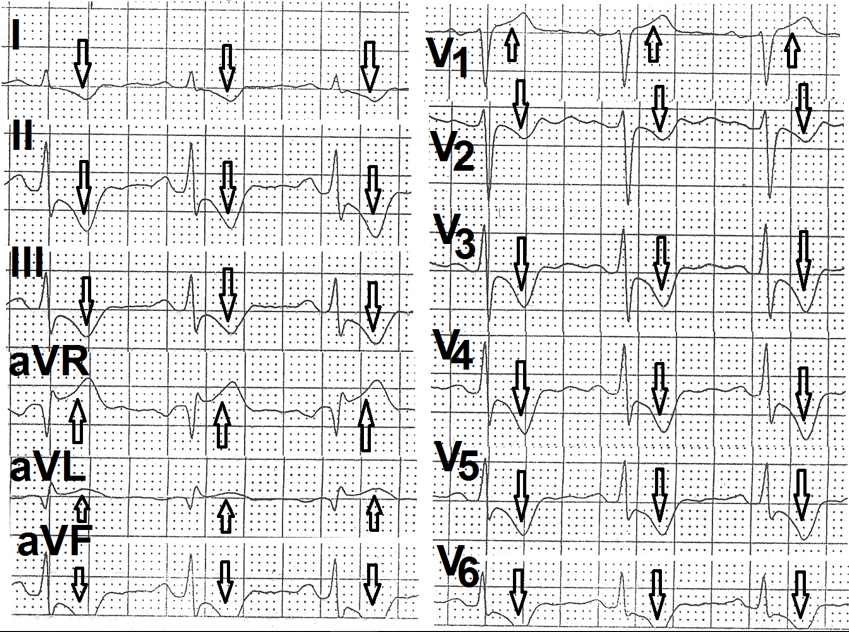
Figure 6b: Electrocardiogram recorded during 9th minute of recovery showing persistence of ST-segment changes.
Statistical Analysis
Difference between different groups was evaluated using unpaired ‘T’ test.
Results
There was no significant difference between the age of group 1 versus group 2 and group2 versus group 3 (Table 1). However, patients of group 3 were significantly older (P<0.01) as compared to patients of group 1 (Table 1). There was no significant difference between the resting supine heart rate and resting supine systolic blood pressure amongst the three groups (Table 1). Resting supine diastolic blood pressure was, however, significantly lower in patients of group 1 as compared to patients of group 2 (P<0.001) and group 3 (P<0.05) Table 1. Diastolic blood pressure in patients of group 2 was, however, higher than the patients of group 1 and 3 (Table 1).
| Parameters | Group 1 | Group 2 | Group 3 | P Values | ||
|---|---|---|---|---|---|---|
| Number of patients | 26 | 25 | 30 | 1 v/s 2 | 2 v/s 3 | 1 v/s 3 |
| Age (years) (mean±SD) | 53.44±9.67 | 57.40±9.99 | 59.30±11.57 | >0.10 (NS) | >0.10 (NS) | >0.01 (S) |
| HR/min (mean±SD) | 76.3±12.69 | 76.07±15.58 | 75.02±14.98 | >0.10 (NS) | >0.10 (NS) | >0.10 (NS) |
| SBP(mm Hg) (mean±SD) | 121.70±8.88 | 124.36±8.11 | 119.65±14.39 | >0.10 (NS) | >0.10 (NS) | >0.10 (NS) |
| DBP(mm Hg) (mean±SD) | 68.88±11.76 | 82.65±6.41 | 77.21±8.53 | >0.001 (VS) | <0.01 (S) | <0.05 (S) |
Table 1: Baseline parameters.
Duration of exercise was maximum in patients of group 1 (Table 2). However, it was significantly lower in patients of group 2 (P<0.001) and group 3 (P<0.001) (Table 2). There was no significant difference in peak exercise heart rate of group
1 and 2 (P>0,10) (Table 2). However, individuals of group 3 attained relatively lower heart rate (p=0.05) as compared to patients of group 1 (Table 2). Increase was maximal in group 2 as compared to patients of group 3 (P=0.01) (Table 2).
| Parameters | Group 1 | Group 2 | Group 3 | P Values | ||
|---|---|---|---|---|---|---|
| 1 v/s 2 | 2 v/s 3 | 1 v/s 3 | ||||
| Exercise duration in minutes (mean±SD) | 10.25±1.86 | 8.35±1.62 | 6.32±2.06 | <0.001 (VS) | <0.01 (S) | <0.001 (VS) |
| Peak heart rate (mean±SD) | 161.31±13.56 | 158.41 ± 20.28 | 149.88±25.73 | >0.10 (NS) | >0.10 (NS) | 0.05 (BLS) |
| Incidence of chronotropic incompetence | 1 (3.84%) | 2 (8%) | 3 (23.33%) | |||
| Percentage of age predicted maximal heart rate/minute (mean±SD) | 98.76±7.76 | 101.33±15.6 | 94.80±14.76 | >0.10 (NS) | 0.01 (S) | 0.05 (BLS) |
Table 2: Exercise parameters.
Incidence of chronotropic incompetence (peak exercise heart rate less than 85% of the age predicted maximal heart rate) increased progressively from group 1 (one patient,( 3.84%)) to group 2 (two patients 8%) and group 3 (seven patients, 23.33%) (Table 2). We tried to evaluate the diagnostic significance of this observation by pooling peak heart rate of another 97 individuals who did not have any electrocardiographic evidence of myocardial ischemia during the treadmill test [2, 29]. Nine of these 97 individuals had peak heart rate less than 85% of their age predicted maximal heart rate. Results are shown in Table 3. Chronotropic incompetence had low positive predictive value, high negative predictive value and high test accuracy.
| Sensitivity | 23.33% |
|---|---|
| Specificity | 94.98% |
| Predictive value of a positive test | 36.84% |
| Predictive value of a negative test | 85.25% |
| Test accuracy | 80.89% |
Table 3: Value of chronotropic incompetence in diagnosing severe myocardial ischemia.
Heart rate recovery at the end of first minute was significantly more (P<0.001) in patients of group 1 as compared to patients of group 2 and group 3 (Table 4). Heart rate recovery by the end of third minute was also significantly higher in patients of group 1 as compared to patients of group 2 (P 0.01) and group 3 (P<0.001) (Table 4). Difference between group 2 and group 3 was, however, not significant (P>0.10) (Table 4). By the end of fifth minute of recovery, decline in heart rate was again significantly greater in patients of group 1 as compared to group 2 (P<0.05) and group 3 (P<0.001) (Table 4). Difference between patients of group 2 and 3 was, however, not significant (P>0.10) (Table 4). Same trend was seen in heart rate recovery by the end of seventh minute and ninth minute of recovery (Table 4). Overall, the heart rate recovery was greatest in patients of group 1 and minimal in patients of group 3 during all stages of recovery.
| Parameters | Group1 | Group2 | Group3 | P Values | ||
|---|---|---|---|---|---|---|
| 1 v/s 2 | 2 v/s 3 | 1 v/s 3 | ||||
| Heart rate recovery by the end of first minute (beats/ min) (mean±SD) | 33.86±15.94 | 20.44±11.29 | 19.08±16.61 | <0.001 (VS) | >0.10 (NS) | <0.001 (VS) |
| Heart rate recovery by the end of third minute (beats/min) (mean±SD) | 60.79±12.87 | 51.29±14.88 | 46.88±17.51 | 0.01 (S) | >0.10 (NS) | <0.001 (VS) |
| Heart rate recovery by the end of fifth minute (beats/ min) (mean ± SD) | 63.03±12.54 | 56.84±13.68 | 51.58±15.33 | <0.05 (S) | >0.10 (NS) | <0.001 (VS) |
| Heart rate recovery by the end of seventh minute (beats/min) (mean ± SD) | 67.92±10.90 | 57.96±14.17 | 54.94±15.89 | <0.01 (S) | >0.10 (NS) | <0.001 (VS) |
| Heart rate recovery by the end of ninth minute (beats/min) (mean ± SD) | 67.33±11.34 | 61.52±14.99 | 51.26±13.15 | >0.10 (S) | <0.01 (S) | <0.001 (VS) |
Table 4: Heart rate recovery parameter.
We tried to analyse reduction in heart rate during different periods of recovery in different groups. Results are shown in Table 5. Significant differences were seen only in reduction in heart rate during the first minute of recovery.
It became clear that significant difference seen during subsequent periods of recovery in Table 3 were only due to impact of difference seen during the first minute of recovery.
| Time | Group 1 | Group 2 | Group 3 | P Values | ||
|---|---|---|---|---|---|---|
| 1 v/s 2 | 2 v/s 3 | 1 v/s 3 | ||||
| First minute | 33.86±15.94 | 20.44±11.29 | 19.08±16.61 | <0.001 (VS) | >0.10 (NS) | <0.001 (VS) |
| Second and third minute | 28.92±10.97 | 31±11.68 | 28.43±15.10 | >0.10 (NS) | >0.10 (NS) | >0.10 (NS) |
| Fourth and fifth minute | 4.57±4.59 | 6.16±7.15 | 6.8±6.78 | >0.10 (NS) | >0.10 (NS) | >0.05 (NS) |
| Sixth and seventh minute | 2.66±2.81 | 1.70±2.34 | 2.66±4.86 | >0.10 (NS) | >0.10 (NS) | >0.10 (NS) |
| Eigth and ninth minute | 3±3.24 | 1.76±3.40 | 2.31±3.26 | >0.10 (NS) | >0.10 (NS) | >0.10 (NS) |
Table 5: Timewise reduction in heart rate during recovery (mean±SD).
We also observed that one patient in group 2 and fifteen patients of group 3 showed increases, rather than decrease in heart rate during second to ninth minutes of recovery. We tried to evaluate the diagnostic significance of this observation by pooling heart rate recovery response of another 97 normal individuals who did not have any electrocardiographic evidence of myocardial ischemia during treadmill test [2, 29]. Nine of these 97 individuals also had increase in heart rate during recovery. Results are shown in Table 6. Increase in heart rate during recovery had high specificity and high negative predictive value in diagnosing severe myocardial ischemia.
| Sensitivity | 53.33% |
|---|---|
| Specificity | 92.56% |
| Predictive value of a positive test | 59.25% |
| Predictive value of a negative test | 90.72% |
| Test accuracy | 85.95% |
Table 6: Diagnostic value of increase in heart rate during recovery period in diagnosing severe myocardial ischemia.
We also tried to evaluate the diagnostic value of combination of both electrocardiographic findings i.e. chronotropic incompetence and/or increase in heart rate during recovery. Result is shown in Table 7. Combining the two variables increased sensitivity with mild reduction in specificity without significant change in test accuracy.
| Sensitivity | 73.07% |
|---|---|
| Specificity | 82.43% |
| Predictive value of a positive test | 73.07% |
| Predictive value of a negative test | 94.57% |
| Test accuracy | 79.21% |
Table 7: Diagnostic value of combined chronotropic incompetence and/or increase in heart rate during recovery in diagnosing sever
Discussion
Chronotrpic Incompetence and Myocardial Ischemia
Chronotropic incompetence is defined as inability to increase heart rate to at least 85% of age predicted maximum heart rate. Chronotropic imcompetence is considered as an important predictor of future cardiac events [43, 44]. However the mechanism of such association is not clear [11].
Previous studies evaluating this parameter have significant limitations. Chin CF, et al. [45] evaluated subjects whose pulse rate for the achieved workloads was below the 95% confidence limit of the established normal for age and sex. They observed that 72% of the patients with chronotropic incompetence but without ST-segment depression had significant coronary heart disease. Important limitation of the study was that obstruction of 50% or more was taken as evidence of coronary artery disease. Now it is clear that large number of individuals with luminal narrowing of 50 to 70% may not have physiological ischemia [15]. This is also clear from the fact that these individuals did not have any ST- segment depression. Secondly patients with both stress tests and coronary angiograms were retrospectively selected. This introduces significant selection bias. Thirdly, authors themselves observed that autonomic dysfunction rather than myocardial ischemia was a possible pathophysiologic mechanism for chronotropic incompetence.
Pratt CM, et al. [46] evaluated 200 women with history of chest pain compatible with angina and having ST-segment depression > 1 mm during a Bruce treadmill test. 120 women with angiographically normal coronary arteries were considered false negative. Ability to reach target heart rate (90 % of age predicted maximum heart rate (P = 0.027) was only one of the four variables which, when combined, could help correct classification of 71% patients. Details of number of patients who could not attain target heart rate are not provided. Further, now, it is well established that females with angina and ST-segment changes during exercise but normal epicardial coronaries on angiogram have interactions of microvascular disease, autonomic nervous system, inflammation, hormones and endothelial dysfunction. Patients studied by Pratt CM, et al. [46] also had definitive or probable angina which resulted in coronary angiography. Other important limitations of the study include non-exclusion of 30 patients of MVP, patients taking digitalis and patients having resting ST-segment abnormalities Echocardiography was also not performed before stress test.
Brener SJ, et al. [11] observed that chronotropic response to exercise predicts the presence and angiographic severity of coronary disease in patients with suspected or stable coronary artery disease. Angiographic findings were obtained within 180 days of the test. Significant coronary disease was defined as > 1 stenosis of > 50% in a major epicardial coronary artery or its main branches. Severe coronary disease was defined as > 50% stenosis in all 3 epicardial coronary arteries or in the left main coronary trunk, or 2 vessel diseases with > 70% left anterior descending artery stenosis. Authors felt that the association was likely related to the proportion of the left ventricular myocardium rendered ischemia during stress. Authors also concluded that chronotropic response strongly correlated with proximal involvement of LAD artery and thus related to a large territory of jeopardized myocardium. However, their study had several limitations. Significant number of their patients in the lowest tertile of peak heart rate had systemic hypertension, was current smokers, and had previous myocardial ischemia and patients with NYHA class > 11. All these could affect exercise duration and chronotropic response. Large number of their patients in the lowest tertile of peak heart rate developd angina or abnormal ST-segment elevation in non-Q-wave leads. These factors could also affect exercise capacity and chronotropic response. Coronary artery luminal obstruction of 50 to 70% was taken as criteria for coronary artery stenosis. Now it is clear that physiological significance of luminal narrowing in the range of 50 to 70% needs evaluation of physiological significance by fractional flow reserve.15 or nuclear perfusion studies.
Wiens RD, et al. [49] observed that only 16 of their 172 patients had a peak exercise heart rate below two standard deviation of the mean. They concluded that chronotropic incompetence is a relatively infrequent occurrence in an exercise test population. However, when present, this finding is relatively specific for coronary artery disease. We also observed that chronotropic incompetence is infrequent. Large number of patients with severe myocardial ischemia may not have chronotropic incompetence.
We observed that chronotropic incompetence had low sensitivity (36.66 %) but high specificity (93.91 %) in diagnosing severe myocardial ischemia. Other workers have also observed that persons with single or even multivessel disease can achieve 85% of age predicted maximal heart rate [50].
Mechanism of chronotropic incompetence and it’s correlation with myocardial ischemia is not clear. Chin CF, et al. [45] observed obstruction to flow proximal to the origin of the sinus node artery only in two cases. They, therefore, concluded that ischemia of the sinus node did not contribute to chronotropic incompetence. Brener SJ, et Al. [11] also did not observe any statistical association between coronary disease limited to the proximal right coronary artery and the various chronotropic parameters. Chin CF, et al. [45] observed that intrinsic heart rate was lower than expected in some of their patients with chronotropic incompetence. They, therefore, concluded that autonomic dysfunction was a possible pathophysiologic mechanism for chronotropic incompetence. Brener SJ, et al. [11] observed correlation between the size of the ischemic left ventricular territory and the chronotropic response. They also observed that chronotropic response strongly correlated with proximal left anterior descending artery involvement and thus related to a larger territory of jeopardized myocardium. We also observed that the incidence of chronotropic incompetence increased with increasing severity of myocardial ischemia.
Significant myocardial ischemia prevents adequate exercise and could contribute to chronotropic incompetence.
Reduced Heart Rate Recovery and Myocardial Ischemia
We observed that magnitude of reduction in heart rate during the first minute of recovery from treadmill exercise test was significantly less (P< 0.001) in group two (moderate ischemia) and group three (severe ischemia) as compared to group 1 (mild ischemia). There was no significant difference in reduction in heart rate in different groups during remaining period of recovery i.e. second to ninth minute. Decreasing reduction in heart rate during recovery was, thus, suggestive of increasing myocardial ischemia during exercise. Vagal reactivation plays an important role in reduction of heart rate during the first thirty seconds after exercise [51]. Heart rate reduces as vagal reactivation takes over the sympathetic stimulation that occurs during exercise. Our observations, thus, show that with increasing myocardial ischemia, exercise induced stimulation of the sympathetic system continue to dominate over vagal reactivation for a longer period during recovery.
Lipinsky, et al. [12] did a retrospective analysis of exercise treadmill and coronary angiographic data of 2193 men and concluded that heart rate decrease during the second minute of recovery significantly predicted the presence of coronary artery disease. Heart rate recovery at one minute was not significantly affected by whether coronary artery disease was present or not. Their study, however, had several limitations. Firstly these authors studied only males. Reasons for termination of exercise were angina, 2mm of abnormal ST-segment depression, decrease in systolic blood pressure or ominous arrhythmias. Thus all of their cases had severe myocardial ischemia. Thirdly, 34% of their cases were taking betablockers and 4.4% were taking digitalis. Fourthly, the group of patient with coronary artery disease were older, had higher incidence of prior myocardial infarction, diabetes mellitus, stroke and congestive heart failure. Thus the group of patients with coronary artery disease was not similar to the group without coronary artery disease. Finally 50% of luminal diameter stenosis was taken as criteria for coronary artery disease. Now we know that 50% luminal obstruction does not predict physiological ischemia [13]. All these factors could have influenced their results.
Gera N, et al. [14] evaluated 509 men who were referred for exercise stress myocardial perfusion imaging - without ischemic electrocardiographic changes or angina during treadmill testing. Abnormal heart rate recovery was defined as a decrease of 12 beats or less at the first minute after maximal exercise. This finding correlated with presence of mild or greater coronary artery disease (P=0.003) or severe coronary artery disease (p=0.001). This study also had several limitations. Firstly only males were studied. Secondly highly selected patients with strong suspicion of myocardial ischemia who were referred for stress myocardial perfusion imaging, were studied. Thirdly, the group with abnormal heart rate recovery were older (p<0.001), had diabetes (p=0.01), were smokers (p<0.01), used betablockers (P<0.001) or calcium channel blockers (P=0.001). During exercise testing also, this group was significantly different from the group without abnormal heart rate response. This group attained lower peak heart rate (P<0.001) and had lower left ventricular ejection fraction (P < 0.001). All these factors could have significant effect on the results.
Increase in Heart Rate During Recovery
We observed that sixteen patients (one from group 2 and fifteen from group 3) had increase (rather than decrease) in heart rate during recovery. Representative tracing from one case are shown in Figures 7 and 8.
This finding had high specificity in diagnosing severe myocardial ischemia. This finding has not been observed by previous workers. This finding is difficult to explain. It is possible that these patients had significant exercise induced left ventricular dysfunction. We placed the patients in supine position soon after exercise. Putting the patient immediately in supine position suddenly increases the venous return. This increases the filling of the left ventricle and left ventricular end diastolic volume. Left ventricular end diastolic volume is an important determinant of myocardial oxygen demand. Sudden increase in left ventricular end diastolic volume increases myocardial oxygen demand and aggravates myocardial ischemia. A patient with pre-existing left ventricular dysfunction may develop aggravation of left ventricular dysfunction resulting from transient increase in myocardial ischemia due to sudden supine position. Increased left ventricular end-diastolic volume and deterioration of left ventricular function result in reflex increase in sympathetic drive and resultant increase in heart rate. If this increase in sympathetic drive is more than the parasympathetic reactivation occurring normally during recovery period, it may result in an increase rather than a decrease in heart rate. Our observation, therefore, suggest that increase rather than decrease in heart rate during recovery suggests severe myocardial ischemia with exercise induced left ventricular dysfunction.
Possible Limitations of this Study
Some confounding factors that are not well known at present could have affected our interpretation of the electrocardiograms. We excluded various confounding factors known at present. Autonomic neuropathy was excluded only by clinical examination. Some degree of subclinical autonomic neuropathy could have remained undetected.
Conclusion
Our study suggests that chronotropic incompetence has low sensitivity but high specificity in diagnosing severe myocardial ischemia. Decreased magnitude of reduction in heart rate during the first minute of recovery also suggests severe exercise induced myocardial ischemia. Combining the two parameters increases sensitivity without significant reduction in specificity. Increase, rather than decrease in heart rate during recovery period is highly specific of severe myocardial ischemia and suggests exercise induced left ventricular dysfunction.
References
-
Thomas GS, Elleated MH (2017) Electrocardiographic exercise testing. In: Fuster V, Harrington RA, et al. (Eds.), Hurst’s The Heart, pp: 318-334.
-
Balady GJ, Morise AP (2019) Exercise electrocardiographic testing. In: Zipes DP, Libby P, et al. (Eds.), Braunwald’s Heart Disease, Elsevier, pp: 154-173.
-
Lauer MS, Okin PM, Larson NG, Evans JC, Levy D (1996) Impaired heart rate response to graded exercise. Prognostic implication of chronotropic incompetence in the Framingham heart study. Circulation 93(8): 1520- 1526.
-
Adabag AS, Granditis GA, Prineas RJ, Crow RS, Bloomfield HE, et al. (2008) Relation of heart rate parameters during exercise test to sudden death and all-cause mortality in asymptomatic men. Am J Cardiol 101(10): 1437-1443.
-
Lauer MS, Francis GS, Okin PM, Pashkow FJ, Snader CE, et al. (1999) Impaired chronotropic response to exercise stress testing as a predictor of mortality. JAMA 281(6): 524-529.
-
Colo CR, Blackstone EH, Pashkow FJ, Snader CE, Lauer MS (1999) Heart rate recovery immediately after exercise as a predictor of mortality. New Eng J Med 341(18): 1351- 1357.
-
Morshedi Meibadi A, Larson MG, Levy D, Donnel CJ, Vasan RS (2002) Heart rate recovery after treadmill exercise testing and risk of cardiovascular disease events. (The Framingham heart study). Am J Cardiol 90(8): 848-852.
-
Coley CR, Foody JM, Blackstone EH, Lauer MS (2000) Heart rate recovery after submaximal exercise testing as a predictor of mortality in cardiovascularly healthy cohort. Ann Intern Med 132(7): 852-856.
-
Mittal SR (2021) Significance of heart rate profile during treadmill stress test-A critical appraisal. J Cardiol 5(1): 000155.
-
Thomas GS, Ellestad MH (2018) Parameters to be measured during exercise. In Thomas GS, Wann LS, et al. (Eds.), Ellestad’s Stress Testing. 6th (Edn.), Oxford, New Delhi, pp: 82-105.
-
Brener SJ, Pashkow FJ, Harvey SA, Marwick TH, Thomas JD, et al. (1995) Chronotropic response to exercise predicts angiographic severity in patients with suspected or stable coronary artery disease. Am J Cardiol 76(17): 1228-1232.
-
Lipinski MJ, Vetrovec GW, Froelicher VF (2004) Importance of the first two minutes of heart rate recovery after exercise treadmill testing in predicting mortality and the presence of coronary artery disease in men. Am J Cardiol 93(4): 445-449.
-
Kern MJ, Seto AH (2017) Cardiac catheterization, cardiac angiography and coronary blood flow and pressure measurements. In: Fuster V, Harrington RA, et al. (Eds.), Hurst’s The Heart. Mc Graw Hill Education, New York, pp: 606-656.
-
Gera N, Taillor LA, Ward RP (2009) Usefulness of abnormal heart rate recovery on exercise stress testing to predict high risk finding on single photon emission computed tomography myocardial perfusion imaging in men. Am J Cardiol 103(5): 611-614.
-
Winchester DE, Pepine CJ (2017) Non obstructive and non-atherosclerotic coronary heart disease. In: Fuster V, Harrington RA, et al (Eds.), Hurst’s The Heart. Mc Graw Hill Education, New York, pp: 923-945.
-
Aziz A, Hansen HS, Sechtem U, Prescott E, Ong P (2017) Sex related differences in vasomotor function in patients with angina and unobstructed coronary arteries. J Am Coll Cardiol 70(19): 2349-2358.
-
Soukouli V, Boden WE, Smith SC Jr, O Gara PT (2014) Non- atherothrombotic medical options in acute coronary syndromes: old agents and new lines on the horizon. Circ Res 114(12): 1944-1958.
-
Mirvis DM, Goldberger AL (2019) Electrocardiography. In: Zipes DP, Libby P Bonow RO, et al. (Eds.), Braunwald’s Heart Disease. Elsevier, Philadelphia, pp: 117-151.
-
De Luna AB, Goldwasser D, Fiol M, Bayes-Genis A (2017) Surface electrocardiography. In: Fuster V, Harrington RA, et al. (Eds). Hurst’s The Heart, Mc Graw Hill, New York, pp: 252-317.
-
Mittal SR, Mittal G (2021) Effect and significance of electrocardiographic changes on standing and hyperventilation prior to exercise electrocardiographic testing. J Cardiol 5(1): 000168.
-
Thomas GS, Ellestad MH (2018) Contraindications and safety for stress testing In: Thomas GS, Wann LS, Ellestad MH. (Eds,). Ellestad’s Stress Testing, Oxford, UK, pp: 71- 81.
-
Sapin PM, Koch G, Blaumet MB, Mc Carthy JJ, Hinds WS, et al. (1991) Identification of false positive exercise test with the use of electrocardiographic criteria. J Am Coll Cardiol 18(1): 127-135.
-
Mason RE, Likar I (1996) A new system of multiple lead exercise electrocardiography. Am Heart J 71(2): 196- 205.
-
Bruce R, Blackman J, Jones J, Strait J (1963) Exercise testing in adult normal subjects and cardiac patients. Pediatrics 32: 742-756.
-
Jain M, Nikonde C, Lin BA, Walker A, Wackers FJ (2011) 85% of maximal age predicted heart rate is not a valid end point for exercise treadmill testing. J Nucl Cardiol 18(6): 1026-1035.
-
Fox S III, Naughton JP, Haskell WL (1971) Physical activity and the prevention of coronary heart disease. Ann Clin Res 3: 404-432.
-
Goldschlager N, Selzer A, Cohn K (1976) Treadmill stress test as indicator of presence and severity of coronary artery disease. Ann Intern Med 85(3): 277-286.
-
Schmroth L (1982) Coronary insufficiency. In: Schmroth C (Ed.), an introduction to Electrocardiography. Blackwell Science, France, pp: 157-185.
-
Thomas GS, Wann LS, Ellestad MH (2018) Predicting prognosis with the exercise test: Putting it all together. In: Thomas GS, Wann LS, et al. (Eds). Ellestad’s Stress Testing. Oxford, UK, pp: 229-267.
-
Potizos G, Ellestad MH (2006) The value of upsloping ST depression in diagnosing myocardial ischemia. Ann Nonivas Electro 11(3): 237-240.
-
Martin CM, Mc Conahy DR (1972) Maximal exercise electrocardiography. Correlation with coronary angiography and cardiac hemodynomics. Circulation 46(5): 956-962.
-
Ellestad MH, Thomas L, Ong R, Loh J (1992) The predictive value of the time course of ST-segment depression during exercise testing in patients referred for coronary angiograms. Am Heart J 123(4): 904-908.
-
Okin PM, Amcisen O, Kligfield P (1989) Recovery phase patterns of ST-segment depression in the heart rate domain. Identification of coronary artery disease by the rate-recovery loop. Circulation 80(3): 533-541.
-
Vorobiof G, Ellestad MH (2011) Lead a VR : dead or simply forgotten?. JACC Cardiovasc Imag 4(2): 187-190.
-
Halon DA, Mevorach D, Rodeanu M, Lewin BS (1994) Improved criteria for localization of coronary artery disease from the exercise electrocardiogram. Cardiology 84(4-5): 331-338.
-
Katircibasi MT, Kocum HT, Tekin A, Erol T, Tekin G, et al. (2008) Exercise induced ST-segment elevation in leads aVR and V1 for the prediction of left main disease. Int J Cardiol 128(2): 240-243.
-
Sriwattanakomen S, Tiozon AR, Zubritzky SA, Blobner CG, Rice M, et al. (1980) ST-segment elevation during exercise: electrocardiographic and angiographic correlation in 38 patients. Am J Cardiol 45(4): 762-768.
-
Callaham PR, Thomas L, Ellestad MH (1987) Prolonged ST-segment depression following exercise predicts significant left coronary stenosis. Circulation 76(3): 253.
-
Weiner DF, Mc Cobe C, Huster DC, Ryan TJ, Hord WB Jr (1978) The predictive value of anginal chest pain as an indicator of coronary artery disease during exercise testing. Am Heart J 96(4): 458-462.
-
Tavel ME, Shaar C (1999) Relation between electrocardiographic test and degree and location of myocardial ischemia. Am J Cardiol 84(2): 119-124.
-
Le VV, Mitiku T, Sungar G (2008) The blood pressure response to dynamic exercise testing : a systematic review. Prog Cardiovasc Dis 51(2): 135-160.
-
Students ‘T’ test- an overview.
-
Ellestad MH, Wan MKC (1975) Predictive implication of stress testing. Follow-up of 2700 subjects after maximal treadmill stress testing. Circulation 51(2): 363-369.
-
Bruce RA, De Rouen TA, Hossack KP (1980) Value of maximal exercise tests in risk assessment of primary coronary heart disease events in healthy men. Five years’ experience of the Seattle heart watches study. Am J Cardiol 46(3): 371-378.
-
Chin CF, Messenger JC, Greenberg PS, Ellestad MH (1979) Chronotropic incompetence in exercise testing. Clin Cardiol 2(1): 12-18.
-
Pratt CM, Francis MJ, Divine GW, Young JB (1989) Exercise testing in women with chest pain: Are there additional exercise characteristics that predict true positive test results?. Chest 95(1): 139-144.
-
Pepine CJ (2015) Multiple causes for ischemia without obstructive coronary artery disease: not a short list. Circulation 131(12): 1044-1046.
-
Pepine CJ, Ferdinand KC, Shaw LJ, Light McGroary KA, Shah RU, et al. (2015) Emergence of non-obstructive coronary artery disease: a woman’s problem and need for change in definition on angiography. J Am Coll Card 66(17): 1918-1933.
-
Wiens RD, Lafia P, Marder CM, Evans RG, Kennedy HL (1984) Chronotropic incompetence in clinical exercise testing. Am J Cardiol 54(1): 74-78.
-
Thomas GS (2018) Heart rate response to exercise. In: Thomas GS, Wann LS, et al. (Eds.), Ellestad’s Stress Testing. Oxford, New York, pp: 437-445.
-
Imami K, Sato H, Hori M, Kusuoka H, Ozaki H, et al. (1994) Vagally Mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J Am Coll Cardiol 24(6): 1529- 1535.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study