Management of a Case of Acute Ischaemic Stroke with Large Vessel Occlusion in an LVAD Patient; A UK Secondary Medical Center Experience
Introduction: Left ventricular assist devices (LVADs) are getting more popular in managing advanced heart failure patients. The implantation of LVADs is associated with neurological complications, including ischemic stroke or intracranial hemorrhage. There are no current guidelines on how to manage these neurological complications. In this report, we presented an LVAD patient with a large ischemic cerebral infarct and subarachnoid hemorrhage simultaneously and outlined our approach to managing these complications without affecting the LVAD function. Case presentation: A 34- year-old gentleman with an LVAD to bridge him to heart transplantation presented with acute left-sided body weakness of an undetermined time of onset. His CT head showed a large right middle cerebral artery infarct. He was not a thrombolysis candidate due to the undetermined onset of his stroke, the anticoagulation he was on for the LVAD, and the signs of infarct maturation in the CT head. We managed him in a multidisciplinary team approach holding the Aspirin and Warfarin he was taking and doing serial CT imaging of his brain to monitor the development of brain edema. The patient developed a small subarachnoid hemorrhage on day 2, that spontaneously resolved on day 5. We started him on unfractionated heparin on day 7 and Warfarin on day 10. We made an excellent recovery of his neurological function without impairment of the function on the LVAD. Conclusion: Simultaneous ischemic stroke and brain hemorrhage are a challenge in LVAD patients. A closely monitored stoppage of antithrombotics and serial brain imaging can guide the treatment. Regular assessment of LVAD function is mandated. Antithrombotics could be carefully reintroduced under surveillance brain scanning to maintain the LVAD function.
Introduction
Continuous flow left ventricular assist devices (CF- LVADs) are used for patients with cardiomyopathy, either as a bridge to transplant or destination treatment [1]. LVADs improve the patient’s functional capacity but increase their risk of bleeding and embolic events [2]. Different antithrombotic strategies have been used in CF-LVAD patients, combining Aspirin (at different doses from 75 mg to 325 mg) and Warfarin (at different INR targets 1.5 to 2 or 2 to 3). None have proven to fully protect LVAD patients from embolic events [3]. Acute ischaemic stroke (AIS) is a dreadful complication for patients with LVAD. Some centers consider it a contraindication of heart transplantation [4]. There are no guidelines for the management of AIS in LVAD patients. We hereby present a case of a young man with therapeutic INR and presented outside the window for reperfusion therapy with concomitant middle cerebral artery (MCA) large vessel occlusion (LVO), and frontal subarachnoid hemorrhage (SAH).
Case Presentation
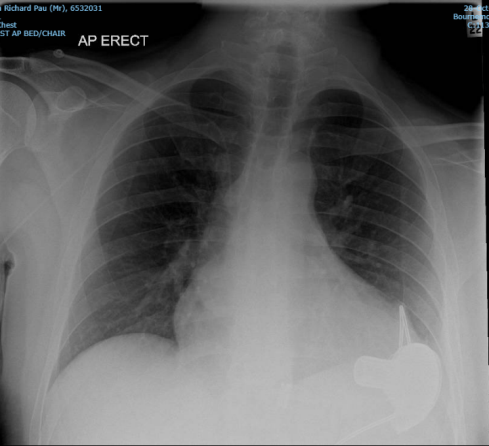
A 34-year-old gentleman, mRS 0 presented in the early hours to our stroke unit with left hemiparesis and dysarthria, having last felt well the night before. He is a known case of dilated cardiomyopathy and has CF-LVAD (Heartware; Medtronic, Minnesota, USA) inserted in 2015 as a bridge to a heart transplant. He was maintained on Aspirin 150 mg and Warfarin 15 mg once daily, with an INR of 3.2 on admission (his target INR was 2-3). He also has chronic driveline infection, managed by long-term Ertapenem. His LVAD parameters were within his baseline parameters: Power (3.8 Watts), flow (3.7 liter/min), and speed (2600 RPM) (Figure 1).
On examination, his mean arterial pressure (MAP) was 70 mmHg using an ultrasound Doppler probe. His initial National Institutes of Health Stroke Scale (NIHSS) was 20, with a Glasgow Coma Scale (GCS) of 14 due to confusion. He was in sinus rhythm, euglycemic, and apyrexial, with no evidence to suggest co-infection with COVID-19 on his polymerase chain reaction (PCR) test. He had muscle power 3/5 in the left upper and lower limbs on the Medical Research Council (MRC) Scale for Muscle Strength. The power in the right-sided limbs, the sensations, and the coordination in both upper and lower limbs were preserved. His cranial nerve examination and speech were normal. We found no bruits on his carotid arteries; his cardiac and chest examinations were unremarkable.
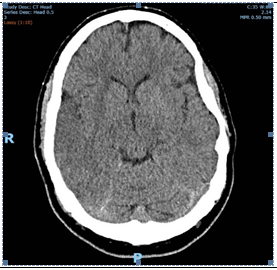
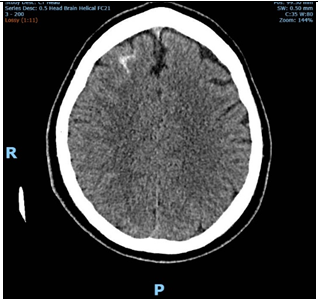
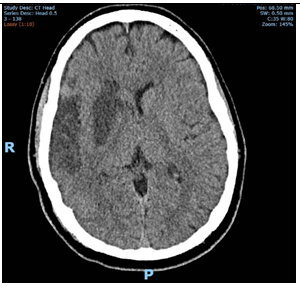
His initial CT brain showed a proximal M1 thrombus with significant early ischaemic changes. Reperfusion therapy could not be considered due to late presentation, evidence of significant early changes, Alberta Stroke Program Early CT Score (ASPECTS) of 5, and the therapeutic INR (Figures 2 and 3).
We discussed the case within a multidisciplinary team (MDT) involving the stroke team, a hematologist, and his heart failure team. Daily full blood count (FBC), bilirubin, lactate dehydrogenase (LDH) levels, and device parameters (power, watts, and speed) were checked for evidence of pump thrombosis or hemolysis. They have been stable all through his hospital stay. His transthoracic echo study did not suggest pump thrombosis.
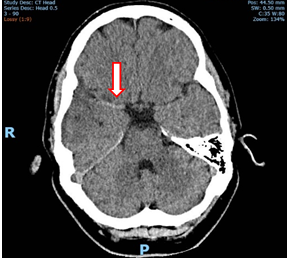
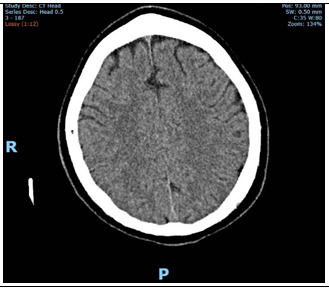
Due to the high risk of malignant MCA syndrome and no in-house neurosurgical unit, he underwent serial brain imaging on days 2,3, and 7 of his stay. A streak of spontaneous SAH was found on his CT on day 2, which was stable on day 3 and disappeared on day 5. No signs of increased intracranial pressure were found on serial CT scans (Figures 4-7).
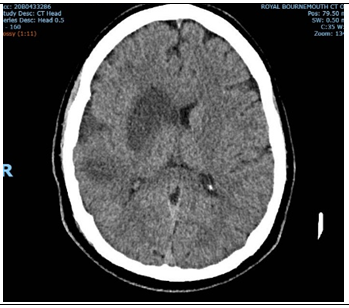
On day 7, he was commenced on IV Unfractionated heparin (UFH) infusion, with a target APTT ratio of 1.5 to 2.5. Repeat CT on day 10 showed further infarct maturation without evidence of hemorrhagic transformation. Warfarin was recommenced with a dose of 10 mg once daily, without Aspirin, with a target of 2.5-3. Aspirin is planned for restart after reaching the target INR without hemorrhagic transformation in his follow-up scans. The patient made an excellent recovery of his neurological functions and was transferred to a rehabilitation center for further rehabilitation.
Discussion
Patients with LVAD are unique. They are at risk of both bleeding and embolic complications. Our patient had both types of complications making management quite challenging.
There is no consensus on the management of AIS in LVAD patients. Willey et al. suggested an algorithm for managing cerebrovascular events in LVAD patients based on single-center experience [5]. They suggested starting Aspirin in 24 hours if there is no hemorrhagic transformation and postponing Warfarin for seven days if the infarct is larger than half MCA territory. In the case of intracranial hemorrhage (ICH), they advised starting Aspirin in 7 days and Warfarin in 14 days if there is no increase in the ICH size [5]. Our patient had both pathologies simultaneously, with a large MCA infarct size. He was at high risk of hemorrhagic transformation. Therefore, we waited seven days without anticoagulation. We preferred to start with UFH as it has a short half-life, and its action is easily reversible with protamine sulfate. We started him on Warfarin on day 10.
The usual advice of re-liaising with the neurosurgical team or a tertiary center when GCS drops by 2 points sometimes leads to a delay in the performance of decompressive hemicraniectomy [6]. In the absence of an in- house neurosurgical unit, regular imaging in the hyperacute phase gives further objective evidence to aid discussion regarding potential transfer before the deterioration in neurological status.
Conclusion
Simultaneous brain infarction and intracranial bleeding present a challenge in LVAD patients. A closely monitored stoppage of antithrombotics and serial brain imaging can guide the need for surgical hemicraniectomy. Regular assessment of LVAD function is mandated. Antithrombotics can be carefully reintroduced under surveillance brain scanning to maintain the LVAD function.
References
-
Kilic A, Ailawadi G (2012) Left ventricular assist devices in heart failure. Expert Rev Cardiovasc Ther 10(5): 649- 656.
-
Adatya S, Bennett MK (2015) Anticoagulation management in mechanical circulatory support. J Thorac Dis 7(12): 2129-2138.
-
McDavid A, MacBrair K, Emani S, Yu L, Lee PHU, et al. (2018) Anticoagulation management following left ventricular assist device implantation is similar across all provider strategies. Interact Cardiovasc Thorac Surg 26(1): 60-65.
-
Patlolla V, Mogulla V, Denofrio D, Konstam MA, Krishnamani R (2011) Outcomes in patients with symptomatic cerebrovascular disease undergoing heart transplantation. J Am Coll Cardiol 58(10): 1036-1041.
-
Willey JZ, Demmer RT, Takayama H, Colombo PC, Lazar RM (2014) Cerebrovascular disease in the era of left ventricular assist devices with continuous flow: Risk factors, diagnosis, and treatment. J Hear Lung Transplant 33(9): 878-887.
-
Shah A, Almenawer S, Hawryluk G (2019) Timing of Decompressive Craniectomy for Ischemic Stroke and Traumatic Brain Injury: A Review. Front Neurol 10: 11.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study