Clinical Profile, Functional Capacity and Fragility of Elderly Referred to Cardiac Surgery
Introduction and objectives: Classifying elderly people with and without frailty referred to surgery can be a way to prevent, delay or even reverse the syndrome. To compare the clinical and functional profile of elderly people with and without frailty undergoing cardiac surgery. Methods: This is a cross-sectional study of an applied and comparative nature in patients over 60 years of age with advanced ischemic or valvular heart disease. Results: Frail elderly have lower hand grip strength (21.96±6.15), p=0.00; gait speed (5.44±1.53), p=0.04 and self-reported fatigue, with 7 (77.78%), p=0.00. Conclusion: Clinical variables are similar between groups. Handgrip strength, gait speed and self-reported fatigue may be more sensitive to detect frailty in the elderly. Possibly future studies with greater n bring significance to assess frailty or refer patients to prehabilitation before cardiac surgery.
Introduction
According to the World Health Organization (WHO), Brazil has more than 28 million elderly people over 60 years old. Such individuals have a high prevalence of comorbidities and heart-related disorders, with coronary artery disease (CAD) being an important predictor of mortality [1]. Elderly individuals indicated for surgery are often at high risk of postoperative complications [2, 3]. The frailty syndrome is recognized as an important predictor of adverse events in patients undergoing cardiac surgery, being considered a multifactorial syndrome that mostly affects people over 60 years old [4, 5].
The frailty syndrome is characterized by the reduction of functional capacity, muscle strength, resistance and loss of physiological reserve in the neuromuscular, metabolic and immune system, which can be prevented or treated with specific modalities such as physical exercise [6, 7]. Therefore, identifying frailty and classifying the clinical profile and functional capacity of elderly people undergoing elective cardiac surgery is the first step to prevent, delay or even reverse the syndrome in this population and possibly intervene in the preoperative period [8, 9].
Several instruments have been validated for frailty screening and functional capacity, with the Fried Frailty Phenotype (FFF) being an assessment scale, in which it was demonstrated that the presence of three or more components classifies the elderly as frail [10, 11]. As an assessment of submaximal functional capacity, the 6-minute walk test (6MWT) is considered the gold standard, demonstrating safety for the prescription of exercises in cardiac rehabilitation [12].
The aim of this study is to compare the clinical profile, functional capacity and frailty phenotype in elderly individuals indicated for coronary artery bypass grafting and/or valve replacement. To assess the preoperative frailty condition and functional capacity of these patients using the Fried Frailty Phenotype and the 6MWT, and compare results between groups.
Methodology
This is a cross-sectional study, of an applied and comparative nature, in which the clinical profile, functional capacity, handgrip strength and gait speed of elderly people over 60 years old, indicated for cardiac revascularization surgery of the (CRM) and/or valve replacement in a reference hospital in cardiology in Rio Grande do Sul, who were referred by the attending physician for screening from March 2020 to November 2021.
The clinical characteristics of the patients were collected through an initial interview and electronic medical record review. The frailty assessment was performed using the Fried Frailty Phenotype, which includes unintentional weight loss, self-reported fatigue using two questions from the CES-D Depression Scale, handgrip strength measured with a dynamometer, low level of physical activity measured by the Minnesota Leisure Time Activities Quiz and gait speed test. In addition to frailty, functional capacity was assessed using the 6MWT.
The study was approved by the research ethics committee CAAE:41978821.6.00005333 and was conducted following the principles of the current revision of the Declaration of Helsinki in its most recent version and Resolution 466/12. All participants signed an informed consent form.
Inclusion Criteria
Patients aged 60 years or older, candidates for elective CABG surgery, valve replacement or combination thereof. Elderly people who were physically capable of performing the functional cap9acity tests and who adhered to the free and informed consent form developed for the study were included.
Exclusion Criteria
Individuals diagnosed with psychiatric disorders and/ or severe cognitive deficits that affected the understanding of the proposed tests were excluded. Patients who failed the initial safety assessment with significant cardiovascular alterations (HR > 150 bpm and SBP > 160), gait speed test and 6MWT when applied, or with changes such as hypotension with postural instability, stage 2 hypertension (>160/100 mmHg), angina, syncope, bradycardia or tachycardia >150 bpm. Patients with non-cardiac surgery associated with the procedure, individuals with stroke or previous physical disability that makes walking impossible, as well as Chronic Obstructive Pulmonary Disease (Gold III and IV) were also excluded. History of ventricular arrhythmias or significant lesion of the left main coronary artery (defined by >50% lesion on coronary angiography). Patients with severe aortic valve stenosis with markers of poor prognosis (defined by aortic valve area < 0.7 cm2, maximum aortic jet velocity > 5.0 m/s, mean left ventricular/Ao gradient > 60 mmHg).
Data Collection Procedure
An initial screening was performed by accessing the list of elective surgeries, in chronological order of referral by the attending physician. Through a telephone call, the evaluation was scheduled to verify the clinical profile, frailty and functional capacity.
Fragility Assessment
Fried’s Frailty Phenotype
It includes five measurable components, such as:
- unintentional weight loss: ≥4.5 kg or ≥5% of body weight in the last year;
- self-reported fatigue using two questions from the CES-D Depression Scale;
- Decrease in grip strength measured with a dynamometer in the dominant hand and adjusted for gender and Body Mass Index (BMI);
- low level of physical activity estimated by weekly energy expenditure in kcal (Minnesota Leisure Time Activities Questionnaire) and adjusted according to gender;
- Gait speed decrease in seconds: 4.6m distance adjusted for gender and height.
The presence of one or two components would be indicative of a high risk of developing the syndrome, and three or more components of the scale in the elderly, classified as fragile [10, 13].
Hand Grip Strength
An analog device of manual Hand grip, hand hydraulic dynamometer, (Saehan brand, model SH500®) was used.
Subjects remained seated on a chair with their feet flat on the floor. The contraction of the flexor muscles of the right and left hands was measured to determine the maximum voluntary contraction (MVC). Three MVC were performed on each limb, with a 1-minute interval between each maneuver, considering reaching the highest value. Subsequently, the predicted strength values for age and gender were measured. The decrease in handgrip strength: measured using a dynamometer in the dominant upper limb. Positivity if below the 20th percentile of the population according to gender and body mass indicates muscle weakness [10, 14].
Gait Speed
The speed test consists of walking at your pace over a distance of 4.6 meters. Start before marking each series with the word “Vai”; start a stopwatch as soon as the first foot hits the ground after the initial mark; interrupt the stopwatch as soon as the first foot hits the ground after the 4.6 meter mark; repeat three times and average the sets, allowing enough time for recovery. Frailty is defined as a time greater than 6 seconds in the average of the sets, or the presence of a reduction in speed by 20% for gender and height [10].
Assessment of Functional Capacity
6 Minute Walk Test
This test evaluates the submaximal functional capacity of the patient by measuring the distance that the individual can walk quickly in a period of six minutes. The test was performed in a 30-meter-long flat corridor where blood pressure (BP), heart rate (HR), oxygen saturation (SpO2) and level of dyspnea (Borg perception of exertion scale) were monitored before and after the test. The test was interrupted when the patient presented the following symptoms: angina, dyspnea, cramps, pallor or when asked to interrupt. All tests were applied by trained professionals [12].
Statistical Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 23.0. Nominal values are presented in absolute and relative frequencies. Parametric data are presented as mean and standard deviation. To compare means, Student’s T Test was used. Statistical significance was considered p<0.05. Fisher’s test was used for independent samples. There was no violation of data normality from the Kolmogorov-Smirnov test.
Results
195 patients were listed for elective CABG surgery and/ or valve replacement. Of these, 135 met the exclusion criteria being under 60 years of age (n=34), severe aortic stenosis (n=63), severe trunk injury (n=23), severe aortic stenosis, and severe trunk injury (n= =15). Thus, 60 patients were indicated for evaluation of the study and of these listed with elective CABG (n=23), elective valve replacement (n=33), CABG and elective valve replacement (n=15), 26 patients were excluded because they had already undergone CRM (n=4), having already undergone valve replacement (n=5), not answering the phone (n=10), surgery cancellation (n=4), death before surgery (n=3). Therefore, 34 patients were contacted for evaluation, with exclusion of 9 for non- attendance, leaving 25 patients, of which 9 were classified as frail elderly and 16 as non-frail elderly (Figure 1).
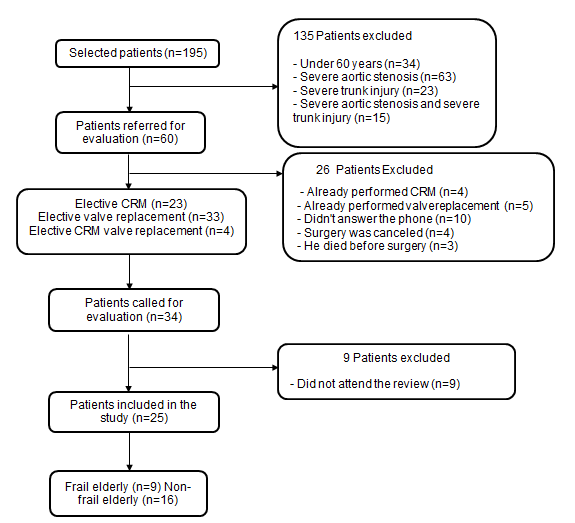
The excluded patients, 135 patients through medical records data, 26 through criteria collected by telephone call and 34 were recruited and 9 did not complete the evaluation, leaving 25 evaluated.
Table 1 presents the clinical profile of the sample. There was no difference between frail and non-frail groups, except for age according to p-values.
| Fragiles (n=9) | Not Frail (n=16) | Value of P | |
|---|---|---|---|
| Age (Years) | 75,8±8,6 | 67,5±5,9 | 0,06 |
| Masculine, n (%) | 5 (55,0) | 14 (87,5) | 0,34 |
| Weight (kg) | 71,6 (7,0) | 76,3 (4,9) | 0,61 |
| Height (meters) | 159,3 (1,7) | 166,4 (0,3) | 0,29 |
| IMC (Kg/m2) | 27,9 (4,5) | 27,3 (3,9) | 0,85 |
| AMI prior, n (%) | 4 (44,0) | 8 (50,0) | 0,67 |
| FE preserved, n (%) | 7 (77,0) | 14 (87,5) | 0,30 |
| Smoking Historic, n (%) | 3 (33,0) | 11 (68,8) | 0,14 |
| Alcoholism, n (%) | 1 (11,0) | 1 (6,0) | 1,00 |
| Comorbidities, n (%) | |||
| Diabetes Mellitus | 3 (33,0) | 7 (43,0) | 0,40 |
| Dyslipidemia | 8 (88,9) | 10 (62,5) | 0,36 |
| Hypertension | 8 (88,9) | 12 (75,0) | 0,14 |
| Depression | 1 (11,0) | 2 (12,5) | 1,00 |
Table 1: Clinical profile of the sample.
Results are presented as mean and standard deviation, absolute numbers and percentages. Kilograms were measured in kilograms and body mass index (BMI) in kilograms per square meter; (AMI) acute myocardial infarction and (EF) ejection fraction.
Fried’s Frailty Phenotype showed lower handgrip strength, lower gait speed, and self-reported fatigue in the frail group compared to the non-frail group, p < 0.05 (Table 2).
| Fragiles (n=9) | Not frail (n=16) | P value | |
|---|---|---|---|
| Handgrip strength (kgf) | 22,0±6,1 | 37,4±9,1 | <0,01 |
| Gait speed (s) | 5,4±1,5 | 4,2±0,5 | 0,04 |
| Weight loss, n % | 5 (55,6) | 3 (18,7) | 0,08 |
| Self-reported fatigue, n % | 7 (77,8) | 3 (18,7) | <0,01 |
| Low Caloric Expenditure, n % | 5 (55,6) | 7 (43,8) | 0,52 |
Table 2: Frailty phenotype of the sample.
The results are presented in mean and standard deviation, absolute numbers and percentages. Results are presented as mean and standard deviation. The evaluation of functional capacity through the 6MWT, according to the results in meters of the distance covered (p=0.78) and the percentage of predicted according to weight and height (p=0.77), did not show a significant difference between groups (Table 3).
| Fragiles (n=9) | Not frail (n=16) | P value | |
|---|---|---|---|
| Travelled distance (m) | 257,7±146,0 | 275,9±165,0 | 0,78 |
| Predicted distance, % | 70,0 ±24,0 | 85,7±17,0 | 0,77 |
Table 3: Functional capacity of the sample.
Discussion
Montgomery et al, in a study carried out in Canada from 2011 to 2014, with a sample of 529 patients, through the Clinical Frailty Score, found 9.6% of frailty in adults aged 50 years and over, subject to cardiac surgery, demonstrating higher mortality (9.8%), and greater need for hospital resources [15]. In the general population, about 10% of people aged 65 years or older have the frailty syndrome; therefore, identifying the syndrome may reduce risks and adverse outcomes in the postoperative period for these individuals, as well as implement care processes to address this growing health problem [16].
Chi et al, showed in a meta-analysis that the impacts of frailty are significantly associated with increased health costs among the elderly [17]. Observed in a 2016 systematic review study conducted in Canada, where Muscedere et al identified that a quarter of Canadians over 65 years old are frail, with a significant increase in the frailty syndrome in those over 85 years old. Therefore, they concluded that as the population ages, the risk of functional decline and deterioration in the health status of the elderly population increases [16]. However, according to our results, elderly classified as frail were on average 75 years old and obtained a percentage of 44.4% being women, in which they exhibited a BMI on average of 27.9 having low diagnostic value of weight loss, low caloric expenditure and functional capacity for frail elderly compared to non-frail.
It is important to recognize how frailty affects the functionality of the elderly, as it will allow the integration of care and treatment options [16, 17]. In a 2021 systematic review, Peeler et al reviewed 19 studies being evaluated using the Fried frailty phenotype, in which the results stated that frail patients are more likely to have poor postoperative outcomes of heart surgery. Lipero, et al. in the year 2021 showed that the prevalence of frail individuals with ischemic heart disease is common. The identification of frailty in these elderly people should be considered relevant to provide individualized prevention and cardiovascular care strategies [18, 19].
In view of the present results, the frailty assessment scale using the Fried Frailty Phenotype demonstrates that handgrip strength, gait speed and self-reported fatigue may be more sensitive to detect frailty in the elderly. This evaluation demonstrates the sensitivity of the aforementioned tool in which, in a randomized controlled study carried out in 2021, by Begiené, et al. they evaluated the effect of two rehabilitation programs on gait speed in frail and non-frail elderly people with acute coronary syndrome, and ejection fraction (≥40%). The percentage of elderly people with frailty was 37.1%, which showed a higher prevalence of elderly people without frailty, still highlighting the importance of assessing the state of frailty in elderly people with ischemic heart disease [20].
Gait speed is a reliable frailty marker, validated and simple to apply, patients with lower gait speed generate worse in-hospital outcomes [21]. Lanziotti, et al. in a sample of 5,532 community-dwelling elderly, found exhaustion to be the fourth most prevalent item of the frailty phenotype, proving the link to frailty, but unable to predict adverse events. In the self-reported fatigue variable classifying the individual’s exhaustion in their daily lives, we found 77.8% of the sample. In a 2021 systematic review, researchers sought evidence of the relationship between self-reported or perceived fatigue and falls in the elderly and found that the report of tiredness is associated with the incidence of a higher risk of falls in this population [22, 23].
The literature points out that elective cardiac patients are at risk of functional loss, and the distance covered (≤300m) in the 6MWT can predict pulmonary complications in the postoperative period, such as atelectasis and longer MV time. In a study with 36 frail patients, when performing prehabilitation of cardiac surgery CRM and/ or valve replacement resulted in a significant difference in the distance covered in the 6MWT, which was shown to be associated with a reduction in the length of hospital stay and improvement in functional capacity [24]. Corroborating the present study, given the results of the assessment of functional capacity in elderly people with and without frailty through the 6MWT, there was no significant difference in meters in the distance covered. The observed data, despite not being statistically significant, demonstrated that the patients were unable to reach a minimum distance covered and percentage of the predicted minimum, which according to the literature is described as a poor functional prognosis in these patients [23, 25].
We observe that there is no evidence in the results that assessing frailty or referring patients to a prehabilitation program would help to achieve better outcomes in cardiac surgery or that patients with frailty have a worse outcome in cardiac surgery. An increase in the number of study participants becomes necessary for greater clinical evidence, however, through the inclusion and safety criteria that we use to assess the functional capacity and frailty of patients indicated for cardiac surgery, we verify that the phenotype of Fried’s frailty and the 6MWT are safe and can be a sensitive tool for evaluating this patient profile [10, 12].
Several factors may influence the difficulty of reaching this public, these being those established in the exclusion criteria, such as stage 2 hypertension (>160/100 mmHg), major lesion of the left main coronary artery (defined by >50% lesion on coronary angiography), aortic valve stenosis among others. Our data show the feasibility of screening and assessing the frailty syndrome and functional capacity, being low cost and favorable to these patients. The elderly are more prone to postoperative dysfunctions, contributing to increased morbidity and mortality and hospital costs [26].
As for the limitations of the study, the number of participants was shown to be small according to the initial list of patients. There is a need for future studies with more time to carry out screening and evaluation, and this is evident through the difficulty of tracking and recruiting such patients, such as the difficulty of transportation.
Conclusions
Handgrip strength, gait speed and self-reported fatigue may be more sensitive to detect frailty in the elderly. The assessment of functional capacity by the 6MWT was reduced in both groups, and physical intervention in these patients may be feasible. The clinical profile showed no influence on frailty by the variables analyzed, and possibly future studies with greater n bring significance to assess frailty or refer patients to a prehabilitation program would help to obtain better results in cardiac surgery.
References
-
Timóteo AT, Ramos R, Toste A, Lousinha A, Oliveira J, et al. (2011) Impact of age on treatment and outcomes after acute myocardial infarction, particularly in very elderly patients. Rev Port Cardiol 30(12): 897-903.
-
DeFilippis AP, Young R, McEvoy JW, Michos ED, Sandfort V, et al. (2016) Risk score overestimation: the impact of individual cardiovascular risk factors and preventive therapies on the performance of the American Heart Association-American College of Cardiology- Atherosclerotic Cardiovascular Disease risk score in a modern multiethnic cohort. Eur Heart J 38(8): 598-608.
-
Kamarajah SK, Bundred J, Weblin J, Tan BHL (2020) Critical appraisal on the impact of preoperative rehabilitation and outcomes after major abdominal and cardiothoracic surgery:A systematic review and meta- analysis. Surgery 167(3): 540-549.
-
Rodrigues MK, Marques A, Lobo DML, Umeda IIK, Oliveira MF (2017) Pre-Frailty Increases the Risk of Adverse Events in Older Patients Undergoing Cardiovascular Surgery. Arq Bras Cardiol 109(4): 299-306.
-
McCann M, Stamp N, Ngui A, Litton E (2019) Cardiac Prehabilitation. J Cardiothorac Vasc Anesth 33(8): 2255- 2265.
-
Zão A, Magalhães S, Santos M (2019) Frailty in cardiovascular disease: Screening tools. Rev Port Cardiol 38(2):143-158.
-
Kamarajah SK, Bundred J, Weblin J, Tan BHL (2020) Critical appraisal on the impact of preoperative rehabilitation and outcomes after major abdominal and cardiothoracic surgery: A systematic review and meta- analysis. Surgery 167(3): 540-549.
-
Rumer K, Saraswathula A, Melcher L (2016) Prehabilitation in our most frail surgical patients: are wearable fitness devices the next frontier?. Curr Opin Organ Transplant 21(2): 188-193.
-
Yau D, Wong M, Wong W (2019) PREhabilitation for improving Quality of recovery after Elective cardiac surgery (PREQUEL) study: protocol of a randomised controlled trial. BMJ Open 9(5): e027974.
-
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, et al. (2001) Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med 56(3): 146-156.
-
Silveira D, Jorge M (2000) Escala de rastreamento populacional para depressão CES-D em populações clínicas e não clínicas de adolescentes e adultos jovens. In: Gorestain C, Andrade LHSG, et al. (Eds.), Escalas de avaliação clínica em psiquiatria e farmacologia. São Paulo: Lemos Editorial 2000.
-
Keeratichananont W, Thanadetsuntorn C, Keeratichananont S (2016) Value of preoperative 6-minute walk test for predicting postoperative pulmonary complications. Ther Adv Respir Dis 10(1): 18-25.
-
Lustosa L, Pereira D, Dias R (2011) Translation and cross-cultural adaptation of the Minnesota Leisure Time Activities Questionnaire in older adults. Geriatria & Gerontologia 5(2): 57-65.
-
Massy Westropp N, Rankin W, Ahern M, Krishnan J, Hearn TC (2004) Measuring grip strength in normal adults: reference ranges and a comparison of electronic and hydraulic instruments. J Hand Surg Am 29(3): 514- 519.
-
Montgomery C, Stelfox H, Norris C, Rolfson D, Meyer S, et al. (2021) Association between preoperative frailty and outcomes among adults undergoing cardiac surgery: a prospective cohort study. CMAJ Open 9(3): 777-787.
-
Muscedere J, Andrew MK, Bagshaw SM, Estabrooks C, Hogan D, et al. (2016) Screening for Frailty in Canada’s Health Care System: A Time for Action. Can J Aging 35(3): 281-297.
-
Chi J, Chen F, Zhang J, Niu X, Tao H, et al. (2021) Impacts of frailty on health care costs among community-dwelling older adults: A meta-analysis of cohort studies. Arch Gerontol Geriatr 94: 104344.
-
Peeler A, Moser C, Gleason KT, Davidson PM (2021) Frailty as a Predictor of Postoperative Outcomes in Invasive Cardiac Surgery: A Systematic Review of Literature. J Cardiovasc Nurs 37(3): 231-247
-
Liperoti R, Vetrano DL, Palmer K, Targowski T, Cipriani MC, et al. (2021) Association between frailty and ischemic heart disease: a systematic review and meta- analysis. BMC Geriatrics 21(1): 357.
-
Beigienė A, Petruševičienė D, Barasaitė V, Kubilius R, Macijauskienė J (2021) Frailty and Different Exercise Interventions to Improve Gait Speed in Older Adults after Acute Coronary Syndrome. Medicina Kaunas 57(12): 1344.
-
Chang J, Natalie J, Nguyenhuy M, Xu R, Virk S, et al. (2022) Slow gait speed is associated with worse postoperative outcomes in cardiac surgery: A systematic review and meta-analysis. J Card Surg 37(1): 197-204.
-
Lanziotti S, Liberalesso A, Ferrioli E, Lourenço RA, Dias RC (2016) Phenotype of frailty: the influence of each item in determining frailty in community-dwelling elderly- The Fibra Study. Cien Saude Colet 21(11): 3483-3492.
-
Pana A, Sourtzi P, Kalokairinou A, Pastroudis A, Chatzopoulos ST, et al. (2021) Association between self-reported or perceived fatigue and falls among older people: A systematic review. Int J Orthop Trauma Nurs 43: 100867.
-
Waite I, Deshpande R, Baghai M, Massey T, Wendler O, et al. (2017) Home-based preoperative rehabilitation (prehab) to improve physical function and reduce hospital length of stay for frail patients undergoing coronary artery bypass graft and valve surgery. J Cardiothorac Surg 12(1): 91.
-
Kassak K, Husari A (2015) The Clinical Impact of 6-Min Walk Test Distance as a Predictor of Complications in Patients Undergoing Major Surgery. World J Surg 39(11): 2845.
-
Steinmetz C, Bjarnason Wehrens B, Baumgarten H, Walther T, Mengden T, et al. (2020) Prehabilitation in patients awaiting elective coronary artery bypass graft surgery-effects on functional capacity and quality of life: a randomized controlled trial. Clin Rehabil 34(10): 1256-1267.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study