Acute Pancreatitis Mimicking Acute STEMI Infarction
A 54-year-old male with the history of pancreatitis, arterial hypertension and diabetes was presented to cardiologist with epigastrial pain, inferior STEMI and hypotension. Initial laboratory findings were delayed because of hemolytic serum that caused administration of invasive procedures for ruling out myocardial infarction. The condition causing hypotension was necrotic pancreatitis. This case report highlights the importance of thinking of other not very likely diagnoses in patients with STEMI infarction and the importance of obtaining laboratory findings in time.
Introduction
It is known that acute pancreatitis can alter EKG. Mostly it causes nonspecific alterations like T wave inversion, sinus tachycardia, QT prolongation, intraventricular conduction disturbances and ST depression without specific regional distribution [1, 2, 3]. These alterations can cause misdiagnosis in emergency departments, and it can worsen patient’s condition if the right approach is not implemented [4]. Our aim was to demonstrate the necessity of including other not very likely diagnoses in diagnosing procedure of acute myocardial infarction and to show importance of fast laboratory findings. Here we present a case of 54 years old male with acute pancreatitis that resembles acute myocardial infarction.
Case Report
A 54-year-old man was presented to cardiologist by Emergency department doctor with crushing pain localized in epigastrium. The onset of pain was more than 24 hours ago.
The symptoms were associated with diaphoresis and fatigue. Patients cardiovascular risk included diabetes type II for 10 years arterial hypertension for 2 years and dyslipidemia. Other risk factors included acute pancreatitis 6 years ago and sangvinizing ventricular ulcus 14 years ago. He also underwent hip surgery of both left and right hips with implantation of total endoprotesis. He was nonsmoker and nondrinker.
Methods
Physical examination showed intact cardiopulmonary findings, but it showed pain in epigastrium provoked by palpation. The arterial blood pressure was 100/70 mmHg at the time of admittance. Twelve lead EKG was recorded instantly, and it showed ST elevation in leads II, III, aVF with Q in the same leads and biphasic T wave in lead V2 (Figure 1).
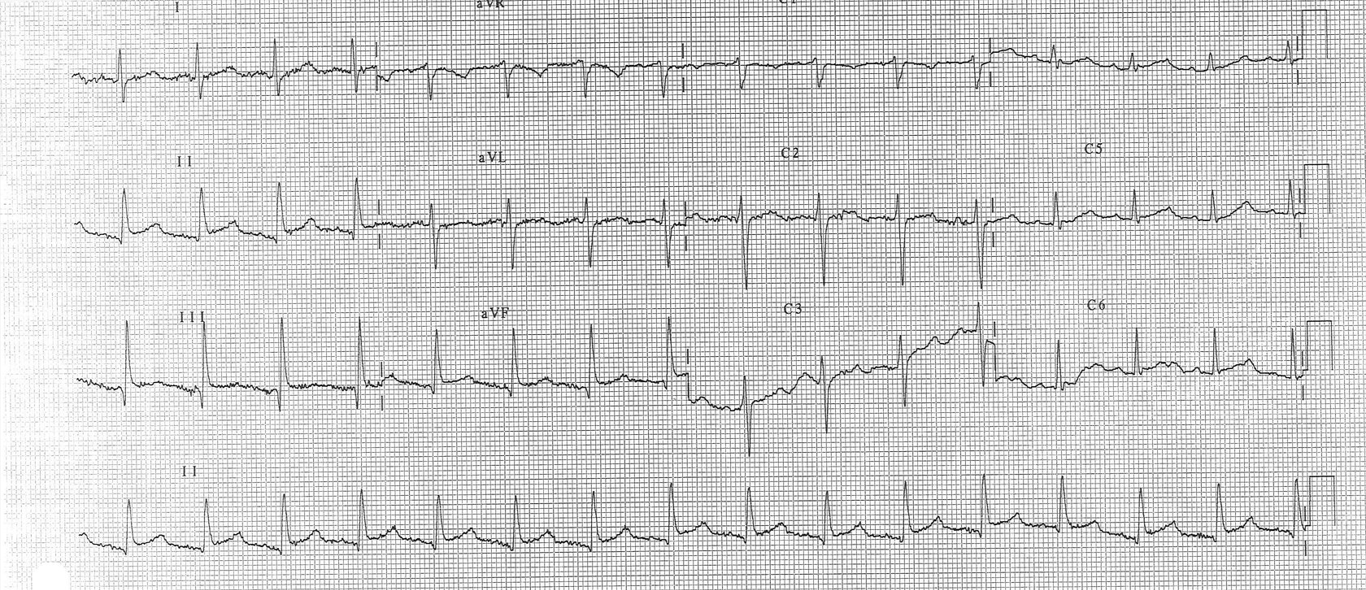
A diagnosis of acute inferior ST elevation infarction was made, and patient was transferred to the coronary care unit. The blood tests showed elevated liver enzymes and amylases in serum and in urine (serum amylase 649 U/l, urine amylase 7262 U/L). Blood count was normal at first, but after 12 hours it showed leukocytosis (12.5x 109). The laboratory findings were obtained after 3 hours since the first 2 blood samples were hemolytic.
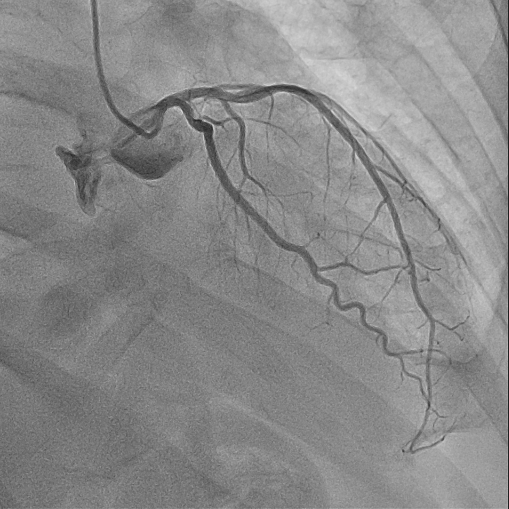
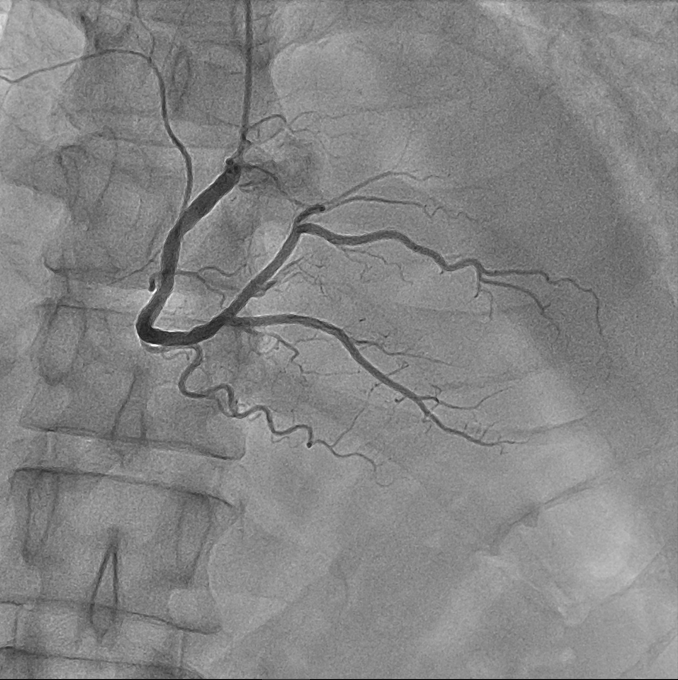
Coronary angiography was made, and it showed intact coronary arteries on the left coronary artery (Figure 2), and on the right coronary artery (Figure 3). Aortography in 3 projections was made during procedure and it showed intact aorta.
Cardiac echo was made while patient was unable to lay on his left side. That caused inability for precise cardiac measurements, but it showed normal aorta, valvular apparatus, and good systolic function of the left ventricle. Abdomen ultrasound showed hyperechogenic liver that was enlarged (16 cm) and pancreas which had inhomogeneous structure and was slightly enlarged. Ultrasound examination was difficult to perform because of patients’ condition and high concentration of air in intestine.
Native abdominal X-ray was not possible to obtain because of patients’ inability to stand. After all tests were done, patient was diagnosed acute necrotic pancreatitis and was transferred to intensive care unit where he died after 1 day. The diagnosis of acute necrotic pancreatitis was confirmed by pathologist who also excluded the diagnosis of acute myocardial infarction.
Discussion
This case is intriguing not only because it presents a scenario of acute pancreatitis mimicking acute ST elevation myocardial infarction of the inferior wall, a rather atypical presentation, but also due to the sequence of events and diagnostic challenges encountered. The patient initially sought consultation with a cardiologist primarily due to abnormal ECG results. The initial diagnosis was based on a 12-lead EKG and clinical examination, which indicated a cardiac issue. Consequently, the patient was transferred to the coronary care unit.
However, the situation took a turn for the worse as the patient became hypotensive, and the pain intensified. During episodes of severe pain, another 12-lead EKG was performed, revealing more pronounced ST elevation in leads II, III, and aVF, along with marked Q waves in the same leads. The underlying mechanism behind these ECG changes remained unclear. There were several possible explanations, including disturbances in metabolites, cardio-biliary reflex, the release of pancreatic enzymes, and even coronary artery spasms. Trypsin and other pancreatic proteolytic enzymes can directly damage the myocyte’s membrane, which can result in cellular necrosis and electrolyte imbalance [5,6.] These enzymes may also cause cardiac thrombosis by altering the characteristics of platelet adhesion [7, 8].
At this juncture, only a complete blood count was available, and it appeared normal, which is unusual for pancreatitis. To investigate further, a cardiac echo and coronary angiography were conducted, both of which showed normal coronary arteries and a cardiac echo without signs of tamponade. Despite these findings, the patient’s hypotension persisted, prompting an aortography that revealed normal aortic dimensions in three different projections. Sometimes, aortic dissection can cause dissection to spread to the left and right coronary arteries, compromising circulation. More often, this pathology is seen on the right coronary artery as an acute ischemia type of an acute STEMI infarct of inferior localization, because the dissection from the aorta enters directly into the ostium of the right coronary artery. Such a dissection can compromise the flow or lead to complete occlusion of the blood vessel with the formation of thrombotic masses in the place where the endothelium of the blood vessel is destroyed. Excess catecholamines may result in ischemia ECG abnormalities in Takotsubo cardiomyopathy [9], a side effect of pancreatitis but cardiac echo showed no traces of this pathology.
The definitive diagnosis faced challenges due to the unusual ECG presentation, normal blood count, and delayed availability of biochemistry lab results because of hemolytic serum. It was only when the biochemistry lab results arrived, indicating elevated amylase levels, in conjunction with an abdominal ultrasound and a repeat coronary angiography that the diagnosis started to become clear.
Despite heading in the right diagnostic direction, the combination of uncommon ECG findings, normal blood count, and the delayed biochemistry lab results made the diagnosis ambiguous. Regrettably, the patient’s condition continued to deteriorate, and he was transferred to the intensive care unit, where treatment involved dopamine and metronidazole. Unfortunately, the patient died within one day.
Fortunately, in this case, the duration of pain exceeded 24 hours, which ruled out the use of fibrinolytic therapy, a treatment that could potentially worsen the patient’s condition and is generally contraindicated in cases of acute pancreatitis. In conclusion, this case highlights the critical importance of obtaining early and comprehensive laboratory findings, as they can significantly aid in directing the diagnosis in the right direction and subsequently improving patient care.
References
-
Rubio-Tapia A, García-Leiva J, Asensio-Lafuente E, Robles- Díaz G, Vargas-Vorácková F (2005) Electrocardiographic abnormalities in patients with acute pancreatitis. J Clin Gastroenterol 39(9): 815-818.
-
Yu AC, Riegert-Johnson DL (2003) A case of acute pancreatitis presenting with electrocardiographic signs of acute myocardial infarction. Pancreatology 3(6): 515- 517.
-
Makaryus AN, Adedeji O, Ali SK (2008) Acute pancreatitis presenting as acute inferior wall ST-segment elevations on electrocardiography. Am J Emerg Med 26(6): 734.e1- 4.
-
White HD, Van de Werf FJ (1998) Thrombolysis for acute myocardial infarction. Circulation 97(6): 1632-1646.
-
Ro TK, Lang RM, Ward RP (2004) Acute pancreatitis mimicking myocardial infarction: evaluation with myocardial contrast echocardiography. J Am Soc Echocardiogr 17(4): 387-390.
-
Manning GW, Hall GE, Banting FG (1937) Vagus stimulation and the production of myocardial damage. Can Med Assoc J 37(4): 314-318.
-
Morrison LM, Swulim WA (1940) Role of the gastrointestinal tract in production of cardiac symptoms. Experimental and clinical observation. J Am Med Assoc 114(3): 217-223.
-
Cheezum MK, Willis SL, Duffy SP, Moawad FJ, Horwhat JD, et al. (2010) Broken pancreas, broken heart. Am J Gastroenterol 105(1): 237-238.
-
Rajani R, Przedlacka A, Saha M, de Belder A (2010) Pancreatitis and the broken heart. Eur J Emerg Med 17(1): 27-29.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study