Cardiac Tamponade in Idiopathic Capillary Leak Syndrome: Philippines’ First
Background: Clarkson’s disease, more known as idiopathic systemic capillary leak syndrome (SCLS) is a rare condition characterized by hypotensive episodes due to capillary hyperpermeability, which may be manifested by fluid accumulation in any organ or potential space, causing range of complications: respiratory failure (from pulmonary edema or pleural effusion), mesenteric hypoperfusion (from hepatic congestion and severe intestinal edema), compartment syndrome and rhabdomyolysis, and even shock from hypovolemia or cardiac tamponade. Very few cases of cardiac tamponade have been reported and certainly a serious and life-threatening complication. Case Summary: A 44-year-old female, reported to have intermittent episodes of angioedema aggravated by menstruation and infection, came in due to persistent hypotension. Patient presented with flu-like symptoms and tested positive for COVID – 19 infection. Initial laboratories revealed hemoconcentration, slightly elevated creatinine and hypoalbuminemia. Electrolytes and urinalysis were normal. 2D echocardiography showed large pericardial effusion with right atrial and ventricular collapse suggestive of cardiac tamponade, hence patient underwent emergency pericardial windowing. Initial chest X-ray was normal but repeat study showed pleural effusion on the 4th day of admission which was drained surgically. Additional diagnostic tests revealed negative for hepatitis, Mycoplasmal and Epstein-Barr virus. Direct and indirect Coomb’s test were also negative and Lupus panel was unremarkable. Serum free light chain panel showed suspicious for low level monotypic serum free lambda light chains (based only on the free light ratio). Immunopathology results showed no overt evidence of monoclonal bands. Protein electrophoresis pattern showed decreased albumin fraction and increased alpha, beta, and gamma fractions. C1 inhibitor was slightly elevated while serum tryptase was within normal values. Patient was managed as a case of idiopathic systemic capillary leak syndrome or Clarkson’s disease. Aside from judicious fluid resuscitation and vasopressors assist Methylprednisolone pulse therapy (MPPT) and intravenous immunoglobulin (IVIg) were administered. Patient was discharged with tapering doses of oral steroids and scheduled monthly IV immunoglobulin infusion. Conclusion: Cardiac tamponade, an uncommon yet severe and life-threatening complication of systemic capillary leak syndrome (SCLS) or Clarkson’s disease, requires immediate intervention. While the exact cause remains unclear, research suggests that during acute SCLS episodes and hyperinflammatory states, fluid accumulation in the pericardial space can impede ventricular filling, leading to hemodynamic compromise.
Introduction
Idiopathic systemic capillary leak syndrome (SCLS), also known as Clarkson’s disease and spontaneous periodic edema, is a syndrome occurring in middle aged patients, and should be suspected in those with hypotension, hypoalbuminemia without albuminuria and hemoconcentration [1, 2]. The hallmark of this syndrome is the presence of fluid collection in pericardial and pleural cavities. However, there is usually a delay in diagnosis of this condition due to its rarity - which remains as the main challenge in the management of this condition, rather than its treatment. Recurrent acute pericardial and pleural effusions should raise the clinician’s index of suspicion, as these may be life threatening [1]. The pathogenesis of this condition remains unclear, but researchers believe that the involvement of cytokines, leukotrienes, complement factors and vascular endothelial growth factor (VEGF) contribute greatly to the development of this condition [2].
Cardiac tamponade is also a possible complication of SARS-COV 2 (COVID-19) infection based on case reports and is more common in middle-aged males. Those who develop ventricular failure signals a worse prognosis [3]. Case reports have shown that COVID-19 infection triggers an exaggerated systemic inflammatory response in particular subset of patients, but the exact mechanism is uncertain [4]. We present a case of cardiac tamponade in a patient with idiopathic systemic capillary leak syndrome, on top of a COVID-19 infection.
Case Presentation
A 44-year-old female with no known comorbidities presented with hypotension and diaphoresis but with no complaints of chest heaviness, dyspnea, easy fatigability or abdominal pain. Patient was initially brought to another institution wherein patient was given a total of 6 liters of normal saline and 3 liters of dextrose water. There was persistence of hypotension despite fluid resuscitation hence patient was placed on inotropic support, eventually needing the use of triple pressors. Incidentally, patient also tested positive for COVID 19 infection. 2D echocardiography showed beginning pericardial tamponade and was advised transfer hence admission to our institution.
On review of patient’s clinical history, patient has a 4-year history of episodic angioedema temporally associated with hormonal changes, present during onset of menses and during upper respiratory tract infections which would subsequently subside. There was a recurrence 10 months prior, noted after the first dose of COVID vaccination accompanied by hypotension, periorbital edema and anasarca. Patient was rushed to the hospital where in fluid resuscitation was done, with noted improvement of blood pressure. At this point, additional workups revealed pleural effusion which was resolved by diuretics and patient was discharged stable. Lupus work-up were negative. Patient eventually received second dose of COVID vaccine, and recurrence of hypotension was noted. 2D echocardiography showed pericardial effusion without tamponade. Patient was eventually sent home with Aspirin, Colchicine, and antihistamine.
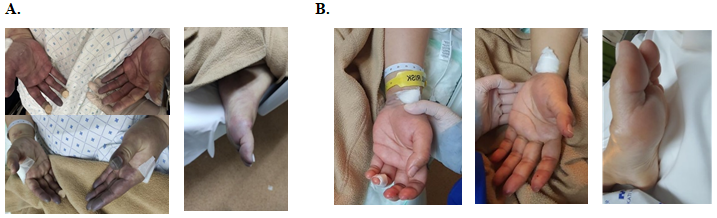
Upon arrival at the emergency room, patient was hypotensive and tachycardic. Pertinent physical examination findings revealed anasarca with positive Raynaud’s phenomenon in all extremities (Figure 1). Patient had no adventitious breath sounds, tachycardic but with regular rhythm and hearts sounds not muffled.
Complete blood count revealed hemoconcentration, with a hemoglobin of 16.9 g/dL, hematocrit of 48.8 %; white blood count was elevated at 28.21 x 103/L with normal platelet counts. Electrolytes were normal with slightly elevated Creatinine. Low serum albumin of 2.1 g/ dL was noted on admission. Urinalysis was unremarkable. Inflammatory markers showed mild elevation of LDH and normal ferritin, with low C3 at 0.05 mg/dL. ECG findings were sinus tachycardia with non-specific ST-T wave changes. Chest Xray showed clear lungs with hila and pulmonary vessels were within normal limits. Emergency 2D echocardiography showed moderate to large circumferential pericardial effusion with diastolic collapse of the right ventricle suggestive of cardiac tamponade (Figure 2). Left ventricular (LV) systolic function was normal and no LV segmental wall motion abnormalities with ejection fraction of 55% (Biplane Simpson’s). She underwent an emergency pericardial windowing and drainage. Operative findings include 400 ml of serous turbid pericardial fluid with no bacterial or fungal growth on cultures. Pericardial fluid studies showed elevated RBC (1,591,200/uL) and elevated WBC (4,140/uL) with segmenter predominance. Wide spectrum antibiotics were started to cover for possible infection. Histopathology result of pericardial tissue showed benign fragment of fibrocollagenous to fibroadipose tissue with mild chronic inflammation. Post-operatively, patient was stable with decreasing pressor requirements and with noted resolution of tachycardia and Raynaud’s phenomenon (Figure 2).
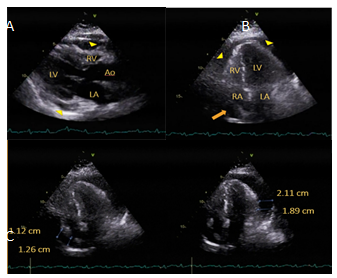
Figure 2: 2D Echocardiography. A. Parasternal long axis (PLAX) view showing pericardial effusion (arrowheads) with right ventricular diastolic collapse consistent with cardiac tamponade. B&C. Apical 4-Chamber (A4C) views showing circumferential pericardial effusion (arrowheads) with corresponding measurements, largest being 2.11 cm. There was note of right atrial systolic collapse consistent with cardiac tamponade (arrow).
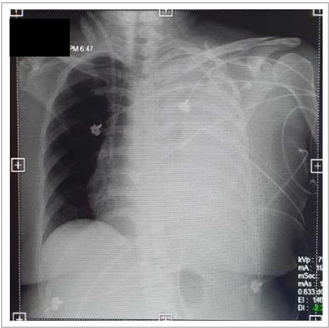
On the fourth hospital day, repeat blood counts showed sudden drop in hemoglobin (5.6 x g/dL), with a total of 850 ml of bloody output per chest tube. Chest Xray revealed opacification of left lung fields compatible with pleural effusion (Figure 3). Patient underwent mediastinal exploration, evacuation of hematoma, control of bleeders with findings as follows: 250ml serous fluid from pericardium, 1.5 liters of blood clot from the left chest with no bleeding from heart or left lung, oozing from chest tube site and Blake drain site. Patient was hooked to back to triple pressors (Dobutamine 7 mg/kg/min, Epinephrine 0.05 mg/kg/min, Norepinephrine 0.03 mg/kg/min) and was transfused with a total of 11 units packed red blood cells, 8 units fresh frozen plasma and 6 units platelet concentrate. Repeat inflammatory markers were elevated (Table 1).
Patient was worked up for possible causes of pleural effusion and pericardial tamponade. Hepatitis, Mycoplasmal tests, Epstein-Barr virus tests were negative. Direct and indirect Coomb’s test were negative and Lupus panel were unremarkable. Serum free light chain panel showed suspicious for low level monotypic serum free lambda light chains (based only on the free light ratio). Immunopathology showed no overt evidence of monoclonal bands. Protein electrophoresis pattern in correlation with concurrent serum immunofixation showed decreased albumin fraction and increased alpha, beta, and gamma fractions. C1 inhibitor was slightly elevated while serum tryptase was within normal values.
Methylprednisolone pulse therapy (MPPT) 1g/day once a day was started for 3 days then shifted to Hydrocortisone
100 mg/IV every 8 hours. Although clinically improving after MPPT, there was persistent decline in hemoglobin. Intravenous Immunoglobulin (IVIg) was initiated at 1g/ kg/day for 2 days. Repeat inflammatory markers were beginning to normalize (Table 1). Initially, patient gained weight 72.4 kg (64.2 kg) after day 1 of IVIg but persistently decreased with intravenous diuretics throughout the course of hospitalization. Patient continuously improved and subsequently discharged with Theophylline 125 mg/tablet 1 tablet 2x a day, tapering doses of Methylprednisolone and with scheduled monthly IV immunoglobulin infusion. One week after her discharge, repeat 2D echocardiography showed no signs of pericardial effusion.
| Day 1 | Day 3 | Day 6 | Day 11 | Day 14 (Pre-MPPT) | Day 19 (Post-MPPT) | |
|---|---|---|---|---|---|---|
| CRP(mg/L) | 12.96 | 17.35 | 53.45 | 39.01 | 1.04 | |
| D-dimer (ng/mL FEU) | 2230 | 2660 | 4410 | |||
| ESR (mm/hr) | 15 | 114 | 44 | |||
| LDH (U/L) | 1255.01 | 925.78 | 417.17 | 395.83 | ||
| Ferritin (ng/mL) | 1850.82 | 789.6 | 666.26 |
Table 1: Trends of inflammatory markers. Note the decrease in trend after MPPT. FEU, fibrinogen equivalent unit.
Discussion
Clarkson’s disease is a rare disorder that may present as distributive shock with swelling of the extremities and fluid accumulation around the heart and lungs [5]. Albumin may be decreased secondary to fluid extravasation from the tissues.
According to a systematic review done in China last 2016, patient would manifest with hypotension, edema, and previous flu-like illness [6]. Hyperinflammatory states such as surgery and infection can aggravate SCLS. Laboratory findings include hemoconcentration since blood becomes more concentrated due to loss of fluid. There is also notable plasma leakage, exhibited by hypoalbuminemia. Diagnosis may be difficult due to rarity of the condition, and one must have a high index of suspicion. Misdiagnosis can lead to fatal death.
The Mayo Clinic (2010) reviewed the records of patients with SCLS from 1981 to 2008. The median age of diagnosis was 44 years old. Out of the 25 patients, 56% of the patients presented with flu like symptoms at the onset of the disease. Two of the patients presented with tamponade, requiring pericardial windowing. Notable laboratory test for all patients with SCLS was the elevated hematocrit (median
19.8 g/dl) and hypoalbuminemia (albumin 1.9 g/dl) during the acute attack [2].
Treatment strategies are based on clinical experience and case reports, due to the lack of guidelines for the management of such disease entities. A case study in United Kingdom reported a 51-year-old female managed as a case of capillary leak syndrome due to progressive dyspnea and repeated readmissions due to recurrent pleural and pericardial effusion.1 Patient was treated successfully with Methylprednisolone 1g intravenously for 2 days then switched to oral prednisone 40 mg/tablet 1 tablet once a day. Patient was on monthly IV immunoglobulin (1 mg/kg) for 3 months and has remained hemodynamically stable with no hospital readmission. On follow-up after 3 months, there were still signs of global pericardial effusion but without cardiac tamponade. She was started on a tumor necrosis factor alpha inhibitor, Etanercept, given through 50 mg subcutaneous injections once a week, to prevent disease recurrence. No recurrence was observed over follow-up 7 months after. Similarly, in another report done in 2021 by Knox DB, et al. [7], a COVID positive 48-year-old asthmatic female diagnosed with systemic capillary leak syndrome had hypotension and pericardial effusion with impending cardiac tamponade. The patient was given IVIG, pressors, continuous renal replacement therapy as well as Remdesivir which improved her symptoms. On follow up, the study mentioned that the patient’s multi-organ dysfunction has now resolved.
Conclusion
Cardiac tamponade is a very rare but serious and life- threatening complication of systemic capillary leak syndrome (SCLS) or Clarkson’s disease and warrants emergent intervention. Due to marked plasma shifts secondary to hypoalbuminemia, hemoconcentration follows. The increase in capillary permeability can result in generalized edema or pleural effusion or in recurrent pericardial effusion and rarely, cardiac tamponade. The pathogenesis behind the condition is not yet fully elucidated. However, like our patient, few studies have shown that pericardial space is a potential hiatus for fluid accumulation resulting in reduced ventricular filling and subsequently hemodynamic compromise in times of hyperinflammatory state in an acute attack of SCLS.
References
-
Khan HR, Khan S, Srikanth A, Smith WHT (2020) A case report of capillary leak syndrome with recurrent pericardial and pleural effusions. European Heart Journal - Case Reports 4(2): 15.
-
Kapoor P, Greipp PT, Schaefer EW, Mandrekar SJ, Kamal AH, et al. (2010) Idiopathic Systemic Capillary Leak Syndrome (Clarkson’s Disease): The Mayo Clinic Experience. Mayo Clinic Proceedings 85(10): 905-912.
-
Hakmi H, Sohail A, Brathwaite C, Ray B, Abrol S (2020) Cardiac tamponade in COVID‐19 patients: Management and outcomes. Journal of Cardiac Surgery 35(11): 3183- 3190.
-
Dabbagh MF, Aurora L, D’Souza P, Weinmann AJ, Bhargava P, et al. (2020) Cardiac Tamponade Secondary to COVID-19. JACC: Case Reports 2(9): 1326-1330.
-
Mullane R, Langewisch E, Florescu M, Plumb T (2019) Chronic systemic capillary leak syndrome treatment with intravenous immune globulin: Case report and review of the literature. Clin Nephrol 91(1): 59-63.
-
Eo TS, Chun KJ, Hong SJ, Kim JY, Lee IR, et al. (2018) Clinical Presentation, Management, and Prognostic Factors of Idiopathic Systemic Capillary Leak Syndrome: A Systematic Review. J Allergy Clin Immunol Pract 6(2): 609-618.
-
Knox DB, Lee V, Leither L, Brown SM (2021) New-Onset Systemic Capillary Leak Syndrome in an Adult Patient with COVID-19. Case reports in critical care 2021: 8098942.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study