Factors Related With Pneumonia among Children with Left-To- Right Shunt Congenital Heart Disease
Background: Infection is one of the major morbidities in congenital heart disease (CHD), especially pneumonia. Pneumonia in CHD has been known to increase overall morbidity and mortality. Early detection of pneumonia risk factors would help decrease the need for hospitalization, increase doctors’ awareness, and improve outcomes. Objective: To identify pneumonia’s incidence and risk factors in children with left-to-right shunt CHD. Method: This is a retrospective cohort study based on medical records of children aged 3 – 60 months hospitalized with diagnosis of any left-to-right shunt CHD with or without pneumonia in Cipto Mangunkusumo National Referral Hospital, Jakarta, in 2015-2019. Data of patients with CHD and pneumonia were retrieved from medical records based on ICD-10 codes. Patient’s clinical profiles were tested as possible risk factors for pneumonia: sex, age, birth weight, parental education, socioeconomic status, number of people in the house, nutritional status, type of heart defect, heart defect size, and immunization status. Bivariate analysis of parameters was done using the Chi square test. Parameters with a p-value less than 0.05 are included to multiple logistic regression test. Results: There were 333 subjects with left-to-right shunt CHD and 167 (50.2%) had pneumonia. The most common CHD type in pneumonia was ventricular septal defect (41.9%). The defect size was significantly related to pneumonia incidence (p=0.001). Risk factors identified to affect the occurrence of pneumonia in left-to-right shunt CHD were malnutrition [OR 5.152 (95% CI 2.363 – 11.234)], incomplete immunization [OR 9.689 (95% CI 4.322 – 21.721)], low socioeconomic status [OR 4.724 (95% CI 2.003 – 11.138)], and large defect [OR 5.463 (95% CI 1.949 – 15.307)]. Conclusion: The incidence of pneumonia in left-to-right shunt CHD was 50.2%, mostly in ventricular septal defects. Nutritional status, immunization status, socioeconomic status, and defect size were significant risk factors for pneumonia in children with left-to-right shunt CHD.
Introduction
Congenital heart disease (CHD) is defined as a structural abnormality of heart or great vessels present at birth, accounting for 28% of all congenital abnormalities [1, 2]. The incidence of CHD is approximately 6-10 cases per 1,000 live births, with significant symptoms found in 50% of cases [3]. The majority of heart issues that occurred in childhood are congenital disorders, with 30% of all heart malformations require intervention in the first year of life [2]. There are three categories of CHD: left-to-right shunt CHD, obstructive CHD, and cyanotic CHD. In left-to-right shunt CHD, 30% are ventricular septal defects (VSD), followed by 12% of persistent ductus arteriosus (PDA), 7% of the atrial septal defect (ASD), and the 2% of atrioventricular septal defect (AVSD) [2]. Disorders due to heart defects provide a spectrum of symptoms describing the degree of abnormality, from asymptomatic to severe heart failure with growth failure, cyanosis, decreased exercise tolerance, and recurrent respiratory tract infections [3, 4, 5].
Infection is a common problem in children with left-to- right shunt CHD, especially lower respiratory tract infections [6, 7]. Recurrent infections and inadequate intake in children with CHD will lead to weight loss, stunted growth, and decreased immunity [3, 5]. Malnutrition and low immunity will further increase the risk of infection, causing a vicious cycle. Pneumonia itself could potentially increase the risk of respiratory failure and mechanical ventilation needs, increased the duration and frequency of hospital stay, also delay definitive CHD surgery [5, 6].
Several factors have been studied regarding the higher risk of acute respiratory infections in children with CHD. Among them are age, gender, nutritional status, breastfeeding, low birth weight, immunization, parental education, socioeconomic status, health insurance and facilities, and pollution [7, 8]. Early detection of significant risk factors for pneumonia in children with CHD would help to decrease the need for hospitalization, increase doctors’ awareness, and improve outcomes of CHD by administering earlier intervention.
Materials and Methods
Study Design
This is a retrospective cohort study based on medical records of pediatric patients in Cipto Mangunkusumo National Referral Hospital, Jakarta. Inclusion criteria were children aged 3-60 months hospitalized with diagnosis of any left-to-right shunt CHD with or without pneumonia from year 2015-2019. The data were retrieved from hospital medical records with the following ICD-10 codes: Q21.0 ventricular septal defect, Q21.1 atrial septal defect, Q21.2 atrioventricular septal defect, Q25.0 patent ductus arteriosus, and J18 pneumonia. Patients with history of chronic pulmonary disease, prolonged perinatal use of oxygen therapy, and heart surgery were excluded. Sampling was done with purposive sampling method.
Operational Definition and Data Collection
Left-to-right CHD diagnosed from echocardiography by experienced pediatric cardiologist. Community- acquired pneumonia diagnosed from the prediction rule for community acquired pneumonia diagnosis as the clinical presentation. Fever, cough, rapid breathing with or without chest retraction was used. Chest x-ray was used to confirm supporting examination. Hospitalization due to pneumonia was excluded as sample if there the patient had been admitted for more than two days in the 90 days prior to the current admission to exclude hospital-associated pneumonia. There was no available data of causative organism of the pneumonia.
Patient’s characteristics and clinical profiles were extracted from medical records and tested as possible risk factors of pneumonia. Tested characteristics and clinical profiles were: sex, age, birth weight, parental education, socioeconomic status, number of people in the house, nutritional status, type of heart defect, heart defect size, and immunization status. Low birth weight was defined as birth weight less than 2,500 grams. Parental education was divided into low (graduated elementary school), moderate (graduated high school), and high (diploma or bachelor’s degree). Socioeconomic status was categorized based on Nielsen-Admosphere classification for Indonesia: high (class A: monthly income IDR 3,000,000 or more), moderate (class B and C: monthly income IDR 1,000,000 to 3,000,000), and low (class D and E: monthly income less than IDR 1,000,000). Left-to-right CHD in this study consisted of VSD, ASD, PDA, and mixed lesions. A mixed lesion was defined as two or more left-to-right CHD found in a patient. Defect size classification based on CHD type: ASD (small 3 – 6 mm, moderate 6 – 12 mm, large >12 mm), VSD (small 3 – 5 mm, moderate 5 – 10 mm, large >10 mm), and PDA (small 1 – 1.5 mm, moderate 1.5 – 3 mm, large >3 mm). Nutritional status was based on weight-for-height z-score plotted into WHO growth curve: severely wasted (below -3 SD), wasted (-3 to -2 SD), normal (-2 to + 2 SD), overweight/obese (above +2 SD). Immunization status was considered complete if the child received all the immunization according to the appropriate age recommended by the Indonesian Ministry of Health.
Data Analysis
The tested characteristics and clinical profiles were presented descriptively as numbers and percentages. Bivariate analysis of tested parameters was done against the pneumonia group the and non-pneumonia group using Chi square test. The predictive ability was presented as relative risk (RR). Parameters with a p-value less than 0.05 then included the multiple logistic regression test to determine the odds ratio (OR). P value less than 0.05 is considered statistically significant. Data were analyzed using Statistical Product and Service Solutions (SPSS) for Windows version 20.0.
This research had received ethical permission from the Research Ethics Commission of Faculty of Medicine, University of Indonesia with number 140/UN2.F1/ETIK/ PPM.00.02/2020, as well as the research permit approval from the Head of Research, Cipto Mangunkusumo Hospital with official note number LB.02/2.2.1/0354/2020.
Results
Total 572 medical records were fulfilled the study criteria; 239 of them were excluded and total 333 medical records were available for analysis (Figure 1). The other medical records were not fulfilling the study criteria due to the incomplete diagnostic data regarding the diagnosis and the therapy.
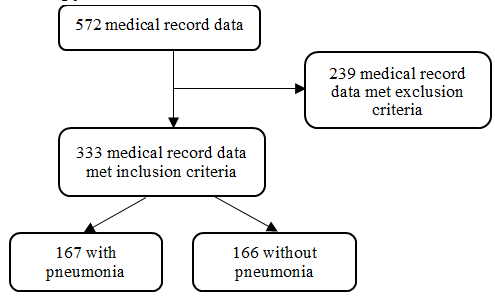
Out of 333 subjects, 52.6% were male and 47.4% were females. The median age of subjects was 12 months. Pneumonia was found in 167 patients (50.2%). The most common CHD in our study is VSD (52%), followed by PDA (18.6%), mixed (18%), and ASD (11.4%). Most of the CHD were of in moderate size (43.5%). Characteristics of subjects are presented in Table 1. In this study, pneumonia occurred approximately 6 – 18 months after diagnosis of CHD. We found an increasing incidence of pneumonia in CHD children, including 16 subjects in 2015, 26 subjects in 2016, 30 subjects in 2017, 41 subjects in 2018, and 54 subjects in 2019 (data not presented).
| Variable | Pneumonia | Without pneumonia | Total |
|---|---|---|---|
| N=167 | N=166 | N=333 | |
| Sex, n (%) | |||
| Male | 89 (50.9) | 86 (49.1) | 175 (52.6) |
| Female | 78 (49.4) | 80 (50.6) | 158 (47.4) |
| Age (months), median (min-max) | 10 (3-60) | 12 (3-60) | 12 (3-60) |
| Birth weight, n (%) | |||
| Low birth weight | 28 (57.1) | 21 (42.9) | 49 (14.7) |
| Normal | 139 (49.5) | 143 (57.1) | 284 (84.4) |
| Parental education, n (%) | |||
| Low | 12 (48.0) | 13 (52.0) | 25 (7.6) |
| Moderate | 126 (53.8) | 108 (46.2) | 234 (70.7) |
| High | 28 (38.9) | 44 (61.1) | 72 (21.8) |
| Socioeconomic status, n (%) | |||
| Low | 138 (63.0) | 81 (37.0) | 219 (65.8) |
| Moderate | 18 (26.5) | 50 (73.5) | 68 (20.4) |
| High | 11 (23.9) | 35 (76.1) | 46 (13.8) |
| Number of people in the house, n (%) | |||
| <3 people | 0 (0.0) | ||
| 3-5 people | 37 (58.7) | 26 (41.3) | 63 (18.9) |
| >5 people | 130 (48.1) | 140 (51.9) | 270 (81.1) |
| Nutritional status, n (%) | |||
| Severely wasted | 69 (77.5) | 20 (22.5) | 89 (26.7) |
| Wasted | 33 (51.6) | 31 (48.4) | 64 (19.2) |
| Normal | 65 (37.6) | 108 (62.4) | 173 (52) |
| Overweight | 0 (0.0) | 7 (100.0) | 7 (2.1) |
| Defect size, n (%) | |||
| Large | 39 (61.9) | 24 (38.1) | 63 (18.9) |
| Moderate | 74 (51.0) | 71 (49.0) | 145 (43.5) |
| Small | 19 (29.2) | 46 (70.8) | 65 (19.5) |
| Type of defect, n (%) | |||
| ASD | 25 (65.8) | 13 (34.2) | 38 (11.4) |
| VSD | 70 (40.5) | 103 (59.5) | 173 (52) |
| PDA | 37 (59.7) | 25 (40.3) | 62 (18.6) |
| Mixed | 35 (58.3) | 25 (41.7) | 60 (18) |
| Immunization status, n (%) | |||
| Incomplete | 92 (85.2) | 16 (14.8) | 108 (32.4) |
| Complete | 75 (33.3) | 150 (66.7) | 225 (67.6) |
Table 1: Characteristics of subjects.
Table 2 presents the type of CHD and its defect size. Half of ASD patients had small defects while half of VSD and PDA patients had a moderate defect. Bivariate analysis of the tested parameters showed that incidence of pneumonia was significantly associated with low socioeconomic status (relative risk [RR] 2.63, 95% CI 1.558 – 4.456, p=0.003), severely wasted (RR 2.063, 95% CI 1.652 – 2.577, p<0.001) and wasted nutritional status (RR 1.372, 95% CI 1.011 – 1.863), p=0.042), large (p<0.001), moderate (p=0.007) defects, mixed type of defect (p=0.010), ASD (RR 2.118, 95% CI 1.385 – 3.239, p=0.001), PDA (RR 1.475, 95% CI 1.122 – 1.937, p=0.005), and incomplete immunization status (RR 2.556, 95% CI 2.091 – 3.124, p<0.001). Other potential risk factors such as gender, birth weight, parental education, and the number of people in the house did not differ significantly between the two groups (Table 3).
Following bivariate analysis, five risk factors were identified with p <0.05: type of defect, defect size, nutritional status, socioeconomic status, and immunization status. These risk factors were then included to multivariate analysis. Type of defect, defect size, nutritional status, socioeconomic status, and immunization status were strongly associated with the occurrence of pneumonia in children with left-to- right shunt CHD. Table 4 describes the multivariate analysis of risk factors for pneumonia in left-to-right shunt CHD.
| Pneumonia | Without pneumonia | Total | |
|---|---|---|---|
| Variable | N=167 | N=166 | N=333 |
| ASD | |||
| Small, n (%) | 11 (44.0) | 8 (61.5) | 19 (50.0) |
| Moderate, n (%) | 10 (40.0) | 2 (15.4) | 12 (31.6) |
| Large, n (%) | 4 (16.0) | 3 (23.1) | 7 (18.4) |
| VSD | |||
| Small, n (%) | 8 (11.4) | 35 (34.0) | 43 (24.9) |
| Moderate, n (%) | 45 (64.3) | 53 (51.5) | 98 (56.6) |
| Large, n (%) | 17 (24.3) | 15 (14.6) | 32 (18.5) |
| PDA | |||
| Small, n (%) | 0 (0.0) | 3 (12.0) | 3 (4.8) |
| Moderate, n (%) | 19 (51.4) | 16 (64.0) | 35 (56.5) |
| Large, n (%) | 18 (48.6) | 6 (24.0) | 24 (38.7) |
| Mixed, n (%) | 35 (58.3) | 25 (41.7) | 60 (100) |
Table 2: Type and defect size of left-to-right shunt congenital heart diseases.
| Pneumonia | Without pneumonia | Risk Ratio (95% Confidence Interval) | P value | |
|---|---|---|---|---|
| Variable | N=167 | N=166 | ||
| Sex, n (%) | ||||
| Male | 89 (50.9) | 86 (49.1) | 1.030 (0.831-1.277) | 0.786 |
| Female | 78 (49.4) | 80 (50.6) | ||
| Age (months), median (min-max)* | 10 (3-60) | 12 (3-60) | - | 0.004* |
| Birth weight, n (%) | ||||
| Low birth weight | 28 (57.1) | 21 (42.9) | 1.167 (0.891-1.529) | 0.261 |
| Normal – overweight | 139 (49.5) | 143 (57.1) | ||
| Parental education, n (%) | ||||
| Low | 12 (48.0) | 13 (52.0) | 1.234 (0.7484-2.035) | 0.409 |
| Moderate | 126 (53.8) | 108 (46.2) | 1.384 (1.012-1.893) | 0.041 |
| High | 28 (38.9) | 44 (61.1) | ||
| Socioeconomic status, n (%) | ||||
| Low | 138 (63.0) | 81 (37.0) | 2.63 (1.558-4.456) | 0.003 |
| Moderate | 18 (26.5) | 50 (73.5) | 1.107 (0.577-2.121) | 0.759 |
| High | 11 (23.9) | 35 (76.1) | ||
| Number of people in the house, n (%) | ||||
| >5 people | 130 (48.1) | 140 (51.9) | 1.220 (0.958-1.552) | 0.13 |
| 3-5 people | 37 (58.7) | 26 (41.3) | ||
| <3 people | 0 (0.0) | 0 (0.0) | ||
| Nutritional status, n (%) | ||||
| Severely wasted | 69 (77.5) | 20 (22.5) | 2.063 (1.652-2.577) | <0.001 |
| Wasted | 33 (51.6) | 31 (48.4) | 1.372 (1.011-1.863) | 0.042 |
| Overweight | 0 (0.0) | 7 (100.0) | 0.166 (0.011-2.447) | 0.166 |
| Normal | 65 (37.6) | 108 (62.4) | ||
| Defect size, n (%) | ||||
| Large | 39 (61.9) | 24 (38.1) | 2.118 (1.385-3.239) | <0.001 |
| Moderate | 74 (51.0) | 71 (49.0) | 1.745 (1.158-2.632) | 0.007 |
| Small | 19 (29.2) | 46 (70.8) | ||
| Type of defect, n (%) | ||||
| Mixed | 35 (58.3) | 25 (41.7) | 1.442 (1.089-1.907) | 0.01 |
| ASD | 25 (65.8) | 13 (34.2) | 1.626 (1.214-2.177) | 0.001 |
| PDA | 37 (59.7) | 25 (40.3) | 1.475 (1.122-1.937) | 0.005 |
| VSD | 70 (40.5) | 103 (59.5) | ||
| Immunization Status, n (%) | ||||
| Incomplete | 92 (85.2) | 16 (14.8) | 2.556 (2.091-3.124) | <0.001 |
| Complete | 75 (33.3) | 150 (66.7) |
Table 3: Bivariate analysis for risk factors of left-to-right shunt congenital heart diseases.
| Odds Ratio (95% Confidence Interval) | P value | |
|---|---|---|
| Type of defect | ||
| Mixed | 2.060 (1.135-3.740) | 0.018 |
| ASD | 3.816 (1.160-12.556) | 0.028 |
| PDA | 3.685 (1.335-10.169) | 0.012 |
| Nutritional status | ||
| Severely wasted | 5.152 (2.363-11.234) | <0.001 |
| Wasted | 3.032 (1.174-7.827) | 0.022 |
| Immunization status | ||
| Incomplete | 9.689 (4.322-21.721) | <0.001 |
| Socioeconomic status | ||
| Low | 4.724 (2.003-11.138) | <0.001 |
| Moderate | 3.936 (1.432-11.138) | <0.001 |
| Defect size | ||
| Large | 5.463 (1.949-15.307) | 0.001 |
| Moderate | 2.107 (0.978-4.540) | 0.057 |
Table 4: Multivariate analysis of risk factors for pneumonia in left-to-right shunt CHD.
Discussion
Incidence of Pneumonia in Left-to-right Shunt CHD
Recurrent infection is a common problem in CHD patients. Some risk factors were associated with the incidence of infection in children with CHD; age, gender, nutrition, number of families, parental education, parental occupation, socioeconomic status, and environment. The loop between infection and malnutrition clearly has a negative impact on the growth of children with CHD. CHD patients that suffered from acute infections such as respiratory infections would experience anorexia, malabsorption, and metabolic disorders. Anorexia and shortness of breath can cause feeding problems in children. Inadequate food consumption will lead to weight loss, stunted growth, and decreased immunity.
The incidence of pneumonia in left-to-right shunt CHD was 167 subjects (50.2%), with the most common types of VSD (41.9%) and moderate defect size (56.6%). Based on this data, it can be concluded that the incidence of pneumonia in left-to-right shunt CHD was quite high. Khalil A, et al. [9] supported the results of this study that children with left-to-right shunt CHD experienced episodes of acute respiratory infection per year of 4.94 (SD 2.54) times, which was statistically significant compared to cyanotic CHD 2.41 (SD 1.89; p=0.01). Acute respiratory infection episodes in left-to-right shunt CHD were higher and more significant at 5.08 (SD 2.55). Another study was Sadoh WE, et al. [10] which reported that out of 131 children with CHD, pneumonia was confirmed in 121 children (92.4%).
A cross-sectional study conducted by Indra R, et al. [11] revealed that episodes of acute respiratory infection frequently develop more than 6 times per year in CHD group of 30 people (51.7%) rather than the control group of 12 people (20.7%). Meanwhile, Wilar R, et al. [3] reported episodes of acute respiratory infection in left-to-right shunt CHD were 2-7 times more common.
Prevalence of Cardiac Anatomical Abnormalities
The anatomical or structural defects in left-to-right shunt CHD are VSD, PDA, ASD, and AVSD. VSD is the most common type of CHD, approximately around 30% of all CHD. ASD abnormalities are found in 8-13% of all CHD, and PDA is around 6-11% of all CHD. The most common anatomical defects in this study were VSD (52.0%), followed by PDA (18.6%), and ASD (11.4%). In this study, there were also combined anatomical defects such as ASD and PDA, ASD and VSD, as well as VSD and PDA, and CAVSD (18.0%). In the combined group, there were 10 patients diagnosed with CAVSD, eight patients suffering from pneumonia, and two patients without pneumonia. The results of this study are similar to the research by Sharmin LS, et al. [12] on the profile of CHD in teaching hospitals in India. This study also found VSD as the most common CHD disorder, approximately 42.6%, followed by ASD 14.8%, and PDA 7.8%. In this study, the highest proportion of CHD with pneumonia was VSD (41.9%), followed by PDA (22.2%) and combined anatomical defects (21%) and ASD (15%). The results of this study are in line with the study by Sadoh, et al. that explained that VSD was the most often non-cyanotic CHD that occurs with pneumonia with approximately 50%. Another study by Owayed AF, et al. [13] also found that 72.2% of non-cyanotic CHD was presented with pneumonia.
Prevalence of Cardiac Defects Size
The defect size with pulmonary and systemic vascular resistance determines the degree of left-to-right shunt CHD.
An increase in blood flow to the lungs will trigger edema due to fluid accumulation in the lungs. This condition will be a trigger factor for respiratory tract infections, one of the most frequent complications is pneumonia.
In this study, we found that there were large defects (18.9%), medium defects (43.5%), and small defects (19.5%). In VSD with pneumonia, the most common defect size was moderate (64.3%), while in PDA with pneumonia, the most common defect size was moderate (51.4%). Moreover, for ASD with pneumonia, the most common defect size was small (44.0%). These results are in accordance with a previous study, which found that VSD associated with pneumonia would frequently occur in moderate to large defects (85.71%), and only (14.21%) with small defects. Meanwhile, PDA associated with pneumonia frequently occurs in moderate size defects [10].
Half of ASD patients had small defects; half of VSD and PDA patients had a moderate defect. The incidence of pneumonia with large VSD and PDA is much higher than the incidence in moderate or small VSD and PDA. Recurrent pneumonia has a more robust association with the size of the defect and shunt and heart failure due to the more evident findings on pediatric patients with higher defect sizes. For example, the higher pulmonary vascular markings and cardiomegaly in children with higher defects. Features of both conditions do co-exist when CHD and pneumonia occur together which may further compound the situation. Thus, it may be difficult to identify children with underlying CHD who present with pneumonia clinically. In this study however, the presence of murmurs (which were mostly systolic) and CCF were pointers to the presence of underlying CHD. These features could be used clinically in identifying children with possible underling CHD in children with pneumonia. On the other hand, smaller defect might not show evident clinical findings.
Also, small congenital heart disease is likely self-limited to age with little or no hemodynamic consequences. Findings regarding the VSD may be incidental during the physical or radiologic examination.
Risk factors for Pneumonia in Left-to-right Shunt CHD
Factors associated with increased risk of pneumonia in left-to-right shunt CHD were also identified in this study. Knowing the risk factors for pneumonia in left-to-right shunt CHD is important in daily clinical practice; therefore, interventions can be immediately carried out to improve the clinical outcome of patients with left-to-right shunt CHD. This study was conducted at the age range of 3-60 months, considering the incidence of acute respiratory infection is more frequent at the age of less than 5 years. We consider 3 months of age as the lowest age range because lung resistance starts to fall after birth until 3 months of age, therefore, shunt symptoms begin to appear at that age. The highest age distribution was in the age group of less than 24 months with a median of 10 months. The Duppenthaler A, et al. [14] study showed that CHD children had a high risk of developing respiratory syncytial virus (RSV) infection, especially in the first year of life.
This study found that economic status, nutritional status, defect size, and immunization status was related to the risk of pneumonia in left-to-right shunt CHD. Whereas gender, birth weight, and the number of people in the house were not statistically significant. The type of defect in this study does not have a statistically significant difference in the ASD group (p =0.018), PDA (p =0.012), and mixed (p =0.018). These results are in accordance with the study by Shah GS, et al. [15], that there was no difference in the type of defect against the incidence of acute respiratory infection in the non-cyanotic CHD group, with VSD (58.3%) as the most common defect in non-cyanotic CHD.
Low socioeconomic status was associated with the risk of developing pneumonia in left-to-right shunt CHD by 4.7 times compared to moderate and high socioeconomic status. These results are consistent with the study by Cohen S [16], which states that children of low socioeconomic status have a higher risk of developing infections, especially respiratory infections (p <0.03). A study by Rahman MM, et al. [17] stated that the risk of experiencing acute respiratory infection was 3.3 times higher in children with low socioeconomic status (p <0.001). This is probably related to poor sanitation, crowded environment, malnutrition, and lack of access to vaccination commonly found in the low socioeconomic family.
In this study, malnutrition status was associated with the risk of pneumonia occurring in left-to-right shunt CHD by 5.1 times compared to underweight and normal nutrition status. These results are in accordance with the study by Sjarif DR, et al. [18] that found the prevalence of malnutrition in CHD children (cyanotic and non-cyanotic) was 54.2% in non- cyanotic CHD. Research by Indra et al11 found a significant difference between the nutritional status in CHD and non- CHD patients (p <0.01).
Large defect size was associated with the risk of developing pneumonia in left-to-right shunt CHD by 5.4 times compared to the size of the medium and small defects. The size of the defect is associated with an increase in blood flow in the lungs. Sari NK, et al. [19] reported a significant association between the size of the defect, flow ratio (Qp/ Qs), and the frequency of acute respiratory infection. This conclusion is also supported by the research by Healy F, et al.
[20], which explained that left-to-right shunts would increase pulmonary blood flow, causing water retention in the lungs (pulmonary edema). Kimball TR, et al. [21] investigated the association of contractility symptoms and the size of the defect in children with VSD. This study found defect size of more than 0.5 cm (the defect size area compared to the body surface area was more than 1.8 cm/m2). This condition is an early symptom of cardiac contractility disorders in children with VSD, characterized by pulmonary congestion that leads to respiratory problems.
In the mixed defects such as ASD and PDA, the risk of developing pneumonia did not differ significantly from VSD. This is also in line with the study by Owayed AF, et al. [13], which stated that 72.2% of non-cyanotic CHD would have pneumonia. In this study, the risk for developing pneumonia in ASD was 3.8 times, due to the smaller sample size, but the incidence of pneumonia was higher (65.8%) compared to other groups.
In this study, incomplete immunization status was associated with the risk of developing pneumonia in left- to-right shunt CHD by 9.6 times compared to complete immunization status. Children who have not received immunizations are more susceptible to pneumonia. Immunization is a way to prevent infectious diseases because the child’s immune system is not yet fully developed. Although not specific to the pneumococcal conjugate vaccine, this study showed that complete basic immunization is important in preventing pneumonia. This may be related to the use of adjuvants in vaccines, which are substances added to vaccines to stimulate and enhance the magnitude and durability of the immune response. In some cases, adjuvants can help increase the immune response to certain subtypes of a given pathogen. Most importantly, adjuvants may also increase the immune system in high-risk populations [22]. The results of this study are in line with those reported by Monita O, et al. [23] at Dr. M. Djamil Padang in January 2010–December 2012, concluding that 34.8% of children with pneumonia had incomplete immunization status. This result is also consistent with the study by Annah I, et al. [24] which stated that incomplete immunization status as a risk factor for pneumonia in children aged 6-59 months, with a risk of 2.39 times is greater than children with complete immunization status. Another study by Estrada J [25] also showed that immunization prophylaxis in children with CHD is quite effective in preventing acute respiratory infection caused by influenza, pneumococcus, and RSV.
In conclusion, there are 50.2% of the cases revolving pneumonia in left-to-right shunt CHD in our hospital, mostly found in ventricular septal defect. Nutritional status, immunization status, socioeconomic status, and septal defect size are significant risk factors of pneumonia in children with left-to-right shunt CHD. However, this study was conducted at the tertiary referral center. Hence, the severity and other characteristics of left to right shunt congenital heart disease could not be traced. Also, this study is based on secondary data so the more needed data regarding the occurrence and the frequency of severity of the acute respiratory illness after the repair of CHD could not be traced.
Also, the small numbers of ASD-caused inferences unreliable. However, we hope that this study could be a starting point for more comprehensive future studies regarding pneumonia in pediatric patients with CHD.
Acknowledgments
We would like to thank the participating authors in the Department of Pediatrics, University of Indonesia Jakarta, and the research groups for the comprehensive data collection.
Funding
The authors received no specific grants from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declare no competing of interests in the subject matter or materials discussed in this manuscript.
References
-
Reller MD, Strickland MJ, Colarusso TF, Mahle WT, Correa A (2008) Prevalance of congenital heart defects in metropolitan Atlanta 1998-2005. J Pediatr 153(6): 807-813.
-
Linde D, Konings EEM, Slanger MA, Witsenburg M, Helbing WA, et al. (2011) Birth prevalence of congenital heart disease worldwide: a systematic review and meta- analysis. J Am Coll Cardiol 58(21): 2241-2247.
-
Wilar R, Wantania JM (2006) Beberapa faktor yang berhubungan dengan episode infeksi saluran pernapasan akut pada anak dengan penyakit jantung bawaan. Sari Pediatri 8(2): 154-158.
-
Tulloh RM (2018) Cardiac disorders. In: Lissauer T, Caroll W (Ed.), Illustrated Textbook of Paediatrics, Elsevier, pp: 320-343.
-
Sastroasmoro S, Sampurno SI (1994) History and physical examination. In: Sastroasmoro S, Madiyono B (Ed.), Textbook of Pediatric Cardiology, Indonesian Pediatrician Association, pp: 1-26.
-
Wheeler DS, St. Louis JD, Dent CL (2009) Congenital heart disease left-to-right shunt lesions. In: Wheeler DS, St. Louis JD, et al. (Eds.), Cardiovascular Pediatric Critical Illness and Injury, Springer, pp: 85-90.
-
Sahan YO, Kilicoglu E, Tutar ZU (2018) Evaluation of children with congenital heart disease hospitalize with diagnosis of lower respiratory tract infection. J Pediatr Res 5(1): 32-36.
-
Wantania JM, Naning R, Wahani A (2008) Epidemiology of acute respiratory infections. In: Rahajoe NN, Supriyatno B, et al. (Eds.), Children’s Respirology Textbook. 1st (Edn.), IDAI Publishing Agency, pp: 268-276.
-
Khalil A, Trehan R, Tiwari A, Malik R, Arora R (1994) Immunological profile in congenital heart disease. Indian Pediatr 31(3): 295-300.
-
Sadoh WE, Osarogiagbon WO (2013) Underlying congenital heart disease in Nigerian children with pneumonia. African Health Sciences 13(3): 607-612.
-
Indra R, Tobing TC, Siregar AD, Siregar AA, Hamid ED, et al. (1998) Nutritional status in children with congenital heart disease: prevalence and its associated factors. Paediatr Indones 38(1-2): 38-46.
-
Sharmin LS, Haque MA, Bari MI, Ali MA (2008) Pattern of clinical profile of congenital heart disease in teaching hospital. TAJ 21(1): 58-62.
-
Owayed AF, Campbell DM, Wang EE (2000) Underlying disease of recurrent pneumonia in children. Arch Pediatr Adolesc Med 154(2): 190-194.
-
Duppenthaler A, Amman RA, Hrisoho MG (2004) Low incidence of respiratory syncytial virus hospitalisations in hemodynamically significant congenital heart disease. Arch Dis Child 89(10): 961-965.
-
Shah GS, Singh MK, Pandey TR, Kalakheti BK, Bhandari GP (2008) Incidence of congenital heart disease in tertiary care hospital. Medical Journal 6(1): 33-36.
-
Cohen S (1999) Social status and suspensibility to respiratory infection. Annals N Y Acad Sci 896: 246-253.
-
Rahman MM, Syahidullah M (2001) Risk factor for acute respiratory infection among the slum infant of Dhaka City. Bangladesh Med Res Counc Bull 27(2): 55-62.
-
Sjarif DR, Anggriawan SL, Putra ST, Djer MM (2011) Anthropometric profile of children with congenital heart disease. Med J Indones 20(1): 40-45.
-
Sari NK, Anindita S, Kosim MS (2014) Hubungan antara besarnya defek septum ventrikel dengan fungsi paru. Sari Pediatri 16(3): 189-194.
-
Healy F, Hanna BD, Zinman R (2012) Pulmonary complications of congenital heart disease. Paediatric Respiratory Reviews 13(1): 10-15.
-
Kimball TR, Daniels SR, Meyer RA, Hannon DW, Khoury P, et al. (1991) Relation of symptoms to contractility and defect size in infants with ventricular septal defect. Am J Cardiol 67(13): 1097-1102.
-
Nathalie G, Moncef S (2004) New Adjuvants. In: Ciro AQ (Ed.), Vaccines: Preventing Disease & Protecting Health. Pan American Health Organization, pp: 263-272.
-
Monita O, Finny FY, Yuniar L (2015) Profile of community pneumonia patients in the pediatric department of RSUP DR. M. Djamil Padang, West Sumatra. Andalas Health Journal 4: 218-226.
-
Annah I, Nawi R, Ansar J (2015) Faktor risiko kejadian pneumonia anak umur 6-59 bulan di RSUD Salewangan Maros Tahun 2012. Jurnal Kesehatan Andalas 4: 1-5.
-
Estrada J (2017) Immunization of the pediatric patient with congenital heart disease: A systematized review with the integrative methodology. Rev Mex Enf Cardiol 25: 31-38.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study