Case Report: Perimyocarditis in the Post-Partum Period
Perimyocarditis refers to an acute inflammation of the pericardium and the underlying myocardium. Following a viral infection is its most common etiology, with reported cases associated with COVID-19 infection. Perimyocarditis in pregnancy is rare and much so this case with symptoms of palpitation and dyspnea presenting two weeks post-partum.
Case
A 42-year-old female who delivered her 1st child through caesarian delivery for breech in labor is currently on her 4th week post postpartum. She had a history of gestational hypertension in the third trimester and was prescribed Methyldopa. She also has a history of mild COVID infection occurring twice, 1 year prior and 3 years prior. She completed two doses COVID vaccination with a viral vector vaccine and an mRNA booster vaccine [1, 2].
Two weeks before admission, the patient experienced cold sweats, dyspnea, and easy fatigability. She had no other associated symptoms such as cough, colds, fever, or weight loss.
Four days before admission, her symptoms persisted and she consulted with her physician. Initial diagnostic results were done showing a normal Troponin I, an elevated D-Dimer (550 ng/ml) and an elevated NT-ProBNP (5026 pg/mL). Persistent dyspnea on minimal exertion prompted admission.
At the emergency room she was coherent, comfortable, and not in distress. She had dyspnea on minimal exertion, but with no reported chest pain. Blood pressure was 120/80, heart rate was 113 beats per minute, and O2 sat of 95% at room air. The heart rhythm was regular, with point of maximal impulse at the 6TH left ICS anterior axillary line, no heaves, lifts or thrills, no audible murmurs. There was noted bilateral fine basal rales. The rest of the physical examination findings were unremarkable. The patient’s chest radiography showed mild accentuation of pulmonary vasculature, suggesting pulmonary congestion.
Primary consideration at this time was heart failure secondary to postpartum cardiomyopathy. 2D Echocardiogram revealed a dilated left ventricle, eccentric left ventricular hypertrophy with severe global hypokinesia with reduced ejection fraction of 28% by Simpson’s. There was also note of mild pulmonary hypertension and grade 1 left ventricular diastolic dysfunction with normal left ventricular filling pressure. Compared to a 2D echocardiogram done 2018, left ventricular ejection fraction decreased from 71% to 28% (Figure 1). Patient had a 24-hour holter examination done revealing infrequent premature atrial depolarization and few multifocal premature ventricular depolarization in singles, with transient shift to complete left bundle branch block pattern which spontaneously reverts back to a narrow QRS complex.
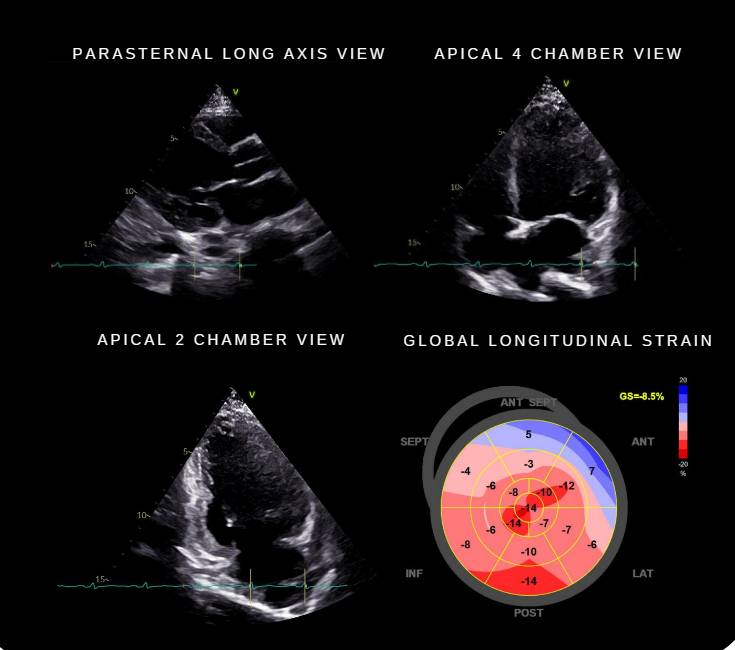
Figure 1: 2D Echocardiography: Dilated left ventricle. Eccentric left ventricular hypertrophy with severe global hypokinesia. Reduced left ventricular ejection fraction of 28% by Simpson’s. Abnormal average global longitudinal strain. (bottom right image). Normal left and right atrial diameter. Normal right ventricular dimension with adequate systolic function. Mild pulmonary hypertension Compared with previous echo three years prior: Left ventricular ejection fraction decreased from 71% to 28%.
Patient was treated with guideline-directed medical therapy for heart failure which included the following: angiotensin receptor-neprilysin inhibitor, angiotensin II receptor blocker, a beta blocker, SGLT-2 inhibitor and a mineralocorticoid receptor antagonist.
Patient underwent a Cardiac MRI with gadolinium contrast which revealed myocardial edema involving the basal to mid inferior septum, basal to apical inferior, basal to mid inferolateral, basal to mid anterolateral, and apical lateral segments. There was linear mid-wall enhancement involving the basal to apical septum, basal to apical inferior, basal to mid inferolateral, and apical lateral segments. There was pericardial enhancement with normal pericardial thickness. Findings were compatible with acute to subacute perimyocarditis (Figure 2).
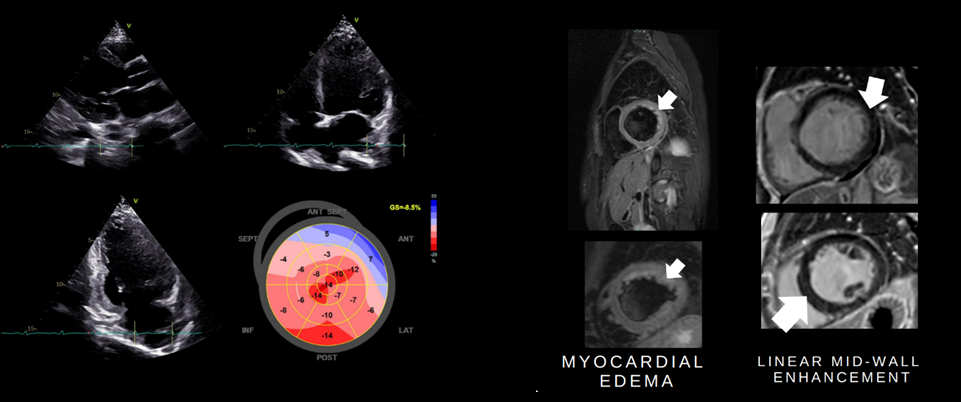
Figure 2: Cardiac MRI with Gadolinium Contrast: Findings suggestive of acute to subacute perimyocarditis. Myocardial edema involving the basal to mid inferior septum, basal to apical inferior, basal to mid inferolateral, basal to mid anterolateral, and apical lateral segments (left). Linear mid-wall enhancement involving the basal to apical septum, basal to apical inferior, basal to mid inferolateral, and apical lateral segments (right). Normal pericardial thickness with pericardial enhancement.
Medications were continued and a repeat 2D echo was done 3 months after revealing an improved left ventricular ejection fraction from 28% to 49% by Simpson’s with improvement of the contractility from severe global hypokinesia to mild hypokinesia.
Discussion
A history of COVID-19 infection or any viral illness presenting with symptoms of heart failure should prompt a thorough work-up. Peripartum cardiomyopathy was initially the primary consideration, however this is a diagnosis of exclusion and other pre-existing heart disease and other cardiomyopathies must be ruled out [3]. In this patient, a cardiovascular magnetic resonance imaging, which provides noninvasive tissue characterization of the myocardium can support the diagnosis of perimyocarditis. CMR imaging is useful when performed at the initial presentation or within two weeks of symptom onset and should be obtained prior to hospital discharge if perimyocarditis is strongly considered [4]. All patients with acute myocarditis should receive guideline-directed medical treatment for heart failure. Colchicine is used routinely in patients with pericarditis, but its role in myopericarditis is not well established [5]. Restriction of physical activity of 3 to 6 after myocarditis diagnosis is recommended [6].
Conclusion
This case highlights the importance of having a high index of suspicion for perimyocarditis in patients presenting with heart failure symptoms who have a history of COVID-19 infection. Cardiac MRI is an important diagnostic tool in the diagnosis of perimyocarditis.
References
-
Caforio ALP, Pankuweit S, Arbustini E, Basso C, Gimeno- Blanes J, et al. (2013) Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on myocardial and pericardial diseases. Eur Heart J 34(33): 2636-2648.
-
Van Driest FY, Fejzovic V, Scholte AJHA, Jukema JW, Lamb HJ (2021) COVID-19 associated perimyocarditis. Magn Reson Imaging 84: 132-134.
-
Wang WW, Wang Y (2018) Peripartum women with dyspnea in the emergency department: Is it peripartum cardiomyopathy?. Medicine (Baltimore) 97(31): e11516.
-
Adler Y, Charron P, Imazio M (2015) ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 36: 2921.
-
Ammirati E, Frigerio M, Adler ED, Basso C, Birnie DH, et al. (2020) Management of acute myocarditis and chronic inflammatory cardiomyopathy. Circulation Hear Fail 13: e007405.
-
Patriki D, Baltensperger N, Berg J, Cooper LT, Kissel CK K, et al. (2021) A Prospective Pilot Study to Identify a Myocarditis Cohort who may Safely Resume Sports Activities 3 Months after Diagnosis. J Cardiovasc Transl Res 14(4): 670-673.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study