Re-Amputations of Atherosclerotic Cause in Non-Diabetic Patients and Associated Factors
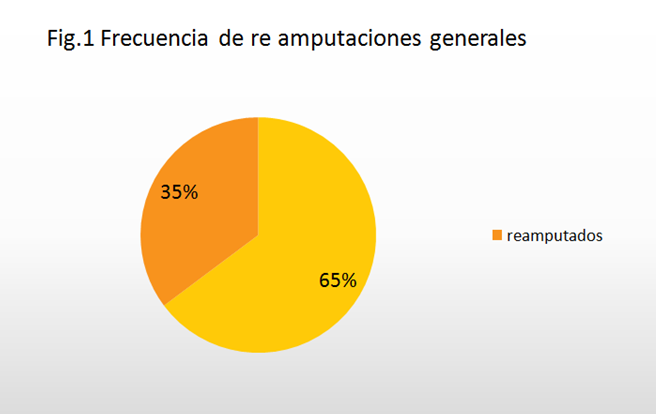
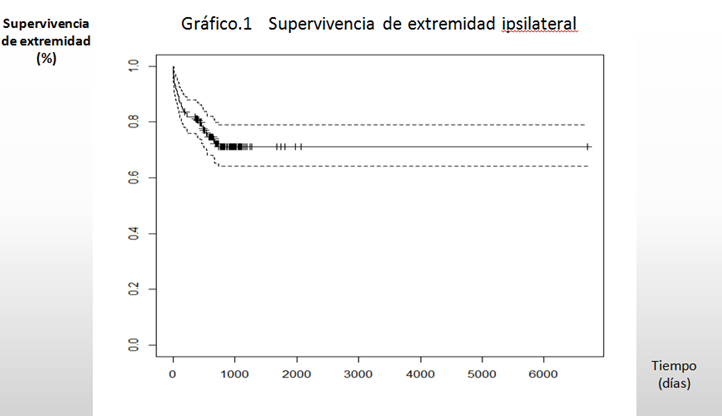
Introduction: Peripheral arterial disease together with coronary disease and cerebrovascular disease are the result of atherosclerotic disease and constitute one of the main causes of morbidity, mortality and disability. Objectives: Estimate the frequency of re amputations and identify the factors associated with it. Material and Methods: Descriptive, ambispective, observational study in all the amputee patients, who were successively reamputed in the period from September 2018 to June 2022. The main variable of the study was the frequency of reamputation. Secondary output variables: time, associated factors: (arterial hypertension, ischemic heart disease, cerebrovascular disease, chronic kidney disease), age, sex, presence of ulcer or ischemic gangrene. Results: Arterial hypertension turned out to be an associated risk factor. Ipsilateral reamputation based on the location of the original amputation demonstrated that the risk of suffering is high for toe, transmetatarsal, and infracondylar amputations; Gangrene predominated as a triggering factor for reamputees and age proved to be a determining factor for reamputation. Conclusions: The frequency of reamputation in general was 35% in amputee patients. The risk of ipsilateral reamputation was shown to be high for toe, transmetatarsal, and infracondylar amputations. Survival of the ipsi lateral limb, in 75% of the amputee patients received a re-amputation at a year and a half (548 days).
Introduction
Peripheral arterial disease, together with coronary disease and cerebrovascular disease, is atherothrombotic disease, which is why it constitutes an important health problem worldwide, and constitutes one of the main causes of morbidity, mortality and disability (amputations) in the older adults. Despite the important advances that vascular surgery has experienced in recent years, major amputations due to ischemic causes continue to be part of the surgical practice of vascular surgeons; its incidence has remained stable in recent decades and ranges between 17 and 43 amputations/100. 000 inhabitants / year [1]. In the western hemisphere, amputations of vascular origin represent 80%
of all amputations, the same as in our country, with the lower limbs corresponding to the highest frequency in a 9:1 ratio. Diabetes mellitus is the main cause of non-traumatic lower limb amputations, being responsible for approximately 50% of them; they are 15 times more frequent in patients who suffer from it; than in the general population and the risk of suffering from them increases with age: in patients > 65 years it is 7 times higher than in those under 45 years [2].
Amputation, as a surgical act, must be considered in the context of pre and postoperative care, which can be achieved if trained teams are available made up of vascular surgeons, prosthetic rehabilitators, and psychologists; gentle and a traumatic manipulation of the tissues is essential to avoid failures, generally due to poor wound healing on ischemic tissues, amputation should not be seen as a mere synonym for cutting off a limb, it should be considered as a plastic intervention and reconstructive in which it is necessary to have a great respect for the tissues, and to provide careful attention to the wound with a view to an early start if possible, of the rehabilitation. Selection of the level of amputation is often a critical decision that requires an adequate assessment of the irrigation status in that area, this decision should not be made based on a preconceived place of safety, but on an assessment of vascular tissue viability. . The choice of the level at which the amputation is to be performed depends on both local and general factors; the onset of ischemia, which can be acute, progressive, or chronic, the extent of gangrene or ulceration, the severity of the infection, the condition of adjacent areas, the degree of arterial involvement, and the intensity of pain [3] The risk factors for re-amputations are the usual ones: not giving up smoking, diabetes, diseases associated with deterioration of the general condition and advanced age [2].
Material and Methods
An ambispective, cross-sectional study was carried out in all amputee patients in the period from September 2018 to June 2022, admitted to the INACV Arteriology service, and who met the inclusion criteria. The main output variable will be the frequency of re-amputation. Which is defined: number of amputees divided or divided by the total number of re- amputees. The type of amputation was defined clinically under the following decision rule: minor amputation performed below the ankle, major amputation performed above the ankle and distributed above the knee, and amputation below the knee. A re-amputation was considered when a new amputation was performed that changed the original level and a bone cut was made from minor to major or from infra to supracondylar. It was obtained probabilistically, and the factors observed at recurrence were identified (form the variables and multivariate’s for those factors).
- Secondary variables: Time: it was considered in months based on the time that elapses from the primary amputation to the recurrence of the re-amputation.
- Associated factors: correspond to co morbidities such as arterial hypertension, ischemic heart disease, cerebrovascular disease, chronic kidney disease, dyslipidemia, etc.
- The independent or explanatory and/or confounding variables: Age, sex, was determined as referred by the patient; associated co morbidities, risk factors, presence of ulcer or ischemic gangrene, were clinically identified; blood chemistry, hematological complex, creatine, cholesterol, triglycerides, these were quantified in the ABX micro 60 hematological complex. The ankle/arm pressure index was considered normal if it was between 0.91-1.40; indeterminate greater than 1.40 (due to calcified arteries that are not very compressible), and diagnosed when the ankle/brachial index is less than 0.9 4 Kimura T, et al. [4] the steno-occlusive pattern (aortoiliac, femoropopliteal and infrapopliteal) was determined clinically-hem dynamically [5]. Previous amputation, level of amputation (supracondylar, Tran metatarsal infracondylar, others), ipsilateral and/or contra lateral reamputation, previous revascularization, surgical time, in vitro culture and antibiogram of the lesion, antibiotic therapy, hospital stay, readmission, death (cause and date).
Inclusion Criteria
Patients 18 years of age and over of both sexes who decide to participate voluntarily by signing a consent to participate and who are going to undergo a re-amputation. Patients who, due to their intellectual or psychological condition, can understand the content of the informed consent document Patients with a history of amputation.
Exclusion Criteria
Diabetic patients with a history of amputation. And/or re-amputation. Patients with a history of primary amputation of non-vascular cause and who are re-amputed. Patients who, due to their intellectual or psychological condition, cannot understand the content of the informed consent document.
Results
The clinical records of 159 patients who underwent original amputations were evaluated, distributed in the following ways; 9 finger amputations, 22 transmetatarsal amputations, 38 infracondylar amputations and finally 90 supracondylar amputations. With our research we set out to estimate the re-amputation rates in non-diabetic patients with atherosclerotic disease of the lower limbs, who underwent these procedures, discarding patients who suffered original supracondylar amputations; leaving a total of 69 patients representing 60.8% of ipsilateral and contra lateral reamputation. Survival analysis showed that patients received a re-amputation 3.1 years (1120 days) after the original amputation including ipsi and contra laterals. The median number of patients received an ipsilateral re-amputation at 1.5 years (548 days was 25%) from the original amputation, and the contra lateral one at 4.85 years (1746 days) from the original amputation. When analyzing the demographic characteristics of all the patients included in the study, we observed the distribution according to: age, sex, height, weight, as well as risk factors: arterial hypertension, ischemic heart disease, cerebrovascular disease, renal failure, the presence of (gangrene-ulcer) and laboratory; It stands out how the age has a mean of 67.5 years with a standard deviation ± 13.7 with predominance of arterial hypertension in 88% as an associated factor (Table 1) and (Figure 1).
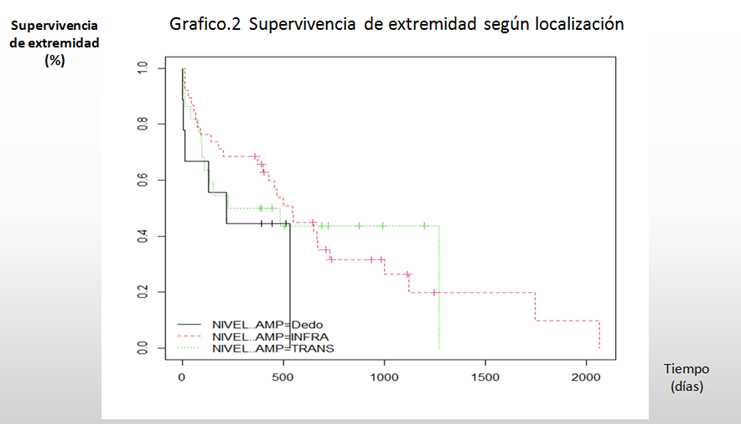
Table 2 reflects the general characteristics of the total number of patients without re-amputation 103 and with re-amputation of 56 patients; attending to the variables described in the study where the statistical analysis shows similar results for both groups. When describing the results of re-amputation according to the location of the initial amputation, we observe that the risk of re-amputation is high for toe, transmetatarsal and infracondylar amputations. The risk of suffering a contra lateral is almost similar for transmetatarsal, infracondylar, and supracondylar amputations. For finger amputations the risk is low (Table 3). Total survival values (without supracondylar) were 94,483 and 1,120 for 25%, 50%, and 75% for the 50% estimate (225-732). At 16 months, 50% of amputees are amputated. For the fingers it occurred at 7 months (220 days), for the transmetatarsal it was at 11.8 months (354 days) and for the infracondylar it was at 18 months (547 days). The median of finger reamputation were performed at 220 days (0.61 years), the transmetatarsal at 354 (0.98 years) days, the infracondylar at 547 days (1.5 years), and the supracondylar were not performed. They were observed at a high frequency, with significant differences, for ipsilateral re-amputations. The median of finger reamputation did not exist, the transmetatarsal at 1273 (3.5 years) days, the infracondylar at 1746 days (4.4 years) and the supracondylar at 1977 days (5.5 years). Without significant differences, for contra lateral reamputation. When working without supracondylar amputations. Table 4 shows the univariate factors associated with minor and infracondylar reamputation, resulting in no significant change in age, sex, arterial hypertension, ischemic heart disease, which are the trigger for reamputation; however the type of injury in 69% gangrene predominates as a triggering factor for re-amputees. In a multivariate analysis associating the level of amputation (Table 5). Age represents an associated factor that predominates in patients.
| Mean±SD, N | % | |
|---|---|---|
| Age | 67,5±13,7 | |
| M/H | 60/99 | |
| Size (cm) | 167,1±51,1 | |
| Weight (Kg) | 65,3±48,9 | |
| Arterial hypertension | 140 | 88 |
| Ischemic heart disease | 54 | 34 |
| E. Brain Vascular | 17 | 10,7 |
| Chronic renal E. | 1 | 0,6 |
| Ischemic ulcer | 81 | 50,9 |
| Gangrene | 76 | 47,8 |
| Leukocytes | 12,612±4,494 | |
| Hemoglobin | 9,8±1,73 | |
| Hematocrit | 31,7±5,7 | |
| Creatinine | 98,3±26,4 | |
| Albumin | 33,3±6,7 |
Table 1: General characteristics of patients included.
| Ipsilateral | Against laterals | |||
|---|---|---|---|---|
| Location | N | % | N | % |
| Fingers (9) | 6 | 66,7 | 0 | 0 |
| Transmetatarsal (23) | 12 | 52,2 | 1 | 4,3 |
| Infra condylar (37) | 24 | 64,9 | 4 | 10,8 |
| Supra condylar (90) | 1 | 1,1 | 9 | 10 |
Table 2: Re-amputations according to location of the initial amputation.
| Without reamputation (103) | With re-amputation (56) | |
|---|---|---|
| Age | 67±13,3 | 68,5±13,0 |
| M/H | 41/72: 0,569 | 19/37: 0,514 |
| Women in % | 36,3 | 33,9 |
| Size (cm) | 167±51,4 | 167±50,0 |
| Weight (Kg) | 65,2±36,5 | 65,6±34,8 |
| Arterial hypertension | 90 (87,4%) | 50 (89,3%) |
| Ischemic heart disease | 34 (33,0%) | 20 (35,7%) |
| E. Brain Vascular | 11 (10,7%) | 6 (10,7%) |
| Ischemic ulcer | 59 (57,3%) | 22 (39,3%) |
| Gangrene | 42 (40,8%) | 34 (60,7%) |
| Leukocytes | 12 423 | 12 960 |
| Hemoglobin | 9,8 | 9,7 |
| Hematocrit | 31,8 | 31,4 |
| Creatinine | 99 | 97 |
| Albumin | 33,2 | 33,6 |
Table 3: General characteristics and amputations.
| Without reamputation (23) | With re-amputation (46) | |
|---|---|---|
| Age | 57,6±16,8 | 69,5±15,9 |
| M/H | ||
| Women in % | 9 (40,9%) | 15 (31,9%) |
| Arterial hypertension | 19 (82,6%) | 42 (91,3%) |
| Ischemic heart disease | 6 (26,1%) | 16 (34,8%) |
| Ischemic ulcer | 12 (52,1%) | 18 (39,1%) |
| Gangrene | 9 (39,1%) | 29 (63,0%) |
Table 4: Factors associated with minor and infracondylar re-amputations.
| coeff b | s.e. | Wald | p-value | exp(b) | |
|---|---|---|---|---|---|
| Intercept | -35,86,33,757 | 4,13,88,481 | 7.51E-03 | 0,99930863 | 2.66E-12 |
| Sex | -10,01,34,329 | 0,67536502 | 21,98,30,964 | 0,13816221 | 0,3673856 |
| Age | 0,06797367 | 0,024151 | 79,21,56,966 | 0,00488489 | 10,70,33,713 |
| Arterial Hypertension | -0,2317079 | 1,05,02,151 | 0,04867715 | 0,82538133 | 0,79317778 |
| Ischemic Heart Disease | -0,17205688 | 0,67129528 | 0,06569267 | 0,79771471 | 0,84193128 |
| Smoking Habit 1. Smoker 2. Non-Smoker 3. Ex-Smoker | 10,13,40,292 | 98,75,55,729 | 1.05E-03 | 0,99918123 | 25,18,56,394 |
| Ischemic Ulcera | 22,65,03,182 | 40,19,30,343 | 3.18E-03 | 0,99955036 | 6869232471 |
| Ischemic Gangrene | 22,84,69,352 | 40,19,30,343 | 3.23E-03 | 0,99954646 | 8361763605 |
Table 5: Multivariate analysis.
Discussion
This study deals with atherosclerotic re-amputations in non-diabetic patients and associated risk factors, and in this sense it is very topical because despite continuous technological and therapeutic advances, the rate of amputations and re-amputations due to diseases Peripheral vascular disease has no tendency to decrease and, taking into account the increase in the longevity of the population, it is most likely that it will even increase. This research demonstrated the distribution of all major and minor amputations (n= 159) performed by the Arteriology service of the National Institute of Angiology and Vascular Surgery for a period of 4 years, discarding patients who suffered original supracondylar amputations, leaving them with a total of 69 patients representing 60.8% of ipsilateral and contra lateral reamputation. Shin JY, et al. [6] report 2.7% of re-amputations, which seems too low; when compared with other authors such as Oshawa and collaborators Lin JH, et al. [7] who report a re-amputation frequency above 40%, while most of the authors consulted remain between 10% and 20% respectively Littman AJ, et al. [8], Primadhi RA, et al. [9] and Reyes Rocha A [10] analyzed the frequency distribution of the amputations received by the patients included in his study, 88.8% of the amputations carried out in atherosclerotic patients were greater with a marked preponderance towards amputations above the knee relative to below knee amputations (66 vs 33%). Minor amputations in these patients were only performed in 11.1% of the patients. It is striking in the study that presents the relationships observed between amputations above the knee and amputations below the knee, both in diabetic and non-diabetic patients. There is a ratio between supra and infracondylar amputations of
2 in atherosclerotic patients and 1 in diabetic patients [2]. Vassallo IM, et al. [11] performed an analysis of all patients who received initial amputations in fiscal years 2000 and 2004 and report that below-knee amputations and above- knee amputations decreased from 1.08 to 0.87 and from 1.41 to 0.72 per 1000 and per year, respectively, which results in the supra/infra ratio, which was initially 1.31, decreasing to 0.85. In this case, we are talking about a population made up mainly of diabetic patients, and yet it is observed that the ratio is currently below unity. Libby IM, et al. [12] in Nigeria in 2016 carried out a 5-year retrospective study, in which they included 251 patients and reported a supra/infra ratio of 1.26. The mean age of the amputee population and the standard deviation are similar to the results of other authors such as Sereday M, et al. [2] who report 63.1 plus or minus 19.5 years (range 16-96 years). Marcos Garcia L, et al. [13] in their research Natural history of the patient subjected to an infracondylar amputation: analysis of survival and fitting for 2 decades, the mean age was 71.88 years. Arterial Hypertension as a cardiovascular risk factor was present in a high percentage of the studied population, which coincides with the consulted bibliography [14, 15]. Sereday M, et al. [2] in their research, observed when studying the different levels of amputation according to the provisions of the LEA Global protocol, that the most frequent amputations in diabetics were at the finger level (36.5%), followed by those above the knee (32.5%). In non-diabetics, the most frequent was above the knee (56.47%) followed by below the knee (14.7%), only one patient suffered contra lateral limb amputation in the same period. O Brien PJ, et al. [16] report a supracondylar, infracondylar, and transmetatarsal reamputation rate of 8.1%, 12.6%, and 26.4%, respectively (Figures 2,3).
Marcos García L et al. [13] When analyzing the survival of the amputations of the total 209 operated patients, 42 required a major amputation of the contra lateral lower extremity throughout the follow-up, which represents 20.1% of the total (30 infracondylar and 12 supracondylar amputations). The rate of absence of amputation in the contra lateral extremity was 88, 82 and 72% at one, 2 and 5 years in the period 1996-2005 and 86, 82 and 76% in the period 2006-2015 respectively, without finding significant differences. Sanchez Perales MC, et al. [17] in their research showed that the survival of the non-amputee patient at 20 months is 81.3% vs 55% in amputees at 60 months, 62.2% vs 35% and at 120 months 33 % vs. 15%. Patient survival after the first amputation was 15.3 plus or minus 16 in diabetics and 13.2 plus or minus 22 months in non-diabetics. Survival for the first major amputation was 14.5 plus or minus 19 and minor 14.1 plus or minus 20 months. Izumi Y, et al. [18] demonstrated that the re-amputation rate was 60% at 5 years. Long-term survival among patients with above-knee or below-knee amputations was 62% at 1 year and 29% at 5 years. Kono Y, et al. [19] observed that of the total of 116 patients studied, 57 required a re-amputation at 3 years; 45 patients (78.9%), received re-amputation within 6 months of their first amputations, 42 patients had a re-amputation once, 14 patients, 2 times and one had a re-amputation three times in 3 years. Finally, 15 patients with finger amputations were amputated at the transmetatarsal level; 24 patients receive below-knee amputation and 8 above- knee amputation. In relation to the type of injury triggering the re-amputation, gangrene predominates as a determining factor. The results coincide with authors such as Kono Y, et al. [19] who describes the presence of gangrene on physical examination, insulin-dependent diabetes, hospital stay, and level of amputation as determinant risk factors. Skoutas D, et al. [20] report age and the presence of heel injuries as determining risk factors for re-amputation. Other authors such as Stone PA, et al. [21] point out that end-stage renal disease and severe ischemia are the triggering factors. Age represents an associated factor that predominates in re- amputee patients. The results obtained in this study fully coincide with all the consulted bibliography [2, 8, 22, 23, 24].
Conclusion
- Survival analysis demonstrated that patients receive a re-amputation at 3.1 years (1120 days) from the original amputation, including ipsilateral and contra lateral.
- The risk of suffering a re-amputation of fingers, transmetatarsal and infracondylar is high depending on the location of the original amputation.
- Gangrene turned out to be a determining risk factor for re-amputation.
References
-
Fernández Travieso JC (2013) Enfermedad arterial periférica en adultos mayores. Rev CNIC Ciencias Biologicas 44(3): 1-13.
-
Sereday M, Damiano M, Lapertosa S, Cagide A, Bragagnolo JC (2009) Amputaciones de Miembros Inferiores en diabéticos y no diabéticos en el ámbito hospitalario. Diabetes Care 13(1): 9-15.
-
Schirò GR, Sessa S, Piccioli A, Maccauro G (2015) Primary amputation vs. limb salvage in mangled extremity: a systematic review of the current scoring system. BMC musculo skeletal disorders 16: 372.
-
Kimura T, Watanabe Y, Tokuoka S, Nagashima F, Ebisudani S, et al. (2019) Utility of skin perfusion pressure values with the Society for Vascular Surgery Wound, Ischemia, and foot Infection classification system. Journal of Vascular Surgery 70(4): 1309-1317.
-
Littman AJ, Tseng C-L, Timmons A (2000) Risk of ipsilateral Reamputation following an incident toe amputation among U.S. military veterans with diabetes, 2005-2016. Diabetes Care 43(5): 1033-1040.
-
Shin JY, Roh SG, Sharaf B, Lee NH (2018) Risk of major limb amputation in diabetic foot ulcer and accompanying disease: A meta-analysis. J Plats Reconstruct Aesthetic Surg 70(12): 1681-1688.
-
Lin JH, Jeon SY, Romano PS, Humphries MD (2020) Rates and timing of subsequent amputation after initial minor amputation. J Vasc Surg 72(1): 268-275.
-
Littman AJ, Tseng C-L, Timmons A, Moore K, Landry G, et al. (2020) Risk of ipsilateral Reamputation following an incident toe amputation among U.S. military veterans with diabetes, 2005-2016. Diabetes Care 43(5): 1033- 1040.
-
Primadhi RA (2021) Susceptibility factors for early Reamputation in diabetic great toe gangrene. Cur Diabetes Rev 17(1): 55-62.
-
Reyes Rocha A. Riesgo de re amputación y presión de perfusión cutánea en pacientes amputados de causa vascular. Trabajo de Terminación de Residencia para optar por el título de especialista de primer grado en Angiología y Cirugía Vascular. 2020. La Habana. Cuba.
-
Vassallo IM, Gatt A, Cassar K, Papanas N, Formosa C (2019) Healing and mortality rates following toe amputation in type 2 diabetes mellitus. Exp Clin Endocrinol Diabetes 129(6): 438-442.
-
Libby P, Bornfeldt KE, Tall AR (2016) Atherosclerosis, successes, surprises, and future challenges. Circ Res 118(4): 531-534.
-
Marcos García L, Mateos Torres E, Velascu A, Díaz Duran C, Lacambra Peñart M, et al. (2020) Natural history of the patient undergoing infracondylar amputation: analysis of survival and prostheticization over 2 decades. Cir Esp 98(7): 403-408.
-
Nerone VS, Springer KD, Woodruff DM, Atway SA (2019) Re-amputation after minor foot amputation in diabetic patients: risk factors leading to limb loss. J Foot Ankle Surg 52(2): 184-187.
-
Hasanadka R, McLafferty RB, Moore CJ, Hood DB, Ramsey DE, et al. (2011) Predictors of wound complications following major amputation for critical limb ischemia. J Vasc Surg North American Chapter 54(5): 1374-1382.
-
O Brien PJ, Cox MV, Shortell CK, Scarborough JE (2013) Risk factors for early failure of surgical amputations and analysis of 8,878 isolate lower extremity amputation procedures. J Am Coll Surg 216(4): 836-842.
-
Sánchez Perales MC (2005) Incidence and risk factors of non-traumatic lower limb amputation in hemodialysis patients. Nefrología 25(4): 399-406.
-
Izumi Y, Satterfield K, Lee S, Harkless LB (2006) Risk of Reamputation in Diabetic Patients Stratified by Limb and Level of Amputation: a 10-year observation. Diabetes Care 29(3): 566-570.
-
Kono Y, Mudder RR (2012) Identifying the incidence of and risk factors for reamputation among patient who underwent foot amputation. Ann Vasc Surg 26(8): 1120- 1126.
-
Skoutas D, Papanas N, Georgiadis GS, Zervas V, Manes C, et al. (2009) Risk factors for ipsilateral reamputation in patients with diabetic foot lesions. Int. J. Low Extreme Wounds 8(2): 69-74.
-
Stone PA, Back MR, Armstrong PA, Flaherty SK, Keeling WB, et al. (2005) Midfoot amputations expand limb salvage rates for diabetic foot infection. Ann Vasc Surg 19(6): 805-811.
-
Bueno-Barbosa BM, Monteiro RA, Sparano LF, Bareiro RFN, Costa-Passos AD, et al. (2016) Incidence and causes of lower-limb amputations in the city of Ribeirão Preto from 1985 to 2008: evaluation of the medical records from 3,274 cases. Rev Bras Epidemiol 19(2): 317-325.
-
Bunte MC, Shishehbor MH (2018) Resolving the high stakes of limb salvage with skin perfusion pressure. Vascular Medicine 23(3): 250-252.
-
Xuanliang P, Chuangang Y, Guoxian C, Huawei S, Chunmao H, et al. (2018) Skin perfusion pressure for the prediction of wound healing in critical limb ischemia: a meta-analysis. Arch Med Sci 14(3): 481-487.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study