Heart Failure and Myocarditis in a 27-Year-Old Male with Human Immunodeficiency Virus
HIV-associated cardiomyopathy is a complication of HIV infection that affects the structure and function of the heart. Early detection and diagnosis is crucial and routine cardiac workup is recommended with people living with HIV. In this report, we have a 27-year-old, Male, who identifies as gay, with a history of AIDS and has been living with HIV since 5 years from admission with a recent undetectable viral load. He presented with undocumented fever, cough and dyspnea over 7 days nonresponsive to Azithromycin. Multimodality imaging stands in the forefront of diagnosis of HIV-associated Cardiomyopathy and cardiomyopathies in general. Transthoracic 2D echocardiography or Cardiac MRI is recommended on initial evaluation among patients suspected to have the disease in order to identify its specific phenotype. Echocardiography is further recommended in monitoring the progression of the disease and response to therapy. Patient’s initial echocardiogram fulfilled the criteria for DCM with an LVEDD of 59mm and a reduced ejection fraction of 40%. Due to scheduling issues, Cardiac MRI was done 77 days after guideline-directed medical therapy for heart failure with reduced ejection fraction ARNI, beta-blockers, SGLT-2 inhibitors, and diuretics as needed. Results showed significant improvement in ejection fraction to 60%, with resolution of previously seen hypokinesia, but persistence of the LV dilatation with an LV volume index of 121 mL/m2. More importantly, post-contrast imaging on the short axis show that there are linear mid-wall enhancement indicative of non-ischemic patterns of enhancement involving the basal to mid anterior septum, basal to mid inferior septum, basal to mid inferolateral, and basal lateral segments characteristic of a post-myocarditis cause of dilated cardiomyopathy.
Introduction
HIV-associated cardiomyopathy is a complication of advanced HIV infection that can result in significant morbidity and mortality [1]. It is characterized by structural and functional abnormalities of the heart, including left ventricular systolic dysfunction, diastolic dysfunction, and dilated cardiomyopathy. HIV cardiomyopathy is thought to result from direct viral toxicity, as well as immune dysregulation and chronic inflammation associated with HIV infection [2]. While the incidence of HIV cardiomyopathy has decreased with the advent of antiretroviral therapy (ART), it remains an important cause of heart failure in people living with HIV [3].
In this case report, we present a case of HIV cardiomyopathy in a patient with advanced HIV infection although with undetectable viral load, who presented with fever and dyspnea. We discuss the diagnostic workup, including echocardiography, cardiac MRI and cardiac biomarkers, and the management of the patient’s heart failure and guideline-directed medical therapy. We also highlight the importance of routine cardiac evaluation in people living with HIV, particularly in those with advanced disease, to detect and manage cardiac complications early [4].
Case Report
This is a case of a 27-year-old, Filipino, Male who identifies as gay, presented with a 1 week history of undocumented fever and cough unresponsive to Azithromycin which was then accompanied by dyspnea. He was a known case of AIDS since 5 years ago, with lowest CD4 count of less than 200/ μL and has since been compliant with antiretrovirals with an undetectable viral load. He was seen awake, speaks in phrases, tachypneic, orthopneic with rales on both bases on auscultation and had faint opacities scattered in both lungs on chest x-ray – he was then managed as a case of Community Acquired Pneumonia – Moderate Risk vs Pneumocystis Pneumonia [5].
A high resolution CT scan of the Chest was done, revealing multilobar patches of ground glass opacities in both lungs, more extensive in the right upper and middle lobe– suggestive of an infectious process with a recommendation of correlation for possible viral pneumonia along with a minimal pericardiac effusion.
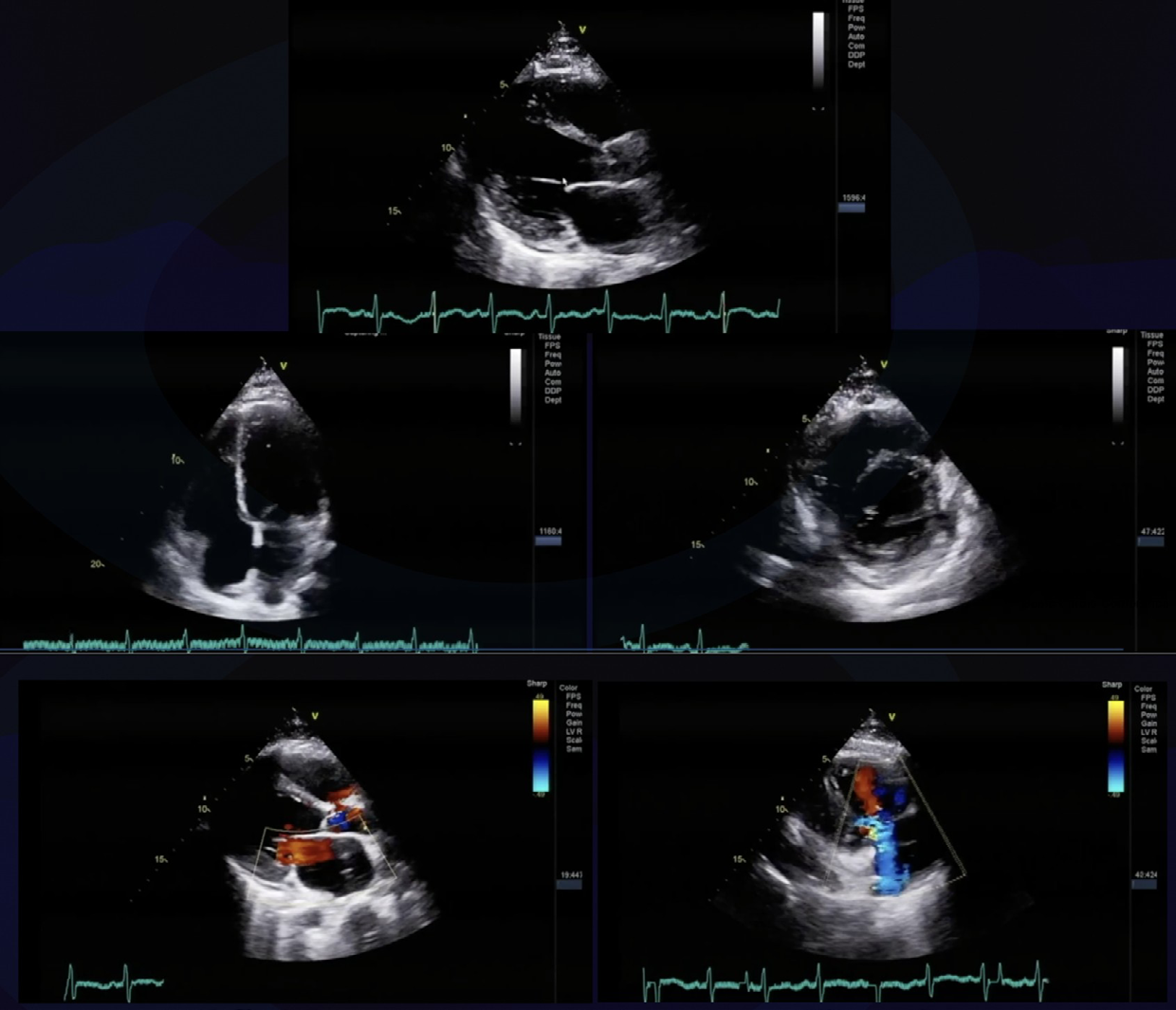
He was negative for both Pneumocystis jirovecii and Mycoplasma pneumoniae. Thyroid function test were normal as well. He had no previous cardiac work up. The initial electrocardiogram showed sinus tachycardia with non-specific ST-T wave changes. Cardiac biomarkers were done – Troponin I High Sensitivity was normal, NT-proBNP was elevated at 1690.55pg/ml. His 2D echocardiography showed trace pericardial effusion, dilated left atrium, dilated and eccentrically hypertrophied left ventricle with global hypokinesia and an ejection fraction of 42% by Simpson with a global longitudinal strain of -6.1% and moderate mitral regurgitation. He was then managed as a case of Acute Heart Failure initially with Furosemide and eventually with Sacubitril + Valsartan, Empagliflozin and Carvedilol. Patient’s symptoms improved dramatically after diuresis and was discharged after 4 days.
Delayed due to several issues, a cardiac MRI was done after seventy-seven days on his heart failure medications, it showed a dilated LV with an ejection fraction of 60%, no evidence of myocardial fatty infiltration or edema, and linear mid-wall enhancement (non-ischemic pattern) involving the basal to mid anterior septum, basal to mid inferior septum, basal to mid inferior, and basal inferolateral segments which is suggestive of Myocarditis. Since discharge, patient has been compliant with both heart failure medications and ARV. He has been well since.
Discussion
HIV prevalence in Asia is the second highest globally, with the majority of cases concentrated in high-risk populations such as men who have sex with men and people who inject drugs [6, 7, 8]. In the Philippines, HIV incidence continues to rise, with sexual transmission being the most common mode of transmission [7]. Early diagnosis and treatment are crucial in managing the disease, and regular cardiac monitoring is recommended for patients with HIV, as HIV cardiomyopathy is a potential complication of the disease [8, 9].
The diagnostic criteria for HIV cardiomyopathy are not well established, but it typically involves ruling out other causes of cardiomyopathy and demonstrating evidence of cardiac dysfunction in HIV-positive patients. The diagnosis is usually made based on clinical symptoms, such as dyspnea, fatigue, or chest pain, in combination with evidence of cardiac dysfunction on imaging studies such as echocardiography, cardiac MRI, or nuclear medicine scans. A biopsy may also be performed to confirm the diagnosis, but it is not routinely recommended due to the risk of complications [1, 10].
Several studies have reported that HIV-positive individuals are at increased risk of developing cardiovascular disease (CVD), including cardiomyopathy [11, 12]. A study conducted in China found that the prevalence of left ventricular systolic dysfunction in HIV-positive individuals was 10.5%, which was higher than that reported in the general population [13]. Similarly, a study conducted in Thailand found that the prevalence of left ventricular diastolic dysfunction in HIV-positive individuals was 16%, which was significantly higher than that reported in the general population [14]. Another study conducted in India found that the prevalence of heart failure in HIV-positive individuals was 4.4%, which was higher than that reported in the general population [15].
The advent of ART brought about a turn in Cardiovascular syndrome present in patients with HIV with Pericardial Effusion and DCM in the Pre-ART era to complications of Atherosclerosis such as MI, stroke, heart failure, atrial fibrillation and sudden cardiac death in the anti-retroviral therapy era. However, DCM still persists especially in those without access to anti-retroviral therapy or non-compliant to prescribed regimen or in patients compliant to ART [16, 17, 18].
HIV cardiomyopathy falls under the non-genetic causes of dilated cardiomyopathy, particularly due to infection causing myocarditis with its sequelae leading to DCM [19]. Diagnosis of cardiomyopathy is based on structural and functional myocardial abnormalities, not explained solely by CAD or abnormal loading conditions. The goal of requesting diagnostics in patients with suspected cardiomyopathy is to compound evidences in order to identify its specific phenotype [19].
Transthoracic 2D echocardiography has a Class Ib recommendation to evaluate LV and RV systolic and diastolic function at initial evaluation, follow-up, and monitoring of disease progression to aid risk stratification and management. Dilated cardiomyopathy is diagnosed by detecting the presence of LV dilatation through LV end-diastolic diameter of >58mm in males and >52mm in females and volume index of >≥75 mL/m2 in males and ≥62 mL/m2 in females with LV systolic dysfunction defined as <50% ejection fraction [19]. In the case, patient has dilated LV which fulfilled both criteria for DCM with end-diastolic diameter of 59 mm, coupled with depressed EF of 40% via Simpsons with global hypokinesia, a dilated LA with a volume index of 4.0cm with no visible thrombus, normal RV with decreased systolic function and trace pericardial effusion. The dilatation on the chambers also resulted to moderate regurgitant flow in the mitral and tricuspid valve.
The cornerstone in the diagnosis of DCM is multimodality to initially establish the diagnosis of cardiomyopathy and stratify it according to structural and functional parameters. In choosing the appropriate imaging technique, physicians should always consider the yield of actionable results vs. the costs, advantages, and limitations of each technique, patient safety and exposure to ionizing radiation and contrast media. At its forefront with superior cost/benefit ratio are 2D echo and cardiac MRI in risk stratification, prognostication and monitoring of disease progression [19]. Stress imaging and CT coronary angiography are used to evaluate valvular and dynamic gradients on specific CM phenotypes and to rule out myocardial ischemia. Lastly, bone scintigraphy and PET-CT are done for more targeted studies for Amyloidosis.
Another more enhanced or high resolution imaging that eliminates the factor of acoustic shadow is Cardiac MRI. It is recommended to be done when possible on initial evaluation of DCM. Especially, if 2D echo has poor image quality as it is independent of acoustic window and also non-invasive. For other etiologies of cardiomyopathy, it has the ability to characterize tissues advantageous in diagnosing ARVC, myocarditis, amyloidosis, sarcoidosis, other forms of inflammatory disease, and iron overload/ haemochromatosis. However, unlike 2D echo, it only has a class IIa recommendation in the monitoring of disease progression and risk stratification, and assessment of treatment response due to perceived costs. And thus, if ever it will be used for that purpose, it is recommended that it be done every 2-5 years depending on initial severity and clinical course. There are the characteristic findings in cardiac MRI among specific phenotypes and etiology of cardiomyopathy. Among these is the characteristic subepicardial late gadolinium enhancement post-contrast among those with post-myocarditis suspected on our patient early due to HIV [19].
The patient’s Cardiac MRI was taken after 77 days of his 2D echo while on guideline directed medical therapy of heart failure. The LV is still dilated at 121 ml/m2, but with improved systolic function of 60% from 40% and no wall motion abnormalities and a normal RV, now with adequate systolic function. On the edema sequences of short axis views from base to apex, it can be seen there were no areas of increased signal intensity or myocardial edema meaning that there is no active myocarditis. More importantly, post- contrast imaging on the short axis show that there are linear mid-wall enhancement indicative of non-ischemic patterns of enhancement involving the basal to mid anterior septum, basal to mid inferior septum, basal to mid inferolateral, and basal lateral segments characteristic of a post-myocarditis cause of dilated cardiomyopathy. Certain considerations are taken on patients undergoing cardiac MRI. But in the advent of newer technology, particularly of newer cardiac implantable devices that reduce image artifacts as well as newer imaging sequences reducing inhomogeneity, technical adjustments reduce the rate of uninterpretable studies to one in five. Furthermore, the newer linear or macrocyclic gadolinium contrast reduces the chance for nephrogenic systemic fibrosis to none with an eGFR cutoff of 30. But it is still not appropriate to use in pregnancy.
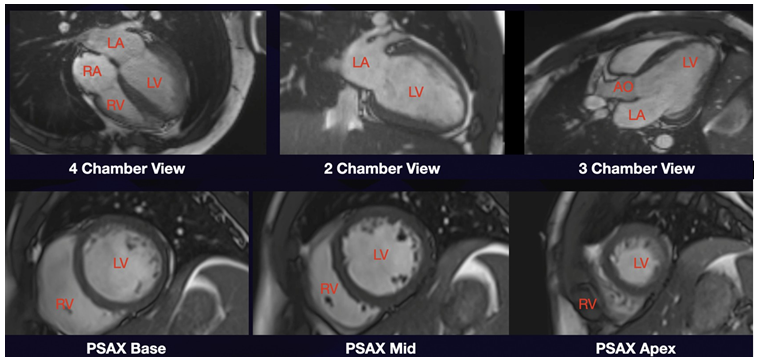
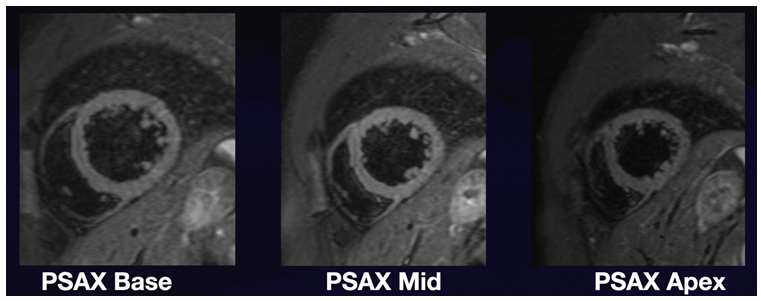
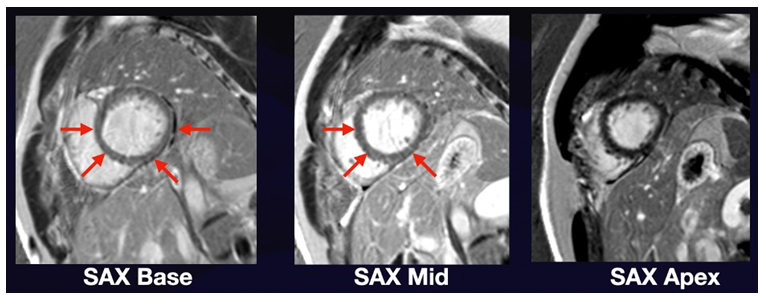
Figure 4: Short Axis Views of Post-Contrast Cardiac MRI showing Late Gadolinium Enhancement of the basal to mid anterior septum, basal to mid inferior septum, basal to mid inferolateral, and basal lateral segments In summary, the use of Multimodality Imaging - 2D echo and MRI is recommended on initial evaluation of cardiomyopathy with 2D echo superior due to its cost benefit ratio in monitoring the progression of the disease and response to therapy, provided that we get good quality images enough to infer the necessary information. And if CAD is highly considered or significantly contributing to the clinical condition then CT coronary angiography or stress imaging may be considered.
Other diagnostics recommended in cardiomyopathy are resting and ambulatory electrocardiogram and laboratory tests. ECG is an accessible test providing information that could lead to certain phenotypes of the disease and among those genotype-positive individuals on family screening, thus is recommended to be done on first clinic visit of all individuals suspected of CM. Primary goal of the lab tests is to detect extracardiac conditions that cause or exacerbate ventricular dysfunction (e.g. thyroid disease, renal dysfunction, and diabetes mellitus) and secondary organ dysfunction in patients with severe heart failure. There are the first-level (Calcium, CK, Ferritin, CBC, Liver function, NR-proBNP, Phosphate, urinalysis, renal function, serum iron thyroid function, Troponin) and second-level tests recommended among different phenotypes, with Troponin and NTproBNP at its forefront for prognostication and monitoring of disease progression. Last but not the least genetic testing/counselling is also recommended among those with confirmed or suspected inheritable cardiomyopathy. Though in the case of our patient, it is not applicable.
We are on the ART era of HIV where complications of Atherosclerosis predominate. And in the case of our patient, since he will need to resume ART therapy. And with the inherent effects of Protease Inhibitors, Non-nucleoside and nucleoside reverse transcriptase inhibitors on lipid levels on top of the natural effects of HIV on them (decreases total cholesterol, LDL, HDL but INCREASES Triglyceride), requesting for baseline lipid levels may be reasonable [18].
HIV-associated cardiomyopathy is on the other end of the spectrum in the treatment of HIV apart from the sequelae of atherosclerosis associated with ART. There are no specific guidelines for HIV-associated Heart Failure and there are no controlled trials from low-to-middle income countries addressing the most effective treatment strategy. Restoration of immune status and viral load suppression may ameliorate cardiac dysfunction as long as medications causing cardiac dysfunction are avoided. The forefront of therapy, therefore, is classifying the type of heart failure that the patient has (Heart Failure with Reduced ejection fraction), and following guideline-directed management by provision of beta blockers, ARNI, beta blockers, MRA, SGLT-2 inhibitors, and diuretics as needed [20]. This was done in conjunction with aggressive control of risk factors (hypertension, metabolic syndrome, dyslipidemia, cigarette smoking) contributing to the disease. This proved beneficial to our patient as we saw a significant improvement in the ejection fraction to 60% on Cardiac MRI. Throughout patient care, he did not meet criteria for him to implanted with an ICD (<35% EF, presence of NSVT, sudden cardiac death). Furthermore, regimens also veer into restoring and improving immune status and viral suppression to avoid outcomes of HIVAC and pericarditis. However, this comes at a cost of balancing the appropriate ART regimen in order to protect patients from the consequences of atherosclerosis and avoiding adverse drug-drug interactions.
Conclusion
In conclusion, HIV cardiomyopathy is an important complication of advanced HIV infection that can result in significant morbidity and mortality. Although there is limited data on the prevalence of HIV cardiomyopathy in Asia, studies have reported a higher incidence of heart failure in people living with HIV compared to the general population. Early cardiac monitoring is crucial in people living with HIV, particularly in those with advanced disease, to detect and manage cardiac complications early. Patients such as in this case responded well to guideline directed medical therapy for which improved his symptoms and his quality of life [21]. Therefore, routine cardiac evaluation in people living with HIV is recommended, particularly in those with advanced disease in order to prevent progression of heart failure and possibly reduce hospitalization and mortality.
References
-
Barbaro G (2005) HIV-associated cardiomyopathy etiopathogenesis and clinical aspects. Herz 30(6): 486- 492.
-
Triant VA (2013) Cardiovascular disease and HIV infection. Curr HIV/AIDS Rep 10(3): 199-206.
-
National Heart, Lung, and Blood Institute (2023) What is Cardiomyopathy?.
-
Reinsch N, Neuhaus K, Esser S (2010) Prevalence of cardiac diastolic dysfunction in HIV-infected patients: results of the HIV-HEART study. HIV Clin Trials 11(3): 156-162.
-
Boccara F (2008) Cardiovascular complications and atherosclerotic manifestations in the HIV-infected population: type, incidence and associated risk factors. AIDS 22(S3): S19-S26.
-
Joint United Nations Programme on HIV/AIDS (UNAIDS) (2021) Asia and the Pacific.
-
Philippines Department of Health (2021) HIV/AIDS & ART Registry of the Philippines.
-
United Nations Development Programme (UNDP) (2020) HIV and AIDS in Asia and the Pacific.
-
World Health Organization (WHO) (2021) HIV/AIDS in the Western Pacific Region.
-
Zhang F, Haberer JE, Wang Y, Zhao Y, Ma Y, et al. (2016) The Chinese free antiretroviral treatment program: challenges and responses. AIDS 30(6): 795-804.
-
American Heart Association (AHA) (2020) HIV infection and cardiovascular disease.
-
Mocroft A, Reiss P, Kirk O, Mussini C, Girardi E, et al. (2010) Is there evidence for an increased risk of myocardial infarction among patients with HIV/AIDS? A cohort study. European Heart Journal 31(4): 463-471.
-
Tripathi AK, Misra R, Gupta SK, Bhattacharya M, Shrivastava S (2011) HIV/AIDS-related cardiac dysfunction in a rural Indian hospital. Journal of Infection in Developing Countries 5(02): 119-124.
-
Chen Y, Han Y, Liang Y, Zhang J, Zhao S, et al. (2018) Prevalence and factors associated with left ventricular systolic dysfunction in HIV-infected individuals. Journal of Acquired Immune Deficiency Syndromes 77(4): 359- 366.
-
Kosalaraksa P, Bunupuradah T, Boettiger D, Colby D, Chokephaibulkit K, et al. (2013) Prevalence of diastolic dysfunction among HIV-infected children receiving antiretroviral therapy. AIDS 27(14): 2245-2252.
-
Sliwa K, Carrington MJ, Becker A, Thienemann F, Ntsekhe M, et al. (2012) Contribution of the human immunodeficiency virus/acquired immunodeficiency syndrome epidemic to de novo presentations of heart disease in the Heart of Soweto Study cohort. European Heart Journal 33(16): 2094-2100.
-
Aberg JA, Gallant JE, Ghanem KG, Emmanuel P, Zingman BS, et al. (2014) Primary care guidelines for the management of persons infected with human immunodeficiency virus: 2013 update by the HIV medicine Association of the Infectious Diseases Society of America. Clinical Infectious Diseases 58(1): e1-e34.
-
Hsue PY, Deeks SG, Hunt PW (2012) Immunologic basis of cardiovascular disease in HIV-infected adults. J Infect Dis 205(S3): S375-S382.
-
Libby P (2022) Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. In: 12th (Edn.), Philadelphia, PA: Elsevier.
-
Arbelo E (2023) ESC Guidelines for the Management of Cardiomyopathies. European Heart Journal pp: 1-124.
-
McDonagh TA (2021) ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal 42: 3599-3726.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study