Ectopic Supraventricular Rhythms during Exercise Electrocardiography
Three cases of the new appearance of ectopic supraventricular rhythms during exercise electrocardiography are presented. Transient decrease in the rate of the sinoatrial node or transient increase in the rate of subsidiary pacemaker are responsible. Electrocardiographic criteria for diagnosing the site of origin of supraventricular ectopic foci are discussed. The diagnostic, and prognostic significance of such a finding is not known.
Introduction
Normally, the rate of the sinus node increase progressively during exercise. Therefore, the rate of any subsidiary pacemaker never exceeds the rate of the sinoatrial node during treadmill testing. We are reporting three cases where ectopic supraventricular rhythm appeared at peak exercise or during recovery.
Case Reports
Case Number 1
A 56 years old male was evaluated for atypical chest pain. Resting supine electrocardiogram was normal (Figure 1). P wave were positive in leads I, II, III, aVF, V4R and V2 to V6 (marked as ↑) and negative in lead aVR (marked as ↓). PR interval was 0.14 seconds. Peak heart rate was 165 beats per minute. During first minute of recovery (Figure 1) patient transiently developed an atrioventricular nodal rhythm with inverted P waves in leads II, III, aVF, V4R (marked as ↑) and positive P wave in lead aVR (marked as ↓). P wave remained positive in lead V5 (marked as ↑) PR interval was short (0.10 second, marked as ∗). There were no ST-segment of T wave changes.
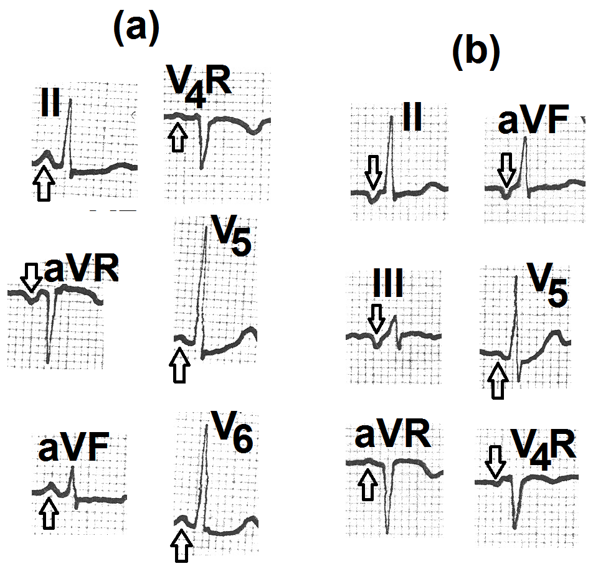
Figure 1: a: Resting supine electrocardiogram. It shows positive P waves in leads II, aVF, V4R, V5 and V6 (marked as ↑) and negative P wave in lead aVR (Marked as ↓). These findings are suggestive of normal sinus rhythm. b: Electrocardiogram recorded during the first minute of recovery. It shows the inversion of P waves in leads II, III, aVF, V4R (marked as ↓) and positive P waves in leads aVR and V5 (marked as ↑). PR interval is normal. These findings are suggestive of ectopic focus in the posteroinferior right atrium.
Case Number 2
A 48 years old male was evaluated for atypical chest pain. Resting supine electrocardiogram (Figure 2) was normal. P waves were positive in leads I, II, III, aVF, V4, V5, V6 (marked as ↑) and inverted in lead aVR (marked as ↓). PR interval was 0.14 seconds. Patient could complete the treadmill test without any symptoms, ST-segment or T wave changes. During the second minute of recovery (Figure 2), P waves became inverted in leads II, III, aVF, V3 to V6 (marked as ↓). P wave became positive in lead aVR (marked as ↑). PR interval remained 0.14 seconds.
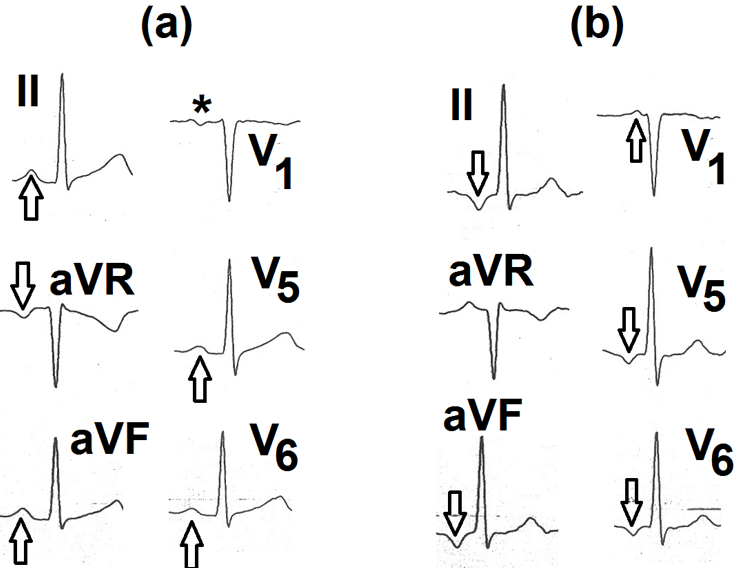
Figure 2: a: Resting supine electrocardiogram showing positive P waves in leads II, aVF, V5 and V6 (marked as ↑). P wave is inverted in lead aVR (marked as ↓) and is biphasic (+/-) in lead V1 (marked as ∗) Findings are suggestive of normal sinus rhythm. b: Electrocardiogram recorded during the second minute of recovery. It shows inverted P waves in leads II, aVF, V5 and V6 (marked as ↓). P waves are positive in leads aVR and V1 (marked as ↑). The PR interval is normal. These findings are suggestive of ectopic focus in the inferoposterior left atrium.
Case Number 3
A 53 years old male presented with chest pain on effort. He was evaluated by treadmill testing. Resting supine electrocardiogram (Figure 3) was normal. P waves were positive in leads II, III, aVF, V3, V4 ,V5, and V6 (marked as ↑) and negative in lead aVR (marked as ↓). The patient could exercise for 11:44 minutes (8.1 METs). Peak heart rate was 142 beats per minute (85% of the age-predicted maximal heart rate). Slow upsloping ST-segment depression appeared during the third stage and increased at peak exercise (Figure 3, marked as ∗). At peak exercise, P waves became inverted in leads V3, V4 and V5 (Figure 3, marked as ↓). Also, PR interval in leads V4 and V5 decreased to 0.08 second (Figure 3, marked as ∗).
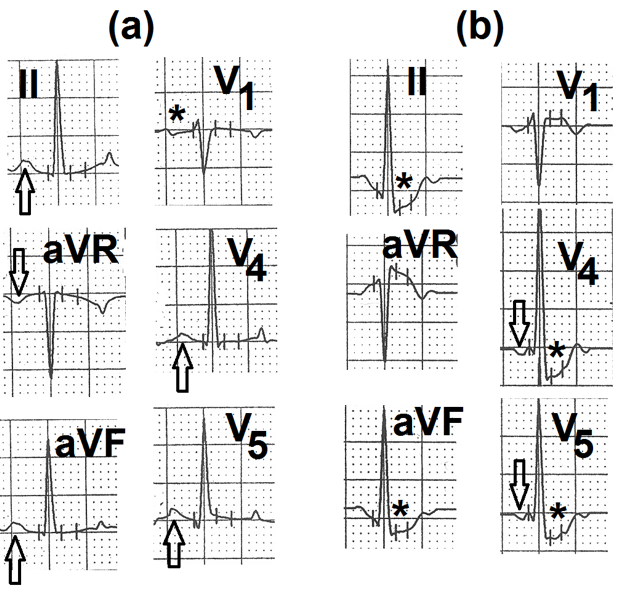
Figure 3: a: Resting supine electrocardiogram showing positive P waves in leads II, aVF, V4 and V5 (marked as ↑). P wave is inverted in lead aVR (marked as ↓) and biphasic (+/-) in lead V1 (marked as ∗) Findings are suggestive of normal sinus rhythm. b: Electrocardiogram recorded at peak exercise. P waves are inverted in leads V4 and V5 (marked as ↓). The PR interval is short. Findings are suggestive of junctional rhythm. There is slow upsloping ST-segment depression in leads II, aVF, V5 and V6 (marked as ∗).
Discussion
Normal P Wave and PR Interval
P wave is produced by depolarization of the atria. Normally, the electrical impulse arises from the sinoatrial node which is situated at the junction of the superior vena cava with the right atrium. The impulse then travels downwards and to the left via intermodal pathways to reach the atrioventricular node. The mean frontal plane vector of the atrial depolarization is, thus, directed towards the positive pole of lead II and away from the positive pole of lead aVR. P wave arising from the sinoatrial node is, therefore, positive in leads II, aVF, III and negative in lead aVR. PR interval ranges from 0.12 seconds to 0.20 seconds as the impulse faces a normal delay in conduction across the atrioventricular node [1].
Inverted P Waves in Leads II, III, aVF
- It can occur in the following situations
- Ectopic impulse arising in the low left atrium [2].
- Ectopic impulse arising in the low right atrium [3].
- Ectopic impulse arising in the vicinity of the atrioventricular node [4].
- Ectopic focus arising within the atrioventricular node [4].
- Ectopic focus arising in the coronary sinus [5].
Low atrial rhythms produce negative P waves in leads II, III, and aVF: P wave is positive in lead aVR and aVL Henckell AK, et al. [6] as the impulse traverses upwards. PR interval is normal because the impulse faces a normal delay in conduction across the atrioventricular node. Ectopic impulse arising in the vicinity of the atrioventricular node behaves like low atrial rhythms: PR interval remains normal.
Ectopic focus arising from within the atrioventricular node also produce inverted P waves in leads II, III, aVF and positive P wave in lead aVR as the impulse traverses upwards and right towards the positive pole of lead aVR. P wave remains positive or flat in leads V5 and V6 as the atrial depolarization vector remains parallel to these leads. The relation of the P wave to the QRS complex depends on the relative velocity of conduction retrogradely to the atria and antegradely to the ventricles [1]. If the retrograde conduction to atria is faster than the antegrade conduction to the ventricles, an inverted P wave appears before the QRS complex. PR interval is short (less than 0.12 seconds) because the impulse arising within the atrioventricular node partly overcomes the normal delay in conduction across the atrioventricular node. If the time taken for retrograde conduction to the atria is equal to the time taken for antegrade conduction to the ventricles, the P wave falls within the QRS. No separate P wave is seen. If the time taken for retrograde conduction to the atria is more than the time taken for antegrade conduction to the ventricles, the inverted P wave falls after the ORS complex with a short R-P interval.
Inverted P Waves in Leads II, III, aVF and Precordial Leads
If the ectopic arises from the anterior part of the left atrium, it traverses upwards and anteriorly to depolarize the two atria. The impulse is once again moving away from the positive poles of the inferior and precordial leads. P waves are, therefore, inverted in leads II, III, aVF and lead V5 and V6 [7]. As the P wave vector moves anteriorly from the posteriorly placed left atrium, P waves are positive in leads V1 and V2 [8]. P wave inversion in all precordial leads is considered as a sensitive and specific marker of ectopic rhythm originating in the anterior wall of the left atrium [9]. As the impulse originates in the anterior wall of the left atrium, it faces normal delay in atrioventricular conduction. PR interval is, therefore, normal. P wave inversion in lead V6 is the most sensitive sign that suggests left atrial focus [8].
Inversion Of P Wave in Leads II, III, aVF, V5 and V6 with Positive P Wave in Lead V1
It suggests ectopic focus in the inferior part of the left atrium [6, 10].
Negative P Wave in Leads II, III, aVF and Positive P Wave in Lead V6 with Negative P Wave in Lead V1
It suggests ectopic focus in the postero inferior right atrium or coronary sinus [6, 8, 10]
Inversion of P Wave in Lead I
As the atrial depolarization vector moves towards the right atrium, it moves away from the positive pole of lead I. Thus P wave inversion in lead I also suggests left atrial origin of the ectopic focus. In situs inversus with dextrocardia, sinoatrial node is situated at the junction of the left superior vena cava and left-sided (morphologic right) atrium [7, 8]. Atrial depolarization, therefore, proceeds from left to right. This also produces P wave inversion in leads I and aVL, P wave is positive in lead aVR Campbell M, et al. [11] and PR interval is normal. In some other congenital defects with the absence of joining of SVC with the right atrium, the absence of sinoatrial node in the right atrium also produces left atrial rhythm. This is seen in left persistent superior vena cava, left atrial isomerism and superior sinus venosus atrial septal defect [12, 13, 14].
Reverse progression of the R wave in precordial leads helps differentiation from technical dextrocardia (reversal of limb leads) which also produces inversion of the P wave in lead I. However, lead I also shows negative QRS and T waves resembling normal lead aVR. Precordial leads also show the normal progression of the R wave.
Dome and Dart P Wave in Lead V1
Some cases of congenital heart disease with left atrial rhythm show ‘dome and dart’ P waves in lead V1. The initial low amplitude and rounded (dome-like) part of the P wave is generated by slow depolarization of the left atrium. It is followed by a sharp spike of greater amplitude (dart) by rapid depolarization of the right atrium. A ‘dome and dart’ P wave in leads V1 or V2 is diagnostic of left atrial rhythm [15].
P Waves Simulating Sinus P Waves
If the ectopic focus is situated in the vicinity of the sinoatrial node or upper part of the right atrium the P waves simulates normal sinus node P wave and may be difficult to differentiate from sinus P waves. Minor variations can also occur due to different sites of exit from the sinoatrial node.
Pacing Studies
Studies involving the pacing of different parts of the left atrium Harris BC, et al. [10] and Khalilullah M, et al. [16] have revealed variable configurations of the P waves from different sites. However, most of these cases had dilated and diseased left and/or right atria. Such atria are likely to have fragmentation of the conduction tissue of the two atria. This may result in variations in the direction of the P wave vector on stimulation of different parts of the left atrium. Another limitation of such studies is that atria were paced at a rate faster than the sinus rate. The P wave vectors are therefore likely to be affected by simultaneously occurring discharge of the sinus node. Ectopic atrial rhythms are usually escaped rhythms that appear transiently in the event of slowing of the rate of the sinoatrial node sinus rate. Further, these studies were performed either on patients of secundum ASD or during transseptal left heart catheterization. Congenital absence of part of the interatrial septum or transcatheter creation of an opening in the interatrial septum could also affect the P wave vector.
Present Impression
The direction of the P wave vector and configuration of the P wave discussed above may be an oversimplification of a complex issue. P wave vector may be affected by genetic or acquired variation in the atrial conduction tissue. Therefore, there could be variation in P wave configuration in different leads in cases of ectopics arising from similar focus.
Interpretation of our Cases
In view of the above-mentioned literature, case number 1 had an ectopic focus in the postero inferior right atrium. Case number 2 had an ectopic focus in the inferno-posterior left atrium. Case number 3 had an ectopic focus within the atrioventricular node.
In all the three cases, the rate of the ectopic focus was less than 100/minute. So these ectopic rhythms do not qualify to be labelled as supraventricular tachycardias. In case number 1 and 2, the ectopic rhythm appeared transiently during recovery. In the third case, the ectopic rhythm appeared very transiently during peak exercise. During exercise, the sympathetic drive increases progressively and so does the discharge rate of the sinoatrial node. During recovery, the sympathetic drive declines rapidly and vagal tone increases [17]. It is possible that in our cases, some autonomic imbalance resulted in transient greater inhibition of the sinoatrial node than the subsidiary pacemakers in the atria or the atrioventricular node. This resulted in the transient appearance of the ectopic supraventricular rhythm. Subsequently, the rate of the subsidiary pacemaker fell below that of the sinoatrial node and sinus rhythm again took over the control of heart rate.
To the best of our knowledge, there is no literature regarding the diagnostic or prognostic significance of the transient appearance of such ectopic supraventricular rhythm during exercise electrocardiography. The transient appearance of such rhythm suggests the presence of supraventricular ectopic foci whose rate is close to that of the sinoatrial node. Such foci can compete with the sinoatrial node during decreased sympathetic drive or increase of parasympathetic tone. Such ectopic supraventricular rhythms are usually benign and occur in children or athletes with a high vagal tone [6, 18]. Permanent low atrial rhythms can be associated with congenital heart disease associated with non-development of the sinoatrial node e.g.. left persistent superior vena cava, left atrial isomerism and sinus venosus atrial septal defect [12, 13, 14]. Suppression of sinoatrial node by drugs or prior surgery can also result in the emergence of such ectopic rhythms [6].
Patients with ‘Dome and Dart’ P waves in lead V1 are considered susceptible to spontaneous or induced supraventricular tachycardias [15].
Conclusion
Ectopic supraventricular rhythms can appear during exercise or recovery of the treadmill test. Transient increase of the ectopic supraventricular rhythm above the rate of the sinoatrial node is probably responsible. Inversion of the P waves in leads II, III and aVF suggest a focus in low atria/ in the vicinity of atrioventricular node / in the atrioventricular node or in the coronary sinus. Additional inversion of the P wave in precordial leads V5 and V6 with positive P wave in lead V1 suggests ectopic focus in the inferior part of the left atrium. Negative P waves in leads II, III, aVF with positive P wave in lead V6 but negative P wave in lead V1 suggests ectopic focus in posteroinferior right atrium. P wave inversion in leads II, III, and aVF with a short PR interval suggests focusing within the atrioventricular node. P wave inversion in leads I and V6 suggest left atrial focus. “Dome and Dart” P waves in lead V1 are specific to left atrial rhythm.
References
-
Mittal SR (2023) The P wave and the PR segment. In: Mittal SR (Ed.), Insights into electrocardiograms with MCQs. Springer Nature, Singapore, pp: 27-42.
-
Beder SD, Gillette PC, Garson A, McNamara DG (1982) Clinical confirmation of ECG criteria for left atrial rhythm. Am Heart J 103(5): 848-852.
-
Leon DF, Lancaster JF, Shaver JA, Kroetz FW, Leonard JJ (1970) Right atrial ectopic rhythms: experimental production in man. Am J Cardiol 25(1): 6-10.
-
Gering LE, Surawicz B, Knilons TK, Tavel M (2008) Atrial rhythms. In: Surawicz B, Knilans TK, et al. (Eds.), Chou’s electrocardiography in clinical practice. Saunders, Philadelphia pp: 345-368.
-
Maclean WA, Karp RB, Kouchoaukas NT, James TN, Waldo AL (1975) P wave changes during ectopic atrial rhythm in man: a study utilizing atrial pacing with fixed electrodes. Circulation 52(3): 426-434.
-
Henckell AK, Guestu G, Rosu R, Ciobanu DM, Istratoaie S, et al. (2022) Low atrial rhythm in a large cohort of children from Transluania. Life 12(11): 1895.
-
Perloff JK, Marelli AZ (2012) Cardiac malpositions. In: Perloff JK, Marelli AJ, et al. (Eds.), Perloff’s clinical recognition of congenital heart disease. Elsevier, Philadelphia, pp: 15-40.
-
Mirowski M (1966) Left atrial rhythm: Diagnostic criteria and differentiation from nodal arrhythmias. Am J Cardiol 17(2): 203-210.
-
Mirowski M (1967) Ectopic rhythm originating anteriorly in the left atrium. Analysis of 12 cases with P-wave inversion in all precordial leads. Am Heart J 74(3): 299-308.
-
Harris BC, Shaver JA, Gray S, Kroetz FW, Leonard JJ (1968) Left atrial rhythm. Experimental production in man. Circulation 37(6): 1000-1015.
-
Campbell M, Reynolds G (1952) The significance of the direction of the P wave in dextrocardia and isolated levocardia. Br Heart J 14(4): 481-488.
-
Perloff JK, Marelli JA (2012) Congenital anomalies of vena caval Convention. In: Perloff JK, Marelli JA, et al. (Eds.), Perloff’s clinical recognition of congenital heart disease. Elsevier, Philadelphia, pp: 503-512.
-
Ito-Hagiwara K, Iwasaki YK, Hayashi M, Maru Y, Oka E, et al. (2019) Electrocardiographic characteristics in the patients with a persistent left superior vena cava. Heart vessel 34(4): 650-657.
-
Perloff JK, Marelli JA (2012) Atrial septal defect: simple and complex. In: Perloff JK, Marelli JA, et al. (Eds.), Perloff’s clinical recognition of congenital heart disease. Elsevier, Philadelphia, pp: 212-272.
-
Mirowski M, Neill CA, Taussig HB (1963) Left atrial ectopic rhythm in mirror image dextrocardia and in normally placed malformed hearts: Report of twelve cases with “Dome and Dart” P wave. Circulation 27: 864- 877.
-
Khalilullah M, Shresth NK, Padmavati S (1978) Left atrial rhythm in man: An experimental study. J Electrocardiology 11(4): 375-378.
-
Imai K, Sato H, Hori M, Ozaki H, Yokoyama H, et al. (1994) Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J Am Coll Cardiol 24(6): 1529- 1535.
-
Ascengr DF, Solari M, Anselimi F, Valentini F, Barbati R, et al. (2017) Electrocardiographic changes induced by endurance training and pubertal development in male children. Am J Cardiol 119(5): 795-801.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study