Pulmonary Thromboembolism in the Intermediate PostOperative Period of Laparoscopic Adrenalectomy for an Adrenocortical Adenoma with Cushing’s Syndrome
Introduction: Cushing’s Syndrome is a constellation of clinical features resulting from chronic exposure to excess glucocorticoids. This is suggested to induce hypercoagulability, which results in a 10-fold increase in the risk for venous thromboembolic events. It results from an increased production of procoagulant factors and impaired fibrinolytic, leading to decreased activated partial thromboplastin time and increased clot lysis time. However, reported events are quite rare and majority of which occur in the post-operative setting. A systematic review done in 2009 by Zaane, et al., discussed that there is up to a 1.5% incidence of venous thromboembolism after transsphenoidal surgery and 0.3-3% after laparoscopic adrenalectomy. Despite this, it is still up to debate whether thromboprophylaxis should be instituted post-operatively among these patients. Discussion: The case is a 42-year-old Filipino, female, with Cushing’s Syndrome readmitted because of generalized body weakness, seven days after laparoscopic adrenalectomy of a left adrenocortical adenoma. After correction of electrolytes and further evaluation, findings suggested the possibility of an infection of the post-operative site. This was confirmed with a whole abdominal CT scan with contrast. She was then managed conservatively with antibiotics. The study was repeated four days after for surveillance of the abscess site. It showed incidental findings of diffuse thromboembolism on the right main pulmonary artery and its segmental branches, right common iliac vein, internal iliac vein, superior gluteal vein, and left ovarian vein. No hypotension, dyspnea, syncope, leg pain, or swelling was noted during this period. Findings were confirmed through CT Angiography of Pulmonary Arteries. Furthermore, no right ventricular dysfunction was noted on 2D echo. She was then treated with loading dose of Rivaroxaban and eventually sent home well after resolution of infection and maintained on anticoagulation.
Introduction
Cushing’s Syndrome (CS) is a constellation of clinical features resulting from chronic exposure to excess glucocorticoids [1]. This could be due to either an excess secretion of adrenocorticotrophic hormone (ACTH), or and ACTH-independent cortisol produced endogenously or introduced exogenously. This result in multiple systemic manifestations related to excess cortisol, including catabolic effects, central fat redistribution and psychiatric manifestations. First-line treatment among those with suspected endogenous secretion of the culprit hormone is surgical resection of the source. Some patients may need medical therapy, bilateral adrenalectomy, or radiation [2].
Hypercortisolism is suggested to induce hypercoagulability, which results in a 10- to 18-fold increase in the risk for venous thromboembolic events (VTE) compared to the general population. This is first observed by the increased incidence of VTE among post-operative patients with Cushing’s Disease compared to those with non-functioning adenoma [2]. It results from an increased production of procoagulant factors (von Willebrand Factor, Fibrinogen, Factor VIII) and impaired fibrinolysis, leading to decreased activated partial thromboplastin time and increased clot lysis time. Initially thought to be rare, evidence present its prevalence both in the pre-op (1.9-2.5% unprovoked) and post-op setting (1.5% in transsphenoidal, 3% in laparoscopic adrenalectomy) [2, 3, 4]. Despite this, there are no established guidelines which recommend screening or thromboprophylaxis pre- and post-operatively among patients with Cushing’s Syndrome.
Case Description
The case is a 42-year-old Female, Filipino, diagnosed with Cushing’s Syndrome readmitted because of generalized body weakness, seven days after laparoscopic adrenalectomy of a left adrenocortical adenoma. After correction of electrolytes and further clinical evaluation, findings suggested the possibility of an infection of the post-operative site. This was confirmed through whole abdominal CT scan with contrast. She was then managed conservatively with antibiotics. The contrast study was repeated after four days for surveillance of the abscess site. It showed incidental findings of diffuse thromboembolism on the right main pulmonary artery and its segmental branches, right common iliac vein, internal iliac vein, superior gluteal vein, and left ovarian vein. Findings were confirmed on CT angiography of pulmonary arteries with venogram.
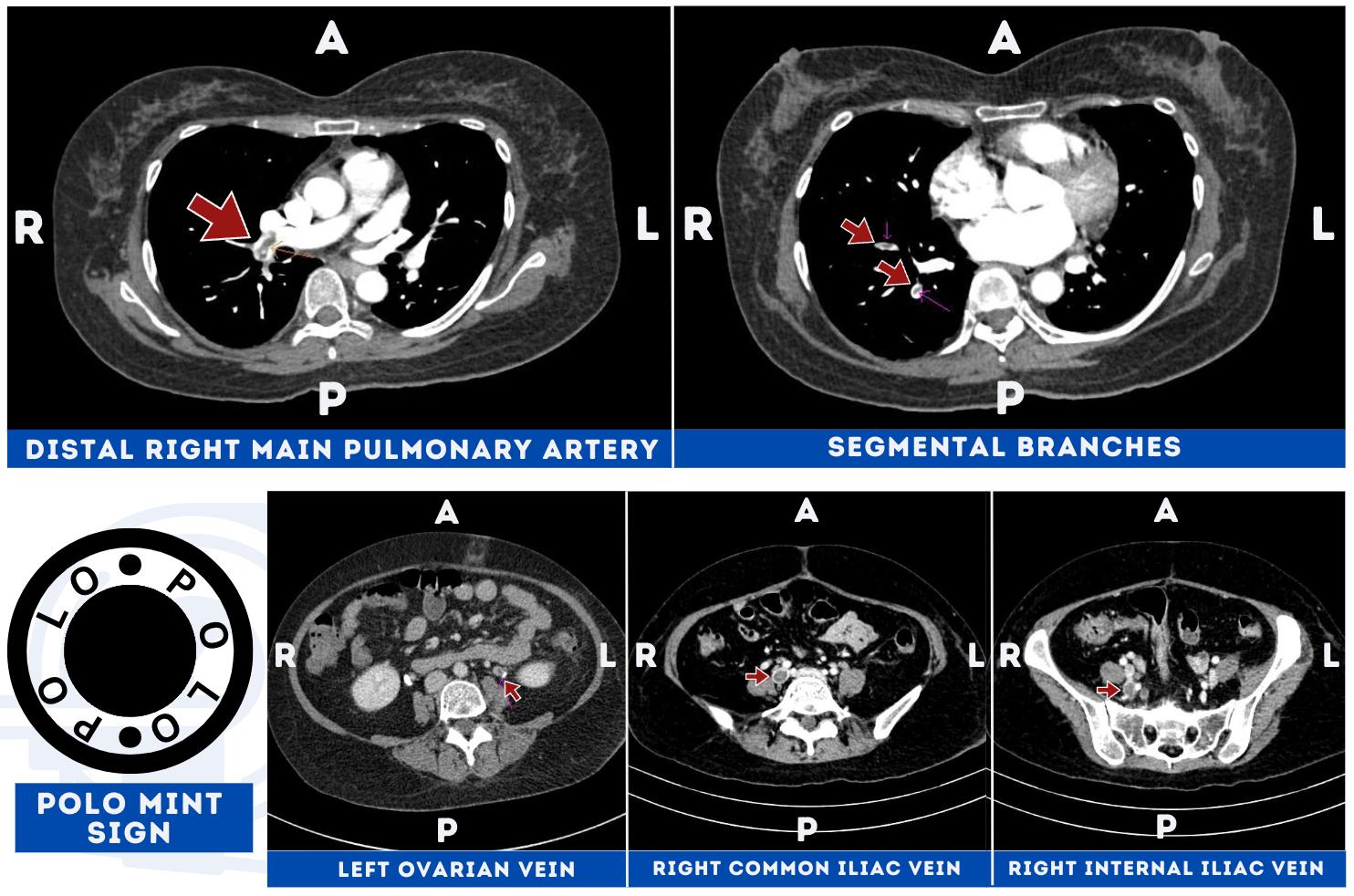
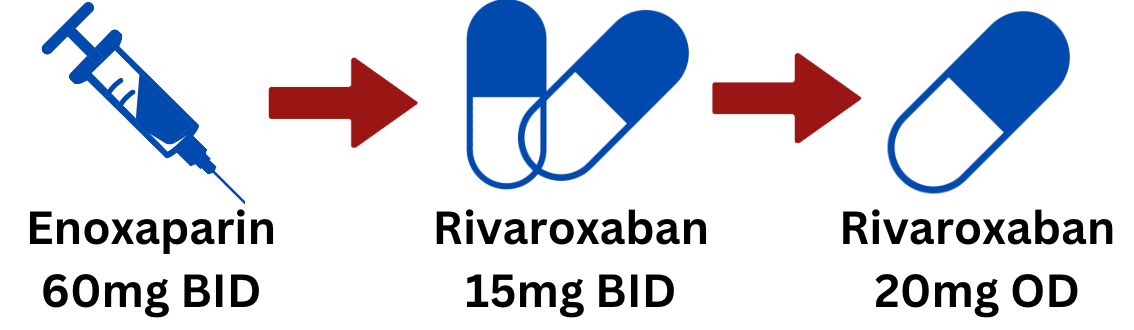
There were no clinical findings suggestive of diffuse acute venous thromboembolism (hypotension, dyspnea, syncope, leg pain, swelling) at that time. Transthoracic 2D echocardiography showed normal right ventricular size with adequate systolic function and normal pulmonary artery pressure. Furthermore, there was no noted left ventricular dysfunction, with normal dimensions of the left ventricle, left atrium, and right atrium. Due to financial constraints, cardiac biomarkers were not requested as it would not change the course of management and she was classified to low to intermediate-low risk pulmonary embolism at most with a pulmonary embolism severity index (PESI) of I. She was then treated with a single weight-appropriate dose of subcutaneous Enoxaparin, then eventually shifted to a loading dose of Rivaroxaban (15mg twice daily) for 3 weeks, and was sent home well after resolution of infection and maintained on maintenance anticoagulation (20mg once daily) for 5 months. Surveillance using CT-PA after 4 months of therapy showed interval resolution of pulmonary embolism, right internal iliac vein, right superior gluteal vein, and left ovarian vain with partial lysis of the thrombus in the right common iliac vein.
Discussion
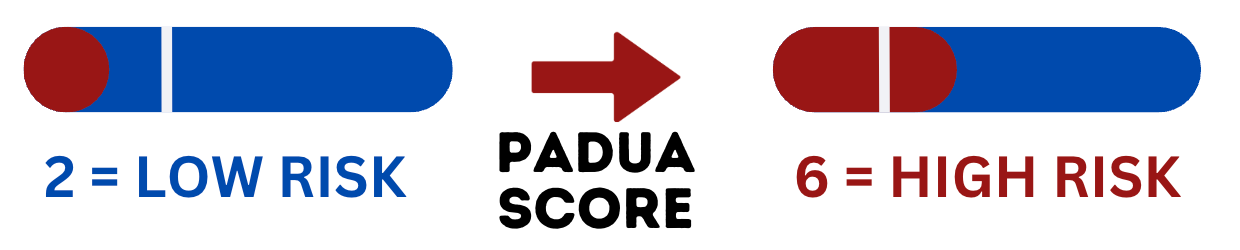
Venous Thromboembolism (VTE) is the umbrella term for the clinical presentation of pulmonary embolism (PE) and deep venous thrombosis (DVT). It is the third most common acute cardiovascular syndrome after myocardial infarction and cerebral infarction with an annual incidence rate of 39- 115 per 100,000 population for PE and 53-162 per 100,000 population for DVT [5, 6, 7]. There is a broad list of recognized genetic and environmental risk factors for VTE. Weak risk factors present in this case include recent laparoscopic surgery, bed rest of at least 3 days, and diabetes mellitus [8]. This translates to a Padua score of 2 which classifies the patient as low risk for thromboembolism. However, the unanticipated immobility of the patient due to an apparent post-operative site infection which translated to generalized body weakness increased the Padua Score of the patient to 6. Thus, patient had a significant risk for pulmonary thromboembolism. Furthermore, the excess cortisol may have also played a role predisposing the patient to diffuse thromboembolism as multiple studies suggest the increased risk for VTE on both pre- and post-operative period [2, 3, 4, 9].
There is limited literature providing recommendations regarding diagnostic algorithm, management, and thromboprophylaxis for VTE among patients with Cushing’s Syndrome. Published studies are still inclined in providing association between the two. As such, attending physicians followed the latest recommendations by the European Society of Cardiology set for the general population in the management of this case. Diagnosis was based on assessing the presence of high risk features to be addressed such as hemodynamic instability, dyspnea, chest pain, syncope, tachycardia, tachypnea, hypoxemia and hemoptysis. All of which are not present in the patient. The pre-test probability of patients are normally computed using the Wells or Geneva Rule to decide on the appropriate diagnostic study. However, due to the diffuse incidental finding on the patient, confirmation through the highly sensitive and specific CT angiography of Pulmonary Arteries and Venogram was facilitated [10]. Further diagnostic tests showed an elevated D-Dimer (high negative predictive value, low positive predictive value) and no significant chest findings on chest X-ray. Patient refused to undergo extraction for arterial blood gas to assess subclinical hypoxemia and Troponin for risk stratification.
Transthoracic 2D echocardiography is primarily used to assess right ventricle (RV) pressure overload and dysfunction through measurement of RV diameter, Tricuspid Annular Plane Excursion (TAPSE), and RV fractional area change (RVFAC). It is not used to rule out PE as it has a high negative predictive value at 40-50% [11]. Other high risk features that should be investigated are the presence of pulmonary ejection acceleration time (PAT) <60ms, peak tricuspid valve gradient >60mmHg, McConnell’s sign (decreased RV contractility with apical sparing), and a visible right heart thrombi. High-risk findings were not appreciated in the patient’s study.
Assessment of pulmonary embolism severity and risk of early death is crucial in the management of acute pulmonary embolism. This is assessed by detecting the presence of hemodynamic instability, evaluating the PESI, detecting the presence of RV dysfunction through imaging, and evaluating troponin levels [6]. Due to the refusal of the patient to undergo testing for cardiac biomarkers, we cannot fully assess the PE severity. However, the absence of RV dysfunction in a hemodynamically stable patient with a PESI of I, stratifies the patient low to Intermediate-low risk at most.
Treatment in the acute phase of VTE include hemodynamic and oxygen support to address mismatch in ventilation and perfusion. Assessment of central venous pressure is crucial as it allows assessment if fluid challenge (<500mL) can be reinstated or if inotropic support (Norepinephrine/Dobutamine) is immediately warranted to support blood pressure. The cornerstone of treatment of VTE is parenteral anticoagulation (low molecular weight heparin, fondaparinux, unfractionated heparin). Recent studies suggest that oral anticoagulation using loading dose of Apixaban for 7 days and Rivaroxaban for 21 days, confer the same effect as parenteral medications [12, 13, 14]. It is recommended to be started even while awaiting results of diagnostic tests among patients with high probability and continued with maintenance dosage for at least 3 months. Since PE of patient is intermediate-low risk at most, systemic/ catheter-directed thrombolysis, or surgical embolectomy is not warranted.
Patient was discharged as soon as antibiotic therapy for post-operative site infection was completed. The presence of intermediate-low risk PE should not delay discharge of patients as outpatient anticoagulant therapy can be done as long as there is adherence to the prescribed regimen and serious co-morbidity or aggravating condition is absent. Furthermore, the Hestia exclusion criteria and PESI use bedside clinical parameters to predict the risk of recurrence or progression to high risk VTE [8]. The minimum duration of anticoagulation is 3 months as risk of recurrence is similar if anticoagulation is extended beyond 6 months, while subjecting patients to bleeding risk [8]. Patient was followed-up after 4 months, with repeat CTPA revealing resolution of pulmonary embolism, right internal iliac vein, right superior gluteal vein, and left ovarian vain with partial lysis of the thrombus in the right common iliac vein. Patient’s Rivaroxaban stocks were then consumed after 1 month without any incidence of major bleeding throughout treatment and patient was asked to be followed up every 6 months thereafter.
Conclusion
There are no established recommendations among patients with VTE and Cushing’s Syndrome. High-value evidence suggest association between hypercortisolism and VTE due to hypercoagulability. Appropriate VTE prophylaxis can therefore be recommended in the post-op setting among patients with Cushing’s Syndrome to prevent its occurrence, especially among those with high risk features such as anticipated immobility.
References
-
Loscalzo J, Fauci AS, Kasper DL, Hauser SL, Longo DL, et al. (2022) Harrison’s Principles of Internal Medicine. In: 21st (Edn.), McGraw Hill.
-
Wagner J, Langlois F, Ting Lim DS, McCartney S, Fleseriu M (2019) Hypercoagulability and Risk of Venous Thromboembolic Events in Endogenous Cushing’s Syndrome: A Systematic Meta-Analysis. Frontiers in Endocrinology 9: 805.
-
Fielders RA, Nieman LK (2022) Hypercoagulability in Cushing’s syndrome: incidence, pathogenesis and need for thromboprophylaxis protocols. Pituitary 25(5): 746- 749.
-
Van der Pas R, Leebeek FWG, Hofland LJ, de Herder WW, Feelders RA (2013) Hypercoagulability in Cushing’s syndrome: prevalence, pathogenesis and treatment. Clinical Endocrinology (Oxford) 78(4): 481-488.
-
Raskob GE, Angchaisuksiri P, Blanco AN, Buller H, Gallus A, et al. (2014). Thrombosis: a major contributor to global disease burden. Arterioscler Thromb Vasc Biol 34(11): 2363-2371.
-
Wendelboe AM, Raskob GE (2016) Global burden of thrombosis: epidemiologic aspects. Circ Res 118(9): 1340-1347.
-
Keller K, Hobohm L, Ebner M, Kresoja KP, Munzel T, et al. (2020) Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in Germany. Eur Heart J 41(4): 522-529.
-
Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, et al. (2020) 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society. European Heart Journal 41(4): 543- 603.
-
Van Zaane B, Nur E, Squizzato A, Dekkers OM, Twickler MThB, et al. (2009) Hypercoagulable state in Cushing’s syndrome: a systematic review. Journal of Clinical Endocrinology and Metabolism 94(8): 2743-2750.
-
Stein PD, Fowler SE, Goodman LR, Gottschalk A, Hales CA, et al. (2006) Multidetector computed tomography for acute pulmonary embolism. N Engl J Med 354: 2317- 2327.
-
Roy PM, Colombet I, Durieux P, Chatellier G, Sors H, et al. (2005) Systematic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ 331(7511): 259.
-
Steffel J, Verhamme P, Potpara TS, Albaladejo P, Antz M, et al. (2018) The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J 39(16): 1330-1393.
-
Agnelli G, Buller HR, Cohen A, Curto M, Gallus AS, et al. (2013) Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med 369: 799-808.
-
Buller HR, Prins MH, Lensin AW, Decousus H, Jacobson BF, et al. (2012) Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 366(14): 1287-1297.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study