Multiple Solitary Plasmacytoma of Chest Wall and Scalp with Extramedullary Solitary Plasmacytoma of Orbit Occurring Simultaneously: A Rare Case Report
Extramedullary plasmacytoma concurrent with multiple solitary plasmacytoma is very rare presentation and multiple myeloma should be excluded very vigilantly in these cases. Though radiotherapy is treatment of choice but conventional oral chemotherapy can also give equivalent results in few cases. Close follow up is required as most of the cases develop multiple myeloma in future. Plasmacytoma of orbit and subcutaneous tissue with no systemic involvement at present may be the first of its kind to be reported to the best of our knowledge. Treatment with alkylating chemotherapy reduces tumour bulk. However, the risk of progression to multiple myeloma being not yet documented should always be kept in mind.
Introduction
Extramedullary Medullary Plasmacytomas make up 4% of all plasma cell tumors and occur mainly in the upper aerodigestive tract while the incidence of multiple solitary plasmacytoma is 0.35/100 000/year, representing 5–10% of all plasma cell neoplasms. Concurrent cases are not mentioned in the literature.
Plasma cell neoplasm can manifest as systemic disease namely multiple myeloma and its variants such as indolent myeloma, smoldering myeloma, osteosclerotic myeloma, plasma cell leukemia and non-secretory myeloma or localized disease represented as solitary plasmacytoma of bone (SMB) or extra medullary plasmacytoma (EMP). Solitary plasmacytoma presenting Multiple Solitary Plasmacytoma of Chest Wall and Scalp with Extramedullary Solitary Plasmacytoma of Orbit Occurring Simultaneously: A Rare Case Report as a soft tissue mass in more than one site is therefore a very rare event and not usually included in the differential diagnosis of other more common soft tissue masses, such as sarcomas, fibrous tumours, haemangiomas, neurofibromas or lymphomas. Extramedullary plasmacytoma is an isolated tumour of monoclonal plasma cells that develops in soft tissue rather than bone. It constitutes about 4% of all plasma cell tumours. 90% of EMP cases develop in the head and neck area especially in the upper respiratory tract, including nasal cavity and sinuses, nasopharynx and larynx. Infrequent sites of involvement include the gastrointestinal tract, liver, spleen, pancreas, lungs, thyroid, breast, testis or skin. Radiation therapy is J Cancer Oncol
generally accepted as the treatment of choice. The role of chemotherapy for localized tumour is not well defined.
We present here a case report of solitary plasmacytomas of the left orbit concurrent with scalp and left chest wall plasmacytoma in a 55-year old male whose thorough diagnostic workup was negative for multiple myeloma and he showed complete resolution with non- conventional treatment that is oral chemotherapy in the form of tab melphalan and thalidomide.
Case History
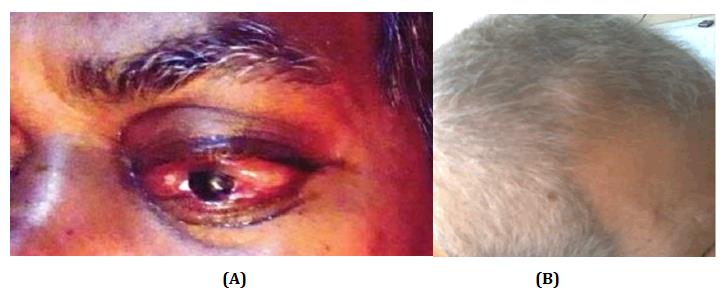
A 55-year old male presented with swelling in left eye and scalp region since 20 days. Swelling was insidious in onset gradually progressive associated with bulging of left eye with redness, watering and blurring of vision. On examination he was found to have ptosis due to marked oedema of left upper eyelid and marked congestion of the left eyeball. A palpable non-tender mass of size approximately 5x4 cm was felt within the left orbit.
Ocular motility was restricted in almost all directions of gaze. Left eye visual acuity was hand movement with perception of light. The intraocular pressure was 17.3 mm of Hg. Slit light examination showed hazy cornea, chemosed conjunctiva, anterior chamber filled with exudates. On Fundoscopy, left eye fundus could not be visualised due to hazy media. Ophthalmic examination of right eye was unremarkable. Two lumps of approximate size 1x1 cm and another adjacent lump of size 5x5 cm were palpable in vertex region on scalp, which were non- tender and fixed. One more lump was palpable over the left chest wall of approximate size 5x 6 cm, non-tender and fixed to underlying structure.
Orbital CT scan demonstrated smooth space occupying lesion in left orbit occupying posterio-superior side of eyeball extending into frontal sinus and cranial cavity causing destruction of adjoining bone and proptosis on left side.
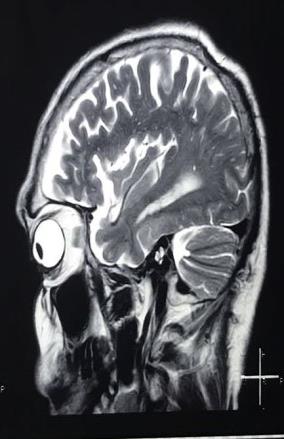
MRI brain and orbit showed expansile mass lesion of 4.5x3.6x3.5 cm in left orbit and supraorbital frontal wall causing mass effect over frontal lobe as well as over left orbit.Multiple altered signal intensity mass lesion in the calvarial and bilateral fronto-temporal-parietal occipital bone. One of the lesions in right parietal lobe causing indentation over parietal lobe. CECT Thorax revealed soft tissue density mass measuring 65x58mm in left thorax wall in 6th rib laterally.
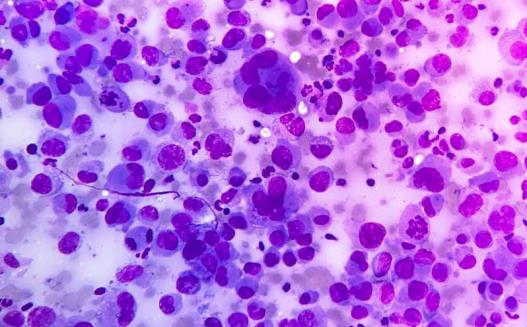
Fine needle aspiration cytology of left chest wall and scalp swelling were suggestive of plasma cell tumour. Patient was advised for biopsy from scalp lesion but he was very reluctant for the same.
Serum electrophoresis was negative for M-band. Alpha-2 was increased but beta gamma reduced. Serum free light chains and immunohistochemistry (CD138) was not done due to financial crisis.CBC and KFT were within normal limit. USG abdomen and pelvis revealed only cystitis. Urine BJ Protein was negative. Bone marrow aspiration showed normal marrow. After complete workup patient was diagnosed a case of multiple solitary plasmacytoma.
Patient was very apprehensive for further histopathological examination so was kept on oral chemotherapy (tablet melphalan 10mg/day, prednisolone 100mg/day in divided dose for 4days with Thalidomide 100mg/day for 28days repeated every 4week) with inj zolidronic acid 4mg i/v monthly. After first cycle of chemotherapy, patient showed very good subjective as well as objective response, so oral therapy was continued.
After 4 week from start of treatment there was complete regression of scalp swelling. Proptosis and orbital congestion was markedly reduced with increase in visual acuity to finger counting.



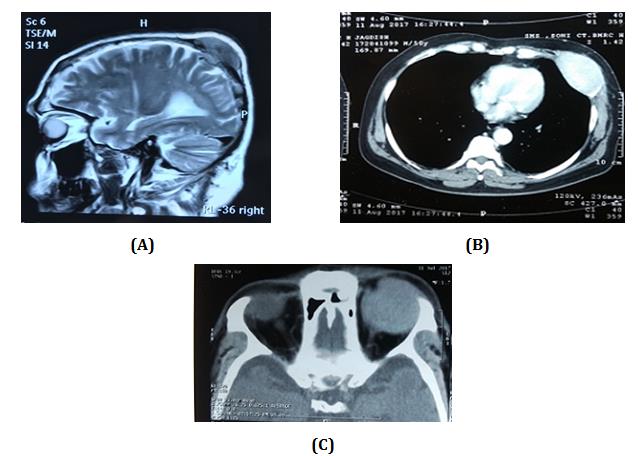
(A) (B) (C) Figure 5: After one month of treatment imaging study showed complete resolution of mass (A) MRI brain, (B) CT thorax, (C) CT orbit.
Discussion
The International Myeloma Working Group in 2003 classified plasmacytomas as solitary plasmacytoma of bone (SBP) when a single bone lesion was present, solitary extramedullary plasmacytoma(SEP) when a solitary soft-tissue lesion was present and multiple solitary plasmacytoma (MSP) when multiple sites of disease were present in soft tissue, or both[1]. SBP, SEP and MSP are rare clinical entities, characterised by a monoclonal plasma cell infiltrate in bone or soft tissue, cytologically and immunophenotypically identical to multiple myeloma (MM). EMP occurs predominantly in males at the ratio of 3:1.The majority of patients affected are between 50 and 70years of age. The incidence of these entities is 0.35/100 000/ year, representing 5–10% of all plasma cell neoplasms [2].
Primary plasmacytoma, whether osseous or nonosseous, is distinguished from multiple myeloma by absence of hypocalcaemia, renal insufficiency and anaemia, normal skeletal survey, absence of bone marrow plasmacytosis, and serum or urinary paraprotein_<_2 g/dl.
The diagnosis of EMP requires demonstration of a monoclonal plasma cell infiltrate with no evidence of myeloma at any other site. Therefore, patients with presumed solitary plasmacytoma of bone or soft tissue (extramedullary) plasmacytoma should undergo a radiological bone survey and MR imaging to ensure that only one lesion is present. The diagnosis of multiple solitary plasmacytoma requires no M-protein in serum/urine, more than one localized area of bone destruction or extramedullary tumour of clonal plasma cells, normal bone marrow, normal skeletal survey, no related organ or tissue impairment [3].
Solitary plasmacytomas can arise at any site, but almost 90% develop in the head and neck area and especially in the upper respiratory tract (nose, paranasal sinuses, nasopharynx and tonsils). Infrequent sites of involvement include the gastrointestinal tract, liver, spleen, pancreas, lungs, thyroid, breast, testis or skin [4, 5]. Orbital swelling may also be due to orbital lymphoma or may be due to lymphoid hyperplasia but in these cases orbital involvement occurs usually in superolateral direction with intraorbital involvement.
After thoroughly investigations our patient was diagnosed a case of multiple solitary plasmacytoma of chest wall and scalp with extramedullary solitary plasmacytoma of orbit occurring simultaneously.
Because of its rarity and heterogeneous presentation, no clear guidelines are available for MSP treatment. Most of the information available regarding the best treatments is found in single or multicentre retrospective series. Chemotherapy, radiotherapy and surgery have been tried with variable results.
While for single-lesion cases of plasmacytoma (SBP and SEP) surgical excision followed by radiation therapy appears a reasonable approach, for multiple-lesions disease (MSP) surgery, radiotherapy and chemotherapy are indicated.
The prognosis of orbital plasmacytoma is good, with a mean survival of 8.3 years in extramedullary plasmacytomas as compared to only 20 months in patients with multiple myeloma. Thus, the presence of systemic tumour is an important prognostic indicator and needs to be evaluated in every case of suspected extramedullary plasmacytomas. In addition, a prolonged follow-up is required to check on the development of multiple myeloma. SEMP represents 3% of plasma cell neoplasms. Seventy-nine percent of lesions occur in the upper respiratory tract, with less common involvement of the gastrointestinal tract and lymph nodes [6, 7]. Current therapeutic options include external beam radiotherapy or local excision [8, 9]. The mean survival time for patients is 8.3 years [6, 9]. In ocular tissue, SEMP has been reported in the orbit and conjunctiva [8, 9].
SEMP of ocular tissue is generally treated with external beam radiotherapy or local excision. More than half of subjects diagnosed with solitary plasmacytomas (52–80% of patients with SBP and 10–44% of patients with SEP) would develop MM later in life [4, 5].
Up to now only few cases of MSP have been reported in literature. Kulbacki et al presented a case of MSP in a young patient with lytic lesions in C1 vertebrae; first left rib and hip [10]. The biopsy of the lesion was positive for CD38, CD138, CD56 and κ-light chain but was negative for CD19, CD20, cyclin D1 and λ-light chain. Collier et al reported a case of an adult man with MSP who presented with raised intracranial pressure. Small lytic lesions were seen on radiographs of the skull, sacrum and left clavicle [11].
Ooi et al describe six patients with MSP, four cases with multiple extramedullary plasmacytomas (MEMP) and two cases with both bone and extramedullary lesions [6]. Shih, et al. collected 32 patients with SPB or SEP and they reported different kind of relapse after therapy: local single recurrence of SPB or SEP, multiple bone plasmacytomas, MEMP or MM [12].
Katzmann, et al. reported 899 patients with plasma cell dyscrasia and monoclonal gammopathies; among these patients, there were 27 with SBP or SEP and 3 with MSP.
Various studies recommended either surgery followed by radiotherapy or radiotherapy alone for solitary plasmacytoma management and suggested that adjuvant chemotherapy has no impact on PFS and OS or progression to MM. No data is available for definitive chemotherapy in solitary plasmacytoma.
Though radiotherapy is usually considered treatment of choice in these cases but our patient was reluctant for any surgical or radiotherapy treatment so we kept our patient on Tab melphalan, prednisolone and thalidomide and inj Zolidronic acid 4mg I/V monthly. Till date patient has completed 4 cycles of chemotherapy and is totally asymptomatic.
Conclusion
Plasmacytoma of orbit and subcutaneous tissue with no systemic involvement at present may be the first of its kind to be reported to the best of our knowledge. Treatment with non-conventional modality i.e. alkylating chemotherapy reduces tumour bulk and sometime may produce complete response. However, the risk of progression to multiple myeloma being not yet documented, should always be kept in mind, mandating a close follow-up of this patient and series of more number of patients are required to comment on significance of oral chemotherapy in these subset of patients.
References
-
International Myeloma Working Group (2003) Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. British Journal of Haematology 121(5): 749-757.
-
Kilciksiz S, Karakoyun-Celik O, Agaoglu FY, Haydaroglu A (2012) A review for solitary plasmacytoma of bone and extramedullary plasmacytoma. Scic World J.
-
(2009) Guidelines on the diagnosis and management of solitary plasmacytoma of bone, extramedullary plasmacytoma and multiple solitary plasmacytomas. United Kingdom Myeloma Forum.
-
Dagan R, Morris CG, Kirwan J, Mendenhall WM (2009) Solitary plasmacytoma. Am J Clin Oncol 32(6): 612- 617.
-
Wiltshaw E (1976) The natural history of extramedullary plasmacytoma and its relation to solitary myeloma of bone and myelomatosis. Mrdicine 55(2): 217-238.
-
Ooi GC, Chim JC, Au WY, Khong PL (2006) Radiologic manifestations of primary solitary extramedullary and multiple solitary plasmacytomas. AJR Am J Roentgenol 186(8): 821-827.
-
Mulligan ME (2007) Myeloma updates. Seminars in Musculoskeletal Radiology 11(3): 231-239.
-
Bataill R, Sany J (1981) Solitary myeloma: clinical and prognostic features of a review of 114 cases. Cancer 48(3): 845-851.
-
Aboud N, Sullivan T, Whitehead K (1995) Primary extramedullary plasmacytoma of the orbit. Aust N Z J Ophthalmol 23(3): 235-239.
-
Kulbacki E, Wang E (2012) Pathological bone fractures in a 20-year-old athletic male with multifocal solitary plasmacytoma of bone. Am J Hematol 87(6): 626-627.
-
Collier A, Ashworth B (1987) Multiple plasmacytoma presenting as raised intracranial pressure. J Neurol Neurosurg Psychiatry 50(4): 495-496.
-
Shih LY, Dunn P, Leung WM, Chen WJ, Wang PN (1995) Localised plasmacytomas in Taiwan: comparison between extramedullary plasmacytoma and solitary plasmacytoma of bone. Br J Cancer 71(1): 128-133.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma