An Incidental Finding of Duodenal Carcinoid Tumor
Neuroendocrine tumors (NETs) are rare, well-differentiated tumors that arise from enterochromaffin cells and are typically found within the digestive tract. Many NETs found within the gastrointestinal tract (GI) are located in the ileum, with duodenal NETs relatively rare. We describe a 56-year-old morbidly obese female who underwent upper gastrointestinal endoscopy (EGD) for refractory gastroesophageal reflux disease (GERD) and was incidentally diagnosed with a grade I NET within the duodenal bulb, which was subsequently resected. As these tumors are often indolent, it is important for clinicians to be cognizant of acting on these incidental findings to help prevent the systemic effects of carcinoid syndrome.
Introduction
NETs, also known as carcinoid tumors, are rare, well- differentiated tumors arising from enterochromaffin cells of the aerodigestive tract. They most commonly arise in the small intestine, and the most common location is in the terminal 60 cm of the ileum. Primary duodenal carcinoids are less common and account for less than 2% of all gastrointestinal carcinoids. Duodenal carcinoids are mostly indolent and discovered incidentally, with very few reported cases of association with carcinoid syndrome [1]. We present to you the case of a patient with a non-functional duodenal carcinoid tumor discovered incidentally during EGD.
Case Presentation
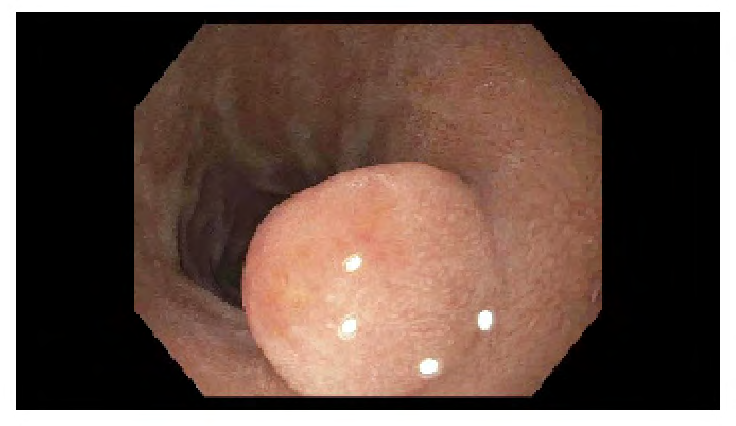
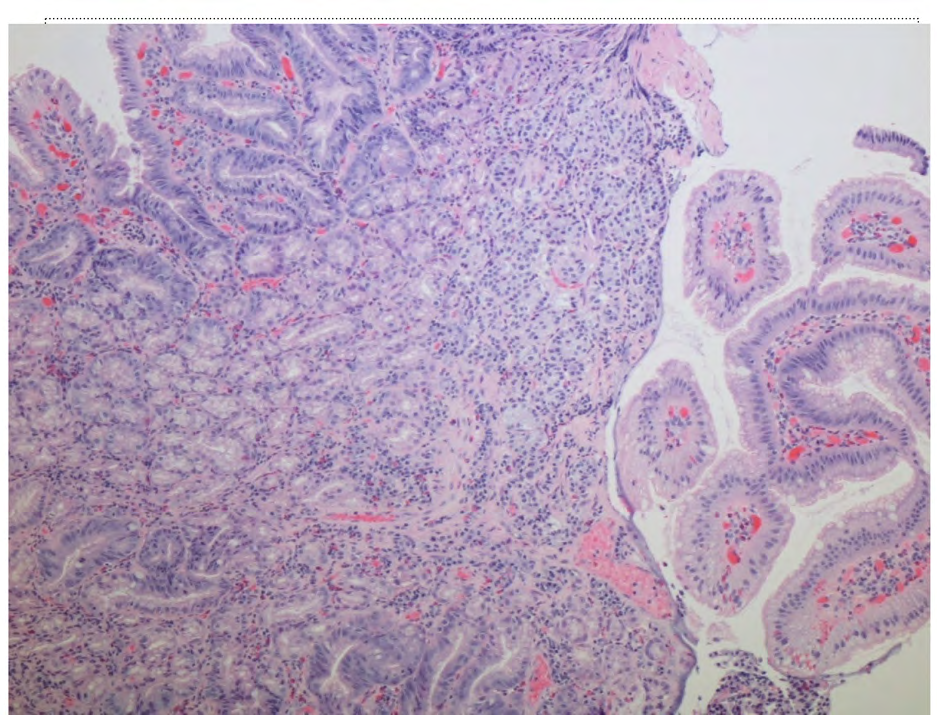
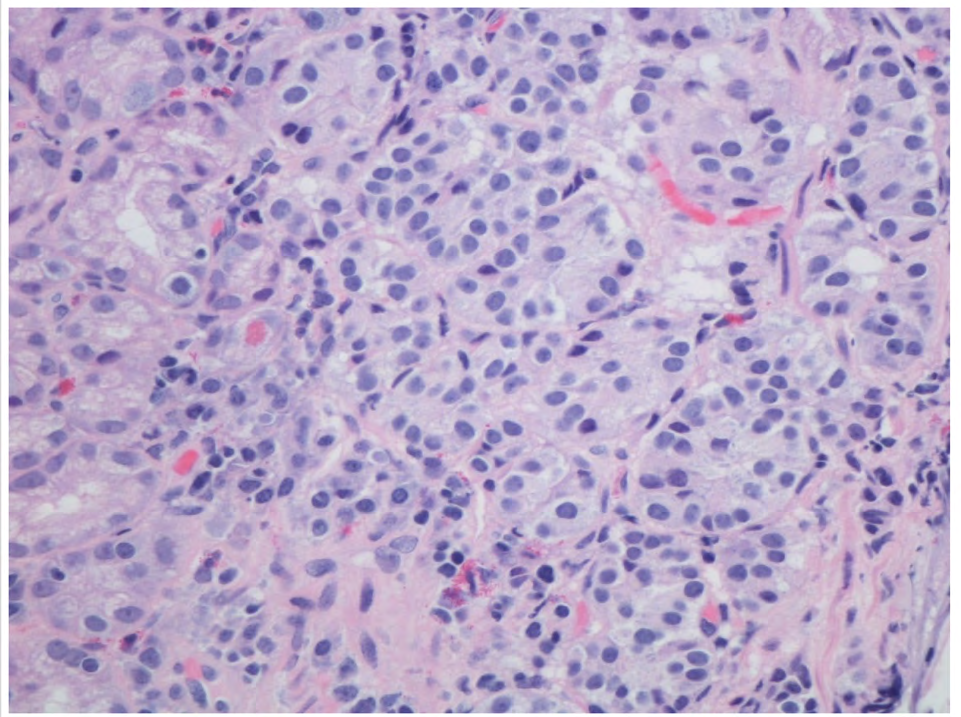
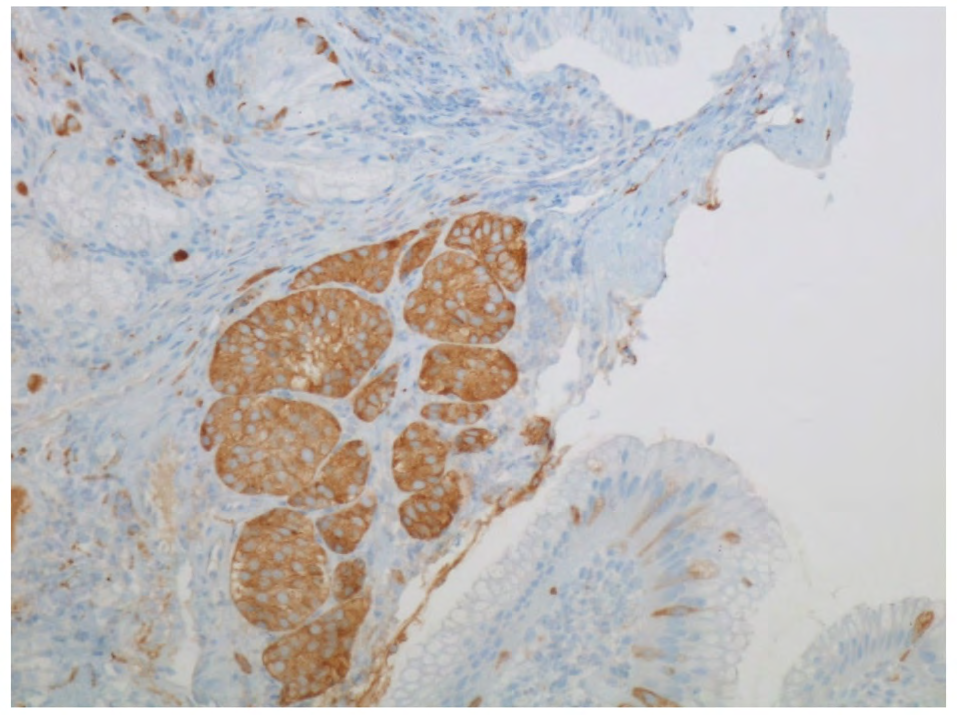
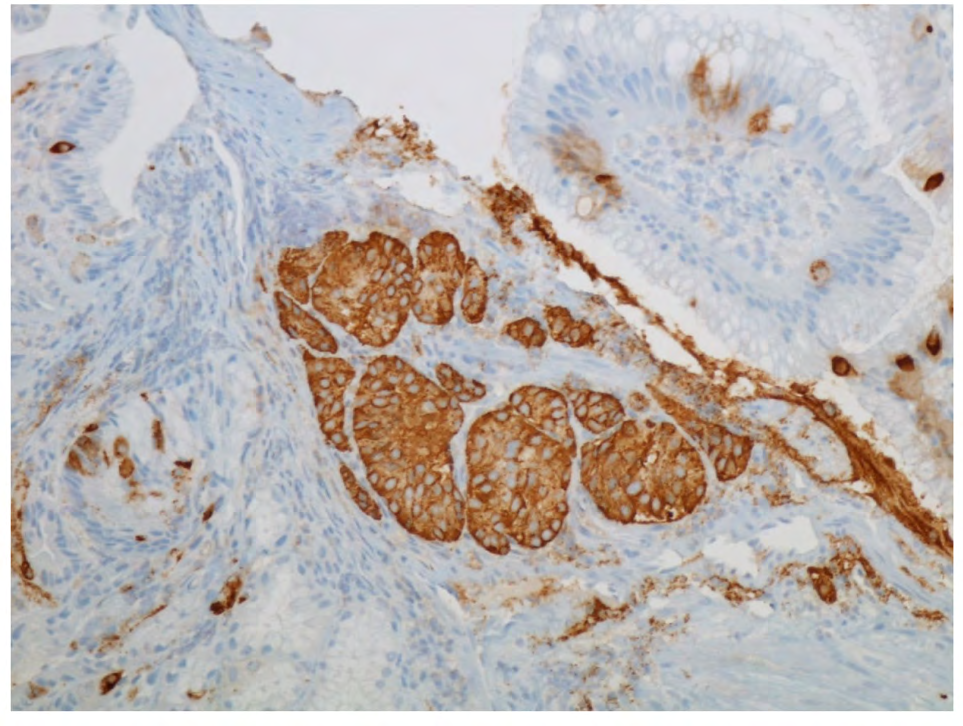
Our patient is a 56- year- old female with a past medical history of severe GERD and no known significant family history who presented to our bariatric surgery clinic for evaluation of morbid obesity and consideration for bariatric surgery. On physical exam, the patient was hemodynamically stable with no other significant findings. However, in view of her severe reflux disease that had not responded to proton pump inhibitor therapy and as a part of her preoperative evaluation for bariatric surgery, an informed decision was made to proceed with an upper gastrointestinal endoscopy. EGD findings included gastritis and a 10-millimeter non- bleeding pedunculated polyp in the duodenal bulb. The polyp was biopsied and removed with a hot snare before being sent for pathological examination. Biopsy results revealed a well-differentiated neuroendocrine tumor with tumor cells positive for synaptophysin, chromogranin A, and CD56. Furthermore, upon deeper sectioning, very few tumor cells were seen, which expressed a Ki-67 labeling index of less than 3%. Based on the combination of low percentage staining and the low mitotic count, the patient was diagnosed with a grade I neuroendocrine tumor. Unfortunately, the serum insulin, glucagon, gastrin, somatostatin, and urine 5-hydroxyindoleacetic acid (5-HIAA) levels were not checked. However, she continued to remain asymptomatic and eventually underwent laparoscopic sleeve gastrectomy.
Discussion
Carcinoid tumors arise from neuroendocrine cells and are relatively uncommon neoplasms. They are most commonly found in the GI tract, followed by bronchopulmonary tracts. The most frequent location within the GI tract is in the small intestine, followed by the appendix, colon, and stomach [2, 3]. Tumors with a primary duodenal origin represent < 2% of all NETs [2, 4]. Their incidence has risen over time due to increased detection by upper gastrointestinal endoscopy. As described in our case, there has also been reported evidence of elevated incidence of carcinoid tumor in obese population [5].
The clinical presentation in most NETs is usually nonspecific with symptoms of abdominal pain, nausea, vomiting, diarrhea, and flushing, with obstructive jaundice seen occasionally due to tumors in close proximity to the ampullary region. NETs localized to the GI tract have a spectrum of presentation, ranging from no clinical symptoms when incidentally discovered on imaging/endoscopy as in our patient to the classical manifestations of carcinoid syndrome, bowel obstruction, and perforation, intussusception, bowel ischemia, and GI bleeding [6].
Tumors arising in the duodenum typically express one or more polypeptide hormones, including somatostatin, gastrin, serotonin, calcitonin, and insulin. Unfortunately, these levels were not checked in our patient. There are five clinicopathological types of duodenal carcinoid (1) gastrinomas, (2) somatostatinomas, (3) nonfunctioning, (4) poorly differentiated, and (5) duodenal gangliocytic paragangliomas [7]. Carcinoid tumors arising in the small intestine have a greater propensity to metastasize compared to those in the appendix, colon, or rectum, with the liver being the most frequent site of metastasis. Most duodenal carcinoids are restricted to the mucosa and submucosa layers, with invasion beyond the submucosa combined with the presence of mitotic figures constituting metastatic disease.
Diagnosis is usually made by measuring serum chromogranin A and urine 5-HIAA level. However, the most sensitive methods for locating carcinoid tumors are Computerized tomography (CT), magnetic resonance imaging (MRI), and somatostatin receptor scintigraphy (SRS) [7, 3]. In duodenal tumors, EGD remains the most sensitive method, as these tumors are generally under 1 cm. This is often complemented with endoscopy ultrasonography (EUS), when possible, to help define the tumor size, level of wall invasion, and the presence of regional lymphatic metastases.
The ideal treatment for duodenal carcinoids is endoscopic resection or surgery [8]. For small tumors <1cm, endoscopic removal is the preferred treatment as done in our patient. Tumors that are 1-2 cm can be removed endoscopically or by transduodenal full-thickness resection using laparotomy or laparoscopy, depending on the invasion depth. Tumors > 2 cm are treated exclusively by surgery. Regional lymphadenectomy is recommended when lymph node involvement is detected on imaging or mitotic index is higher than two mitotic figures per HPF. In the case of ampullary or periampullary tumors, surgical excision is preferred regardless of tumor size [3]. In patients with metastatic disease, systemic therapy with somatostatin analogs, peptide receptor radionuclide therapy, and chemotherapy can be used.
Conclusion
Duodenal carcinoid tumors are extremely rare, and our case is unique, representing the indolent subset of NETs. Their incidence is high in obese population our case reinforces the importance of performing an endoscopic procedure before bariatric surgery.
References
-
Naalla R, Konchada K, Kannappan O, Lingadakai R (2014) Duodenal carcinoid with carcinoid syndrome. BMJ Case Rep 2014: bcr2013202159.
-
Mullen JT, Wang H, Yao JC, Jeffery HL, Nan- cy DP, et al. (2005) Carcinoid tumors of the duode- num. Surgery 138(6): 971-977.
-
Negrean V, Buchman C, Perne MG, Milaciu M, Domsa L, et al. (2020) Duodenal carcinoid tumour-a case report. JMMS 7(1): Article 19.
-
Nikou GC, Toubanakis C, Moulakakis KG, Spiridon P, Elias M, et al. (2011) Carcinoid tumors of the duodenum and ampulla of Vater: current diagnostic and therapeutic approach in a series of 8 patients. Case series. Int J Surg 9(3): 248-253.
-
Mottin CC, Cruz RP, Gomes Thomé G, Padoin AV (2009) Carcinoid tumors and morbid obesity. Obes Surg 19(2): 247-249.
-
Abraham A, Singh J, Siddiqui G, Prasad A, Vikas G, et al. (2012) Endoscopic management of a primary duodenal carcinoid tumor. Case Rep Gastroenterol 6(1): 135-142.
-
Harnden I, Walker R, Balmadrid B, Jiang X, Obando J, et al. (2015) Endoscopic Mucosal Resection of Duodenal Carcinoid Tumors: A Single Tertiary Care Center Experience. Gastroenterol Hepatol Open Access 3(2): 00075.
-
Wandhare T, Guerrero M, Madlinger R, Zuberi J (2020) A Rare Case of Duodenal Carcinoid Tumors in a Patient with Atypical Symptoms. Journal Of Current Surgery 10(1-2): 7-9.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma