Total Body Irradiation in the Era of New Radiotherapy Techniques
Total body irradiation (TBI), in combination with chemotherapy which is most often cyclophosphamide, is widely used since it was introduces in the fifties by E.D.Thomas as a preparatory regimen before bone marrow transplant. Even if it is an important part for conditioning regimen for patients with acute myeloid leukemia (AML) or acute lymphoid leukemia (ALL) undergoing hematopoietic stem cell transplantation, it is responsible for many side effects. New irradiation technique, tomotherapy and VMAT achieved a significant dose reduction to the OARs and the feasibility of dose escalation in a BMT conditioning regimen.
Introduction
Total body irradiation (TBI), in combination with chemotherapy which is most often cyclophosphamide, is widely used since it was introduces in the fifties by E.D.Thomas as a preparatory regimen before bone marrow transplant. It’s an important part for conditioning regimen for patients with acute myeloid leukemia (AML) or acute lymphoid leukemia (ALL) undergoing hematopoietic stem cell transplantation (HCT), usually allogeneic, to provide both immunosuppressive and cytotoxic effects [1]. TBI induces immunosuppression to prevent the rejection of donor marrow and aims to eradicate malignant cells in the same area that chemotherapy does, in sanctuary organs that are not reached by chemotherapy drugs, mainly the brain and testes [2].
Even though TBI is an efficient part of bone marrow transplantation conditioning treatment, it is responsible for many side effects. The most common acute toxic effects of TBI include parotitis, nausea and vomiting, dry mouth and mucositis, diarrhea, fatigue, decreased appetite, erythema, esophagitis, and alopecia. These toxic effects are usually transient and well manageable [2]. In the opposite, late effect such us cataract [3], gonadal failure , thyroid and kidney dysfunction, decreased bone mineral density , endocrine disorders, cardiometabolic traits and veno-occlusive disease and specially interstitial pneumonitis [4] are still challenging. As a result, more targeted forms of TBI are currently being evaluated in clinical trials using VMAT IMRT and helical tomographic IMRT.
In this article, we review the literature about TBI IMRT techniques in bone marrow transplantation.
Total Body Irradiation
Rational
TBI has traditionally been part of myeloablative conditioning regimens aimed to eradicate malignant cells , provide powerful means of immunosuppression and prevent rejection of donor hematopoietic cells. Unlike chemotherapy, delivery of radiation therapy (RT) to the tumor site does not depend on blood supply and is not influenced by variability in drug absorption, metabolism, biodistribution, or clearance kinetics [1]. It also had the advantage to reach sanctuary sites such as brain and testis.
Indications
Acute lymphoid leukemia (ALL) remains the main indication of a TBI based conditioning regimen in bone marrow transplantation [2], Current indications include patient achieving first remission with Philadelphia chromosome– positive disease, or in first remission with Philadelphia chromosome–negative disease with poor risk features; having disease that is refractory or does not respond to initial induction chemotherapy; being in remission after treatment for relapse; or having disease that remains refractory after relapse [1].
Other diseases, such as acute myelogenous leukemia (AML), chronic myeloid leukemia (CML), multiple myeloma (MM), and Hodgkin’s disease, might benefit from a TBI- based conditioning regimen, but the indications remain controversial [4].
Techniques
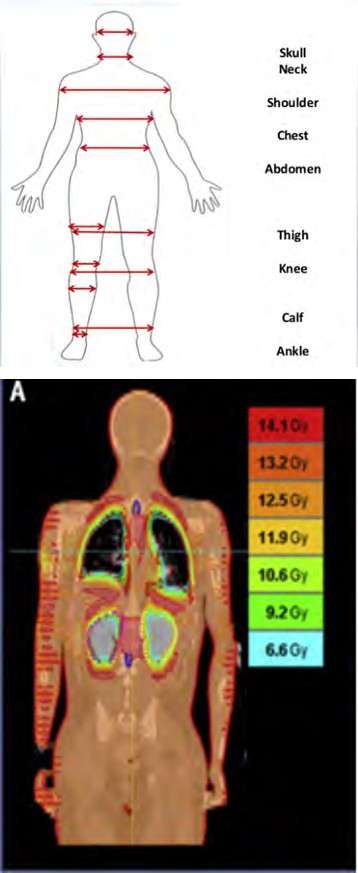
60C and linear accelerator based techniques were the first techniques of TBI that were described, and they are still widely used [5]. Measurements for planning purposes include the thickness, the distance from soles of the feet, and the distance from central axis at the following anatomic points: top of head, forehead, chin, suprasternal notch, xiphoid, umbilicus, central axis, pelvis, thigh, knees, calves, ankles, and toes. (Figure 1). Differences in separation along the patient’s length can result in dose heterogeneity that can exceed 10%-20%. The primary limitation of standard linear accelerators is the maximum field size of 40 × 40 cm at a standard source-surface distance (SSD). However, positioning patients at a superior SSD, generally 200–600 cm, allowed for an enlarging of the field size. If the size of the treatment room allows it, patients are treated by a single field. Otherwise, multiple fields are required.3 main categories can be described [4]: • Techniques using two opposite parallel anterior and posterior beams using one or two sources [6].
- Techniques using two opposite lateral beams where the shoulders play the role of compensator.
- Techniques using the combination of the two.
Intensity Modulated Radiotherapy in Bone Marrow Transplantation
Increasing numbers of centers have begun to use CT- based 3D planning, intensity modulated radiation therapy (IMRT), and inverse planning in an effort to improve dose uniformity and organ sparing. Soon after helical tomographic IMRT was introduced into the clinic, using it to deliver TBI with conformal avoidance of normal organs was proposed (Figure 2a, 2b)
Figure 2A: Conformal-avoidance TBI delivered with helical tomographic (tomotherapy).
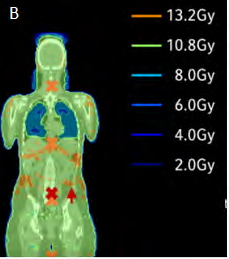
Figure 2B: Optimized VMAT-TBI plan.
Concept
The primary limitation of TBI is its toxicity to organs at risk, especially to the lungs, heart, liver and kidneys. In addition, Nevertheless, current accepted techniques of total body irradiation are laborious, time-consuming and cumbersome, and lead to significant acute and late toxicity due to the non-conformity of beam-application with the inability to individually spare organs at risk. The use of VMAT IMRT [7, 8], and helical tomographic IMRT [9, 10] are currently being evaluated as ways to deliver more targeted TBI.
TBI with Helical Tomotherapy
Penagaricano, et al. (2011); Gruen et al. (2013) s report the feasibility of TBI performed with HT. They both defined planning treatment volumes (PTV) as the whole body excluding organs at risk (OARs). In 2017, R. Suna, et al. published the First French experiences of total body irradiations using helical TomoTherapy. Total body irradiation consisted in a single fraction of 2 Gy. Planning target volume was divided in two due to the limited translation length of the table. Delivery quality assurance was performed with cylindrical phantom, ionization chamber and films. Planned V95% was covered by D95% and V2% did not exceed D107% for five of the six patients. The mean relative difference between measured and calculated absolute dose of the Delivery quality assurance was always less than 2.5%. This study showed that tomotherapy guaranteed high dose homogeneity throughout the body and dose verification was achievable, showing small difference between planned and delivered doses [11].
TBI with Volumetric arc Therapy (VMAT)
TBI with VMAT seems to provide significant decrease of the dose to OAR. Springer et al published in 2016 their study evaluating TBI with VMAT in 7 patient. It showed that using VMAT achieved reduction of the mean dose received by the lungs of 13–27%. In one patient, presenting with renal insufficiency, the mean dose to the kidneys has been reduced of 43–52%. Every patient suffered from grade 3 mucositis and one from bladder inflammation. With a mean follow- up time of 8 monts (2.3–15 months), one patient died from refractory disease, one from relapse and the five others live disease free [12].
limitations
The HT maximum field is limited to 60 × 160 cm which imposes a treatment in two parts for most of the patients. Most of the team have chosen to treat the upper body with HT and the lower body (limbs) with AP-PA fields, which leads to junction field uncertainties in the dosimetry calculation. Moreover, a recent case of radiation dermatitis has been reported and is an example of the uncertainties of the fields junction [13].
Treatment Duration
Nevertheless, TMI and TMLI request a long contouring time: 8 h for HT-TMI and 12–16 h for HT-TMLI. Studies report an average in-room time of 2 h, which could be decreased to 90 min with experience and a mean beam on time approximately 50 min [10].
Conclusion
Although TBI continues to be an important part of conditioning regimens for many patients, its use is declining for several possible reasons, including increased use of chemotherapyonly myeloablative conditioning regimens increased use of reduced-intensity conditioning regimens. The use of IMRT techniques allowed significant dose reduction to the OARs and feasibility of dose escalation in a BMT conditioning regimen. The outcomes of these irradiation techniques should be confirmed by the results of phase III trials.
References
-
Wong JYC, Filippi AR, Dabaja BS, Yahalom J, Specht L (2018) Total Body Irradiation: Guidelines from the International Lymphoma Radiation Oncology Group (ILROG). International Journal of Radiation Oncology Bio Phys 101(3): 521-529.
-
Paix A, Antoni D, Waissi W, Ledoux M P, Bilger K, et al. (2018) Total body irradiation in allogeneic bone mar- row transplantation conditioning regimens: A re- view. Crit Rev Oncol Hematol 123: 138-148.
-
Belkacemi Y, Labopin M, Vernant JP, Prentice HG, Tichelli A, et al. (1998) Cataracts after total body irradiation and bone marrow transplantation in patients with acute leukemia in complete remission: a study of the european group for blood and marrow transplantation. Int J Radiat Oncol Biol Phys 41(3): 659-668.
-
Belkacémi Y, Rio B, Touboul E (1999) Irradiation corporelle totale: techniques, dosimétrie et complications. Cancer/Radiothérapie 3(2): 162-171.
-
Giebel S, Miszczyk L, Slosarek K, Moukhtari L, Ciceri F, et al. (2014) Extreme heterogeneity of myeloablative total body irradiation techniques in clinical practice: A survey of the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation. Cancer 120(17): 2760-2765.
-
Brenfeman JC, Elson HR, Little R, Lamba M, Foster AE, et al. (1990) A technique for delivery of total body irradiation for bone marrow transplantation in adults and adolescents. Int J Radiat Oncol Biol Phys 18(5): 1233-1236.
-
Aydogan B, Yeginer M, Kavak GO, Fan J, Radosevich JA, et al. (2011) Total marrow irradiation with rapidArc volumetric arc therapy. Int J Radiat Oncol Biol Phys 81(2): 592-599.
-
Patel P, Aydogan B, Koshy M, Mahmud D, Irum K, et al. (2014) Combination of linear accelerator-based intensitymodulated total marrow irradiation and myeloablative fludarabine/busulfan: a phase I study. Biol Blood Marrow Transplant 20(12): 2034-2041.
-
Wong JYC, Liu A, Schultheiss T, Leslie P, Anthony S, et al. (2006) Targeted total marrow irradiation using threedimensional image-guided tomographic intensity- modulated radiation therapy: An alternative to standard total body irradiation. Biol Blood Marrow Transplant 12(3): 306-315.
-
Rosenthal J, Wong J, Stein A, Anthony S, Qian D, et al. (2011) Phase 1/2 trial of total marrow and lymph node irradiation to augment reduced-intensity transplantation for advanced hematologic malignancies. Blood 117(1): 309-315.
-
Sun R, Cuenca X, Itti R, Nguyen Quoc S, Vernant JP, et al. (2017) First French experiences of total body irradiations using helical TomoTherapy ®. Cancer/ Radiothér 21(5): 365-372.
-
Springer A, Hammer J, Winkler E, Track C, Huppert R, et al. (2016) Total body irradiation with volumetric modulated arc therapy: Dosimetric data and first clinical experience. Radiat Oncol 11: 46.
-
Takenaka R, Haga A, Yamashita H, Nakagawa K (2016) Adequate target volume in total-body irradiation by intensity-modulated radiation therapy using helical tomotherapy: a simulation study. J Radiat Res 58(2): 210-216.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma