Paraneoplastic Dermatomyositis Revealing Tardly an Ovarien Cancer at Metastatic Stage Who Responded Favorably to Treatment
Dermatomyositis is a type of inflammatory myopathy characterized by inflammatory and degenerative changes of the muscles and skin. The Para neoplastic dermatomyositis is a subtype associated with cancer. The pathophysiothogy remains unfully understood. The diagnosis is supported by both the clinical and serological features. The treatment involves both the DM and the malignancy. Multi-disciplinary management is fundamental for patients. However the pronosis remains usually poor. We report a case of Para neoplastic dermatomyositis revealing an ovarian cancer; the purpose is to illustrate the diagnostic, therapeutic and pronostic of this entity.
Background
Dermatomyositis is a form of auto immune inflammatory myopathy, with typical cutaneous characteristics and myositis-related impotence [1]. It includes juvenile and adult forms. Paraneoplastic dermatomyositis represents around 30% of adult dermatomyositis cases [2]. No clinical, histologic, or laboratory markers specific for paraneoplasic disease in DM have been identified to date [2]. The physiopathology shows an immune-mediated process causing by malignancy in genetically predisposed individuals [3]. Therapy is based on systemic corticosteroids and frequently on steroid-sparing immunosuppressive medicines, associated with the excision of the cancer. But new-targeted therapies may modify the treatment strategy in the near future. However the prognosis is still worse [3]. We report one case as an illustration of this paraneoplastic course revealing an ovarian cancer, and to make an update on the state of knowledge on paraneoplastic DM in such cancers.
A 76 years -old-woman with previous medical history of asthma and type 2 diabetes, was admitted to our hospital because of an persistant red rash on the face, present over many months. At the interrogation, the patient report other symptoms including fatigue; nostalgia, and chronic Arthritis. Physical examination shows a characteristic skin rash consist of a lilac-colored, reticulated, heliotrope-appearing rash on the upper eyelids. In addition, there is often erythema on the cheeks and over the shoulders and exposed upper chest (Figure 1). Erythematous, hyperkeratotic, scaly patches occur symmetrically on the extensor surfaces of the elbows, knuckles, and knees (Figure 2). Periungual hyperemia and telangiectasias was present (Figures 3 & 4). Gottron papules also exist, as violaceous papules; slightly elevated, and plaques over metacarpophalangeal joints, proximal and distal interphalangeal joints (Figures 3 & 4).

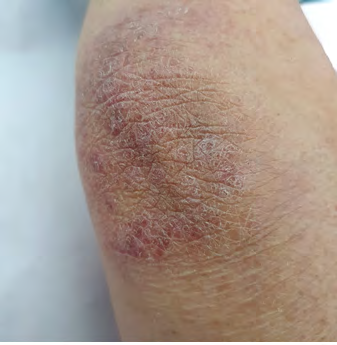


Figure 4: Periungual hyperemia and telangiectasia was present. Gottron papules are also existing and plaques over metacarpophalangeal joints, proximal and distal interphalangeal joints.
Also, the patient present asymmetrical weakness of proximal muscles of pelvic and shoulder girdle. The patient has difficulty getting out of chairs, the car, and bath; climbing stairs; reaching above the head, and dysphagia occurs. Laboratory findings were significant for an elevated serum creatinine phosphokinase (CPK) level of 399 U/L, creatine kinase isoform MB 369.7 ng/mL, aldolase 31.7 U/L, erythrocyte sedimentation rate 20mm/h, C-reactive protein 8.41 mg/L, lactate dehydrogenase (LDH) 804 U/L, ECG shows abnormalities incomplete right bundle branch block. Muscle biopsy shows perimysial and perivascular inflammation, perifascicular atrophy. TDM shows an ovary mass, peritoneal calcinosis, deep mediastinal adenopathies. The patient benefice of total excesses of the ovarian mass followed by chemotherapy sessions, with good regression of lesions.
Discussion
Dermatomyositis is an-auto immune connectivity. It has been recognized as clinical entity for more than 100 years [4]. But the first adult patients with dermatomyositis and malignancy were described early in the twentieth century, a causal association was proposed in the 1940s [4]. Studies show an increased risk of cancer in dermatomyositis patients, with standardized incidence ratios for neoplasm between 3.0 and 7.7 [2]. Predominantly affects females with sex ratio 1:3 in the fifthand sixth decades of life [3]. In the epidemiological study by Hill et al, 32% of DM was connected to malignant neoplasm of the ovary, lung, pancreas, breast or gastrointestinal tract or non-Hodgkin’s lymphoma [3]. The predominant malignancies associated with dermatomyositis are ovarian, breast and colon cancer, melanoma and non- Hodgkin’s lymphoma. Ovarian cancer was discovered in 8.3% of patients with dermatomyositis. Cancer isusually found simultaneously with or during the first year after the diagnosis of dermatomyositis although there continues to be an elevated risk of malignancy even after 5 years. Malignancies are usually identified through a history, physical exam, basic labs and/or age-appropriate screening tests. In women, a transvaginal ultrasound and CA 125 may be helpful to identify ovarian cancer.
In 1975,Bohan and Peter proposedfive criteria for their diagnosis, Symmetrical weakness of limb girdle muscles, elevated skeletal muscle enzyme levels myopathic pattern on EMG, muscle biopsy evidence of inflammation, and skin rash. Like other paraneoplastic phenomena, the pathophysiology of paraneoplastic dermatomyositis is thought to relate to autoimmune cross reactivity between similar autoantigens within the cancer tissue and normal tissue in muscle and skin [1]. Patients with malignancy associated dermatomyositis express a specific auto antibody pattern usually positive for anti–transcription intermediary factor 1-g (TIF1-g), anti-nuclear matrix protein (NXP-2) [3, 5, 6, 7]. Several clinical trial shows 80% of patients with cancer-associated dermatomyositis had antibodies against either TIF-1γ or NXP-2 [3, 5]. Histologically muscle biopsy shows an immune complex deposition at the dermal-epidermal junction. There is an indefinite quantity in CD4 T cell and B lymphocyte, and this inflammatory infiltrate is much more seen in the perivascular area. Capillary obliteration, fibrin thrombi and endothelial cell damage are markers of DM [3]. EMG shows prominent spontaneous activity (fibrillation potentials, positive sharp waves, and complex repetitive discharges). MUAPs are small, short, and polyphasic with early recruitment. The treatment of DM in a patient with cancer involves treating the DM and treating the malignancy. It is the same in patients with or without associated malignancy. The goal is to raise muscle strength and to improve extramuscular manifestations [3]. Treatment remains mostly empiric, using Topical emollients and steroids for all patients. If the tumor cannot be treated quickly and radically, the patient will require oral corticosteroids, and High-dose intravenous immunoglobulin has shown to be beneficial for recalcitrant DM [3]. Hydroxychloroquine is quite effective in about 80% of DM patients [3]. Immunosuppressors, such as methotrexate, azathioprine or cyclosporin, may be effective in inducing or maintaining remission. Most newly, rituximab, a monoclonal antibody directed against the surface antigen CD20 present on most B lymphocytes, has been recommended for use in DM [3]. The most widely accepted plan is to repeat the screening for cancer atonce a year for the first 3 years [2]. Regarding the management of paraneoplastic dermatomyositis, our aim must always be to control the underlying neoplasm [2, 6, 7].
Conclusion
Dermatomyositis is a disease of reputed autoimmune pathogenesis that presents with a symmetric, proximal, extensor inflammatory myopathy and a characteristic cutaneous eruption it is important for dermatologistto be aware in the work-up of dermatomyositis, that there may be an underlying rare cancer. This case emphasises that Early diagnosis of a cancer may provide the opportunity for curative surgical resection, and possible resolution of the dermatomyositis that heralded their disease.
References
-
Merry E, Smrke A, Halai K (2020) Paraneoplastic dermatomyositis associated with metastatic leiomyosarcoma of unknown primary. Clin Sarcoma Res 10(15).
-
Requena C, Alfaro A, Traves V, Nagore E, Llombart B, et al. (2014) Paraneoplastic Dermatomyositis: A Study of 12 Cases. Actas Dermosifiliogr 105(7): 675-682.
-
Chakroun A, Guigay J, Lusinchi A, Marandas P, Janot F, et al. (2011) Paraneoplastic dermatomyositis accompanying nasopharyngeal carcinoma: Diagnosis, treatment, and prognosis. Eur Ann Otorhinolaryngol Head Neck Dis 128(3): 127-131.
-
Jorizzo JL, Vleugels RN (2018) Dermatomyositis Dermatology 4th (Edn.), 42: 681-692.
-
Arnon J, Elia A, Nevo Y, Lossos A, Nechushtan H, et al. (2021) SCLC, Paraneoplastic Dermatomyositis, Positive Transcription Intermediary Factor 1-γ, and Point Mutation in the Transcription Intermediary Factor 1-γ Coding Gene: A Case Report. JTO Clin Res Rep 2(9): 100217.
-
Findlay AR, Goyal NA, Mozaffar T (2015) An overview of polymyositis and dermatomyositis. Muscle Nerve 51(5): 638-656.
-
Ofori E, Ramai D, Ona M, Reddy M (2017) Paraneoplastic Dermatomyositis Syndrome Presenting as Dysphagia. Gastroenterology Res 10(4): 251-254.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma