Impact of Covid on Duration Time of Treatment in Cervical Cancer
Duration Time of treatment (DTT) in cervical cancer is an essential prognostic factor. Longer treatment duration is the most unfavorable prognostic factor for local control. Objective: The main objective of this study is to investigate the impact of the pandemic on (DTT) in cervical cancer. Through a unicentric retrospective study carried out at the Radiotherapy department of the National Institute of Oncology, for 2 years, before and during the pandemic. Results: The number of patients followed before the pandemic was 138 and 157 during the pandemic. The average age before the pandemic was 54 and 53 during the pandemic. Squamous cell carcinoma accounted for 91% versus 9% adenocarcinoma. The average spread was 53 days before the pandemic, and 51 days during the pandemic. To facilitate patient care, a guest house has been made available to them. And a new system for programming and organizing brachytherapy was launched in July 2019, to control sprawl in these patients, and avoid its extension. Conclusion: Our study has made it possible to assess the impact of the pandemic on sprawling in our patients and the means to overcome the constraints of travel and organization for treatment within the optimal timeframe, in order to ensure a better local control.
Introduction
Cervical cancer is the fourth most common cancer in women, with around 604,000 new cases in 2020. Of the
342,000 deaths from cervical cancer in 2020, around 90% occur in countries with low or middle income [1, 2]. In Morocco, this cancer ranks second among women after breast cancer, according to the cancer registry of Rabat, for the year 2005-2009. In the majority of cases, the treatment is based on (external radiotherapy/External Beam Radiation Therapy (EBRT), (exclusive in the early stages and associated with chemotherapy in the locally advanced stages), followed by intracavitary brachytherapy (ICBT ) which is a cornerstone of its care [3]. In cancer of the cervix, spreading is an essential prognostic factor, compliance with which plays a key role in local control. Indeed, a longer duration of treatment has been shown to be the most unfavorable prognostic factor for local control (an overall duration of treatment greater than 56 days leads to a loss of 1% of local control per day) [1]. During the COVID-19 pandemic, containment measures may have impacted the use of patient care [4]. Thus, the objective of this work being to evaluate the respect of (DTT) during the pandemic in patients treated for cancer of the cervix receiving irradiation with curative intent in the radiotherapy department for a period of 2 years before and during the pandemic.
Material and Methods
This is a unicentric retrospective study conducted in the Department of Oncological Radiotherapy, at the National Institute of Oncology in Rabat; aimed at comparing the spread of patients treated for cervical cancer. Patients followed during the period from 2019 to 2021 for cervical cancer who received concomitant radio chemotherapy followed by brachytherapy were included. Patients followed for cancer of the cervix treated by surgery were excluded. Data from two separate time periods were compared: A first so-called “pre-pandemic” period which includes patient data between March 1, 2019 and March 1, 2020. A second period during the pandemic, where containment measures were put in place, grouping patient data between March 2, 2020 and March 31, 2021.
Data from patients seen in consultation for initial care in the radiotherapy department were collected continuously over the two periods. The data collected was:
- Age at first consultation
- The histological type
- The stage of the disease
- The therapeutic protocol
- The date of the start of treatment
- The date of the end of treatment
- Spreading
Data Analysis
The data collected was noted on an operating sheet then entered, stored and processed by SPSS25 and Excel 2013 software.
Results
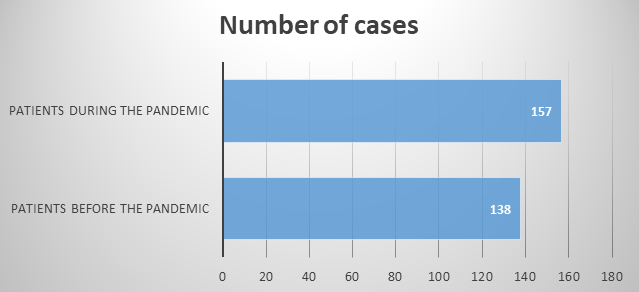
Number of Cases
In our study the number of patients admitted for cervical cancer before the Covid period of 2019-2020 was 138 while during the pandemic between 2020-2021, the number of patients was 157 with a total of 295 patients (Figure 1 & Table 1).
Age and histological types of patients followed before and during the pandemic
| Before Pandemic | After Pandemic | |
|---|---|---|
| Age | ||
| Average Age | 54 | 53 |
| Minimum | 28 | 94 |
| Maximum | 28 | 88 |
| History Type | ||
| Squamous Cell Carcinoma | 91% | 91% |
| Adenocarcinoma | 9% | 9% |
Table 1: Age and histological types of patients followed before and during the pandemic.
The Therapeutic Protocol The treatment received was external radiotherapy at a total dose of 46 Gy with a fractionation of 2 Gy per fraction associated concomitantly with weekly chemotherapy based on cisplatin at a dose of 40 mg/m2 followed by boost by utero- vaginal brachytherapy with protocol 7 Gy in 4 fractions.
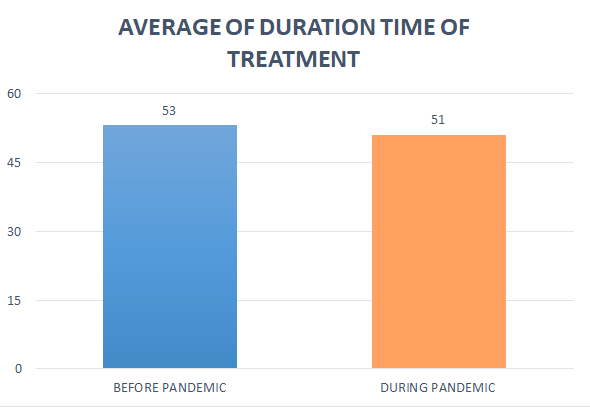
Duration Time of Treatment
The average spread before the Covid pandemic was 53 days with extremes between 31 and 88 days, while during the pandemic it was 51 days, with extremes between 31 days and 91 days (Figure 2).
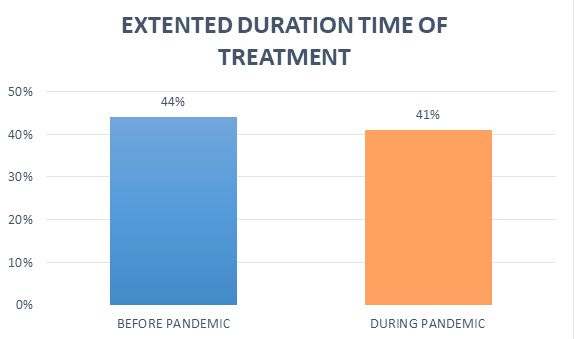
Spreading exceeded 56 days in 61 patients, i.e. 44% of cases before the COVID period, distributed as follows: 17% of patients received a 4-field supplement and 27% a supplement on the +/- ADP parameters while it was less than
56 days in 56% of patients.
While during the pandemic, the staggering exceeded 56 days in 66 patients, i.e. 41% of cases, distributed as follows: 14% of patients received a 4-field supplement, 27% a supplement on the parameters with or without ADP; against 59% of patients with spread of less than 56 days (Figure 3).
Discussion
In Morocco, cervical cancer is the second most common cancer after breast cancer in women according to the Rabat cancer registry for the period 2005-2009. It is the most common gynecological cancer in our country. In the majority of cases, the treatment is based on external radiotherapy/ External Beam Radiation Therapy (EBRT) (exclusive in the early stages and associated with chemotherapy in the locally advanced stages), followed by intracavitary brachytherapy (ICBT) which constitutes a cornerstone of its care [3]. The average age of onset is 47 years and about half of cases are diagnosed before the age of 35 [5]. However, in our series, the average age was 54 years, and nearly 85% of patients were diagnosed after the age of 40 years. The literature shows that squamous cell carcinoma is the most frequent histological type, and represents 80% of cases against 15% for adenocarcinomas [6]. In our study, squamous cell carcinomas represented 91% of cases while adenocarcinomas represented 9% of cases. Concomitant radio chemotherapy is the standard treatment for cancers of the cervix, locally advanced or localized with poor prognostic factors. The use of chemotherapy in combination with radiotherapy improves survival rates and local control [6, 7]. The total spread of the treatment is an independent factor influencing the prognosis [8, 9].
In our series, the average duration of treatment was 51 days before the COVID pandemic and 53 days during the pandemic, which remains acceptable compared to the references, being around 56 days [10]. Indeed, a longer treatment duration has been shown to be the main factor of poor prognosis for local control (an overall treatment duration greater than 56 days leads to a loss of 1% of local control per day) [1]. And in order to facilitate the care of our patients, and to avoid a long spread; a guest house has been made available to patients during their care, providing them with a home during their treatment period, thus overcoming the transport problems of patients with difficulty in accessing hospital structures. This structure remained functional even during the pandemic, contributing in part to respecting the duration of treatment and avoiding an extension. It should be noted that the Department of Radiotherapy of the National Institute of Oncology implemented in July 2019 a new system for programming and organizing brachytherapy in order to control the spread of patients treated for cervical cancer. uterus, and avoid prolonging the smear.
Several means have been used to organize the treatment planning of patients who are candidates for brachytherapy; and allow treatment within the optimal timeframe. In particular Excel files in which the names of patients scheduled for brachytherapy are noted, with the date of the first radiotherapy session; a pre-brachytherapy consultation is planned and carried out while the patient is still undergoing external radiotherapy, to assess the response and the feasibility of brachytherapy; and a pre- anesthetic consultation to assess eligibility for anesthesia. This, in order to avoid a long spreading, which was found in 44% of our patients before the pandemic and 41% during the pandemic period. Indeed, prolonging the spreading has a negative impact on local control via tumor repopulation [11]. And to limit the extension of the overall treatment duration, our department has tried to respect the time between EBRT and brachytherapy as much as possible. By several means including: A preference for schemes with a reduced number of fractions: 3×8 Gy or 4×7 Gy. In our unit we use the HDR ICBT scheme of 7 Gy per fraction for 4 fractions in 2 insertions 1 week apart. For each insertion, patients receive 2 fractions per day separated by an interval of 6 hours [12, 13]. For patients over the age of 70 or with significant comorbidities (chronic respiratory or cardiac disease, immunosuppression, etc.) who have small tumors or who respond well to external radiation therapy (EBRT), a shorter regimen of 9 Gy per split into 2 splits 1 week apart can be considered [14, 15]. The brachytherapy program is adapted by limiting the number of hospitalized patients, without compromising the length of treatment time. The problem that still arises is the delay in carrying out the supplement if necessary, especially since the patients lose their place in external radiotherapy once they have arrived at brachytherapy; hence the need to reprogram the patients again to benefit from additional parameters on the +/- ADP or 4 fields in the event of non-feasibility of brachytherapy.
A retrospective review evaluating the effect of overall duration of treatment (External Beam Radiation Therapy (EBRT) and brachytherapy) in cervical cancer (stages I to IV) noted a 1% decrease in local disease control for each day of delay beyond the median duration of treatment [16]. Similarly, various studies have noted an adverse outcome for cervical cancer patients whose duration of radiation treatment extended beyond 8 weeks (56 days) [10, 17]. Tanderup K, et al. [18] published data on 488 patients with locally advanced cervical cancer treated with chemo- radiotherapy followed by brachytherapy. A total treatment duration of 7-8 weeks is recommended for chemo-radiation therapy and brachytherapy. The Williams et al study, published in 2020, highlighted the impact of the pandemic on the spreading of cervical cancer with an extension of the duration of treatment, which has a negative impact on the local control. And in order to reduce spreading, this study proposed to use shorter fractionation schemes [19].
Conclusion
Staggering is a factor influencing the prognosis in cervical cancer. Its respect is essential for a good local control. The pandemic that the world had to face was responsible for a set of restriction and displacement measures that could have had an impact on this factor. Thus, this study was carried out, in search of the impact of the pandemic on spreading in patients treated for cervical cancer. Our study did not find any negative impact of the pandemic on Duration time of treatment in our patients. This can be explained in part by the logistical measures made available to patients, in particular the guest house which made it possible to alleviate to the constraint of travel to benefit from the treatment during the pandemic, as well as the new organizational system which compensated for the delay which occurred during the brachytherapy. On the other hand, the complement by external radiotherapy in 4 fields or in front of invaded parameters or envaded lymph nodes could be a source of delay, and must be taken care of in an optimal time in order to reduce the spread, thus ensuring good local control.
Conflicts of Interest
The authors declare no conflict of interest
References
-
Mazeron R, Castelnau MP, Dumas I, del Campo ER, Kom LK, et al. (2015) Impact of treatment time and dose escalation on local control in locally advanced cervical cancer treated by chemoradiation and image-guided pulsed-dose rate adaptive brachytherapy. Radiother Oncol 114(2): 257-263.
-
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, et al. (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71(3): 209- 249.
-
Elmajjaoui S, Ismaili N, El Kacemi H, Kebdani T, Sifat H, et al. (2016) Epidemiology and outcome of cervical cancer in national institute of Morocco. BMC Women’s Health 16(1): 62.
-
Gosset M, Gal J, Schiappa R, Dejode M, Fouche Y, et al. (2020) Impact of the COVID-19 pandemic on treatment for breast and gynecological cancer, Bulletin du Cancer.
-
Wagoner SE (2003) Cervical cancer. Lancet 361(9376): 2217-2225.
-
Morris M, Eifel PJ, Lu J, Grigsby PW, Levenback C, et al. (1999) Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high- risk cervical cancer. N Engl J Med 340(15): 1137-1143.
-
Fyles AW, Pintilie M, Kirkbride P, Levin W, Manchul LA, et al. (1995) Prognostic factors in patients with cervix cancer treated by radiation therapy: results of a multiple regression analysis. Radiother Oncol 35(2): 107-117.
-
Saibishkumar EP, Patel FD, Sharma SC, Karunanidhi G, Ghoshal S, et al. (2006) Prognostic value of response to external radiation in stage IIIB cervix cancer in predicting clinical outcomes: a retrospective analysis of 556 patients from India. Radiother Oncol 79(2): 142- 146.
-
Perez CA, Grigsby PW, Castro VH, Lockett MA (1995) Carcinoma of the uterine cervix. I. Impact of prolongation of overall treatment time and timing of brachytherapy on outcome of radiation therapy. Int J Radiat Oncol Biol Phys 32(5): 1275-1288.
-
Petereit DG, Sarkaria JN, Chappeli R, Fowler JH, Hartman TJ, et al. (1995) The adverse effect of treatment prolongation in cervical carcinoma. Int J Radiat Oncol Biol Phys 32(5): 1301-1307.
-
Allam A, Perez LA, Huang P, Taghian A, Azinovic I, et al. (1995) The effect of the overall treatment time of fractionated irradiation on the tumor control probability of a human soft tissue sarcoma xenograft in nude mice. Int J Radiat Oncol Biol Phys 32(1): 105-111.
-
Elledge CR, Beriwal S, Chargari C, Chopra S, Erickson BA, et al. (2020) Radiation therapy for gynecologic malignancies during the COVID-19 pandemic: international expert consensus recommendations. Gynecol Oncol 158(2): 244-253.
-
Williams VM, Kahn JM, Harkenrider MM, Chino J, Chen J, et al. (2020) COVID-19 impact on timing of brachytherapy treatment and strategies for risk mitigation. Brachytherapy 19(4): 401-411.
-
Patel FD, Rai B, Mallick I, Sharma SC (2005) High-dose- rate brachytherapy in uterine cervical carcinoma. Int J Radiat Oncol Biol Phys 62(1): 125-130.
-
Novetsky AP, Einstein MH, Goldberg GL, Hailpern SM, Landau E, et al. (2007) Efficacy and toxicity of concomitant cisplatin with external beam pelvic radiotherapy and two high-dose-rate brachytherapy insertions for the treatment of locally advanced cervical cancer. Gynecol Oncol 105(3): 635-640.
-
Fyles A, Keane TJ, Barton M, Simm J (1992) The effect of treatment duration in the local control of cervix cancer. Radiother Oncol 25(4): 273-279.
-
Song S, Rudra S, Hasselle MD, Dorn PL, Mell LK, et al. (2013) The effect of treatment time in locally advanced cervical cancer in the era of concurrent chemoradiotherapy. Cancer 119: 325-331.
-
Tanderup K, Fokdal LU, Sturdza A, Haie MC, Mazeron R, et al. (2016) Effect of tumor dose, volume and overall treatment time on local control after radiochemotherapy including MRI guided brachytherapy of locally advanced cervical cancer. Radiother Oncol 120(3): 441-446.
-
Williams VM, Kahn JM, Harkenrider MM, Chino J, Chen J, et al. (2020) COVID-19 impact on timing of brachytherapy treatment and strategies for risk mitigation. Brachytherapy 19(4): 401-411.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma