Thyroglobulyn in Pleural Effusion in Metastasic Papillary Thyroid Cancer
We report case of massive pleural effusion caused by papillary thyroid cancer, which was accompanied by multiple pulmonary metastasis. A 60‑year‑old female patient presented with shortness of breath and cough due to massive left pleural fluid. Since cytological and cytochemical studies were not conclusive for the primary tumor, and the measurement of thyroglobulin washout has been recommended as a complementary study in suspicious cervical lymph nodes, we performed it using the cut- off points used in cervical lymph nodes.
Introduction
Papillary thyroid cancer (PTC) is the most common malignant neoplasm of the thyroid [1], it has an excellent prognosis and a 10-year survival of 95% [1, 2]. Most PTCs are indolent and do not recur nor metastasize after resection and treatment with radioiodine, even in the presence of metastases in cervical lymph nodes1. At the time of diagnosis, lymphatic metastases can be found in 50-60% of cases and distant metastases in 7-23% [3], being the most frequent sites lung where it manifests as multiple small bilateral nodules [4], and bone. In rare cases, it can metastasize to the pleura and manifest as a malignant pleural effusion (MPE), and it portend a poor prognosis [1]. The physical characteristics of MPEs do not allow distinguishing between PTC and other malignant causes since they usually correspond to exudates. Cytology is important for differential diagnosis as well as immunohistochemistry and immunostai\ning, which is positive only in differentiated thyroid cancer (DTC) [5, 6].
Objective
Report a case of the use of thyroglobulin measurement in aspiration needle washout (TgW) in pleural effusion in metastatic PTC.
Clinical Case
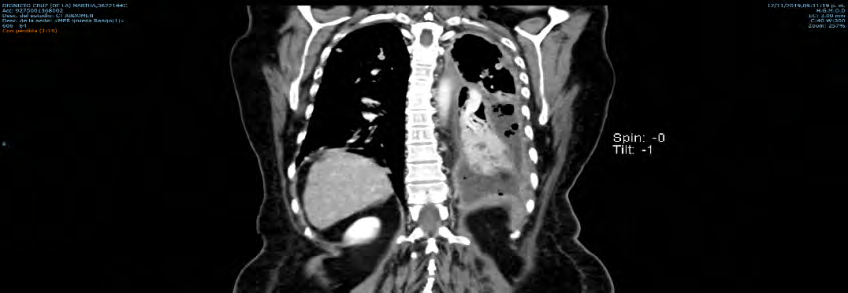
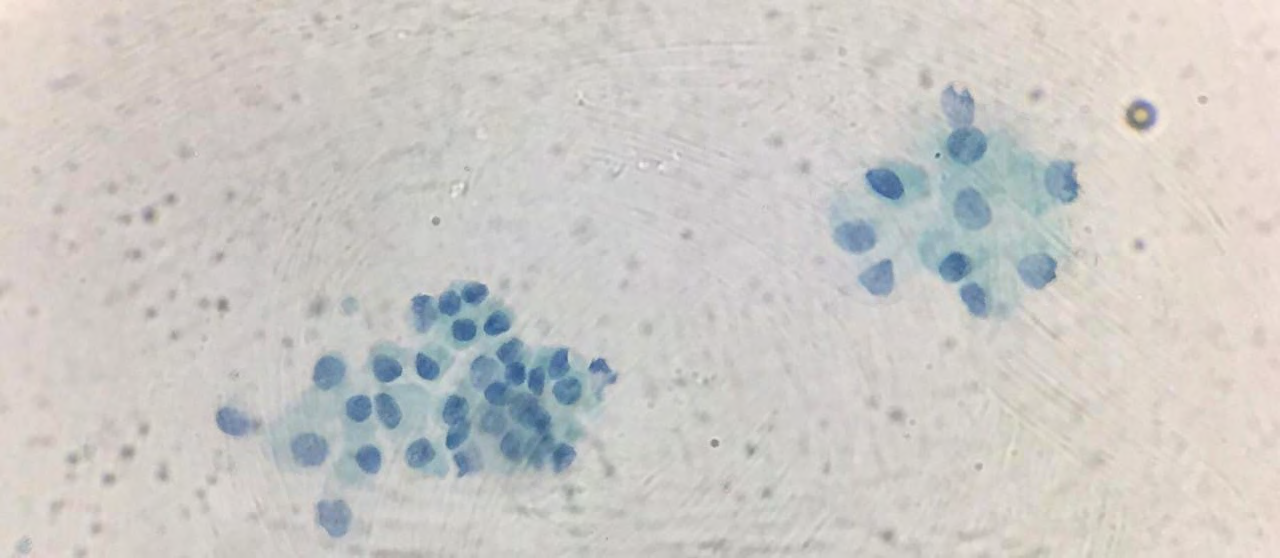
60-year-old female who underwent total thyroidectomy plus lateral neck dissection for PTC in July 2019, reporting classic variant of papillary carcinoma (multifocal tumor, size: 6x 4x 2 cm, extrathyroid extension: present, lymphovascular invasion: present, 23 lymph nodes were dissected with the presence of neoplastic cells in 14); ATA [7] high risk, AJCC [8] stage IV A; undergoing treatment with levothyroxine sodium 100 mcg/ daily and calcium and calcitriol supplements for postsurgical hypoparathyroidism. Iodine 131 ablation was indicated according to the NCCN guidelines [9], but it was pending at the time of her hospitalization. She was admitted by the pneumology service in October 2019 due to shortness of breath and cough of 2 weeks of evolution. On physical examination with hypoventilation, dullness and decreased vocal vibrations in the left lung field. Chest X-ray: left pleural effusion of approximately 70% (Figure 1), for which an endopleural tube was placed. Chest CT scan revealed a left pleural effusion, with multiple nodules in the right lung and mediastinum (Figure 2). Blood test: TSH 55.46 mIU/ml, FT3 2.19 pg/ml, FT4 0.43 ng/dl, Tg 4955.36 ng/ml, Tg Ab 0 IU / ml. Hormonal replacement with levothyroxine sodium was adjusted to 175 mcg/ daily. Pleural fluid studies: TgW>
24450 ng/ ml, cytochemistry compatible with exudate and cytological positive for malignant cells, without specifying details of cellularity (Figure 3).

Discussion
The main causes of MPE are metastatic lung carcinoma, breast cancer, ovarian cancer, cancer of the upper digestive tract, mesothelioma and lymphoma [1, 6]. PTC is only responsible in <0.6% (50 cases reported) [5, 6], its diagnosis represents advanced systemic disiease with low survival rate (<10 months) and poor quality of life. MPE´s physical characteristics do not allow distinguishing between malignant causes. The differential diagnosis of PTC and other causes of MPE depends on the presentation of all the typical cytomorphological characteristics of DTC, which are usually not appreciated if the cause of the metastasis to the pleura is a poorly differentiated or anaplastic thyroid cancer [5];
and the use of auxiliary studies (TTF-1, PAX8, napsin- 2 and thyroglobulin) [1, 5, 6].
TgW in lymph nodes was proposed since the cytopathological diagnoses of these may be inadequate or inconclusive [10]; even the ATA [7], ETA [11] and AACE [12] guidelines have recognized its importance and recommend including it in the complementary evaluation with fine- needle aspiration biopsy of the suspicious cervical lymph nodes [10]. TgW offers the advantage that, even if epithelial cells are not found in the aspirate, Tg may be elevated both inside and outside the lesion. A Tg value greater than 10 ng/ml has been taken as highly indicative of disease [10, 13]. To date, the use of TgW has only been described in lymph nodes [10, 13]. The cytochemical and cytological studies in our case were not definitive for PTC. Considering that no complementary immunocytochemical studies were made, we performed a TgW of the pleural fluid using the same cut-off values for the interpretation described for the measurements for TgW of lymph node, since there is no cut- off values described for pleural fluid, considering the value obtained in this case with a positive result as compared to those applied for cervical lymph nodes. Leaving no doubt metastasic involvement related to the primary tumor and demonstrating that, given its measurement is readily available, it can be used for the complementary evaluation in patients with history of DTC who have suspected tumor activity, however, it will be necessary to work in the establishment of cut- off values for its best interpretation.
Conclusion
TgW is a useful tool for the diagnosis of lymph node metastatic disease in PTC, which can also be applied for the evaluation of the presence of metastasic activity in other organs or tissues.
References
-
Kosmas K, Tsonou A, Mitropoulou G, Salemi E, Kazi D, et al. (2017) Malignant pleural effusion from papillary thyroid carcinoma diagnosed by pleural effusion cytology: A case report. Diagnostic Cytopathology 46(2): 204-207.
-
Tomoda C, Ogimi Y, Saito F, Masaki C, Akaishi J, et al. (2016) Outcome and characteristics of patients with malignant pleural effusion from differentiated thyroid carcinoma. Endocrine Journal 63(3): 257-261.
-
Vyas M, Harigopal M (2016) Metastatic Thyroid Carcinoma Presenting as Malignant Pleural Effusion A Cytologic Review of 5 Cases. Diagnostic Cytopathology 44(12): 1085-1089.
-
Tamura T, Shiozawa T, Satohi H, Kurishima K,Kagohashi K, et al. (2019) Pleural fluid due to papillary thyroid cancer. Oncology Letter 18(1): 962-966.
-
Lew M, Pang JC, Roh MH, Jing X (2015) Cytologic Features and Immunocytochemical Profiles of Malignant Effusions with Metastatic Papillary Thyroid Carcinoma: A Case Series from a Single Institution. Acta Cytologica 59(5): 412-417.
-
Olson MT, Nuransoy A, Ali SZ (2013) Malignant Pleural Effusion Resulting from Metastasis of Thyroid Primaries: A Cytomorphological Analysis. Acta Cytologica 57(2): 177-183.
-
Haugen BR, Alexander EK, Bible KC, Doherty G, Mandel SJ, et al. (2016) 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid 26(1): 1-133.
-
Tuttle M, Morris LF, Haugen B, Shah J, Sosa JA, et al. (2017) Thyroid‐Differentiated and Anaplastic Carcinoma (Chapter 73). In: Amin MB, Edge SB, Greene F, Byrd D, Brookland RK, et al. (Eds.), AJCC Cancer Staging Manual. In: 8th (Edn.), Springer International Publishing, New York City, USA.
-
National Comprehensive Cancer Network. Thyroid Carcinoma (Version 1.2021).
-
Degertekin CK, Yalcin MM, Cerit T, Ozkan C, Kalan I, et al. (2016) Lymph node fine-needle aspiration washout thyroglobulin in papillary thyroid cancer: Diagnostic value and the effect of thyroglobulin antibodies. Endocrine Research 41(4): 281-289.
-
Leenhardt L, Erdogan MF, Hegedus L, Mandel SJ, Paschke R, et al. (2013) 2013 European thyroid association guidelines for cervical ultrasound scan and ultrasound- guided techniques in the postoperative management of patients with thyroid cancer. Eur Thyroid J 2(3): 147- 159.
-
Gharib H, Papini E, Garber JR, Duick DS, Harrell RM, et al. (2016) AACE/ACE/AME task force on thyroid nodules. American association of clinical endocrinologists, American college of endocrinologist, and associazione medici endocrinologi. Medical guidelines for clinical practice for the diagnosis and management of thyroid nodules - update. Endocr Pract 22: 622-639.
-
Trimboli P, Daurizio F, Tozzoli R, Giovanella L (2017) Measurement of thyroglobulin, calcitonin, and PTH in FNA washout fluids. Clin Chem Lab Med 55(7): 914-925.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty