An Update on Fertility Preservation in Men Undergoing Cancer Treatment, Irrespective of Age-A Comprehensive Review
Cancer in addition to the correlated radiotherapy, along with chemotherapy, possesses significant deleterious actions on the male reproductive capacity, resulting in a lot of men infertile. Fertility preservation has become a critical issue with regards to survivors in the last 2 decades, with a lot of professional organizations, have published literature with regards to the guidelines that advocate fertility preservation to assume a routine part of dealing with an man who is supposed to receive cancer treatment. Maximum males possess the capacity of generation of an ejaculate having sufficient semen specimen for fertility preservation by cryopreservation of sperms. Despite different other approaches for collection of sperms are existent certain patients like adult males with azoospermia, besides, prepubertal, boys who do not have the initiation of spermatogenesis, one can’t harvest the sperms, besides all the advances of cryopreservation of testicular tissue cryopreservation, yet translation to adult sperms has not got attained with lot of efforts being directed towards attaining same by particular metabolism manipulation of immature germ cells, besides use of various factors like VEGF &PDGF laden nanoparticles. Thus lot of experimental, besides investigational strategies, give the hope that translation to Clinical scenario that will provide extra pathways In achieving successful fertility preservation.
Introduction
The incidence, of cancer has escalated markedly, which represents a heterogenous disorder with about 50% of men generating over their lifetime. In the form of a disease event cancer in addition to treatment of the same might result in battling with a lot of side actions. Dysfunction In the reproductive health being one of these harmful actions, that is associated with infertility, is what these men will usually encounter, besides marked stress, depression, anxiety in addition to poor quality of life [1, 2]. Secondary to that fertility has become a significant issue that gets correlated with the subjects who survive in this oncology field over the span of the last 2 decades.in this article subsequent to our initial review of fertility preservation advances, that was inclusive of testicular tissue transplantation along with in vitro Spermatogenesis in case of animals, with minimal human experiences, besides, VSELs here we have tried to update the influence of cancer on male fertility preservation, that is inclusive of, the influence of cancer therapies on male fertility, advocated guidelines, results derived from the cryopreservation of sperms from patients with cancer, besides discussion of the stem cell technology that might create a revolution in the field of reproductive medicine [3, 4].
With the fast pace in clinical along with basic sciences details on fertility preservation this would be of use to clinicians, in addition to those from laboratory besides basic science researchers.
Methods
Thus here we conducted a systematic review utilizing search engine pubmed, google scholar and othersutilizing the MeSH terms like fertility preservation; male cancer; hormone modulates ; radiotherapy; chemotherapy; prepubertal boys; Spermatogonial Stem Cells Induced pluripotent Stem Cells(iPSCs); Testicular Tissue Transplantation; Semen cryopreservation; In vivo Spermatogenesis; VEGF- nanoparticles; VEGF-nanoparticles+PDGF-nanoparticles; NECINH-nanoparticles, Testicular organioid generation from 1975 to 2021 till date.
Results
We found a total of 1050 articles out of which we selected 101 articles for this review. No meta-analysis was done.
Influence of Cancer on Male Reproduction
Pretesticular Action of Cancer on Male Reproduction: Hypothalamic-Pituitary-Goadal (H-P-G) Axis
The physiology correlated with male reproduction is robustly dependent on the normal intact hypothalamic -pituitary-Goadal (H-P-G) Axis. Structural integrity is significant In view of direct structural injury that is secondary to any tumour, whose manifestation might be as a mass action (causing compression) or via the infiltration by tumour of the surrounding anatomical structures that were normal from an anatomical point of view. Besides that systemic inflammation usually exists in the cancer subjects, which might possess deleterious action on the normal hypothalamus. This specific hypothalamic inflammation might result in a lot of endocrine alterations that result in a reduction of appetite, in addition to decrease of lean body mass, that is usually correlated with association with the presence of any oncologic entity [5], that is known as’’ anorexia cachexia syndrome’’ as well as is usually secondary to systemic inflammation, that is seen usually In association with a cancer diagnosis. The mode implicated is of 2 types i) hypothalamic interleukin-1β ( IL-1β), that influences the hypothalamic -pituitary-adrenal axis, resulting in enhancement of liberation of GC’s that leads to activation in ubiquitin-proteasome pathways as well as escalation of catabolism. ii) up regulation of hypothalamic serotonin pathways that cause changed orexigenic in addition to anorexigenic response leading to reduction in food ingestion. These 2 modes in combination cause lot of alterations in the properties of anorexia cachexia syndrome’’ that is inclusive of fertility dysfunction.
Testosterone (T), i.e., a crucial controller of the reproduc- tive health, a reduction is usually observed In the T in men who presented with cancer [6]. The generation of anorexia cachexia syndrome’’ that occurs secondary to both systemic along with hypothalamic inflammation has got correlated with the lower T concentration. Escalation of IL-6 in addi- tion to C Reactive Protein(CRP) concentration are observed in men who manifest with cancer, in association with aber- rantlly low serum T concentration, besides cachexia in con- trast to men without cancer [7]. Moreover, in patients with cancer in addition to cachexia possess a greater prevalence of signs with symptoms associated with the deficit of T, that is inclusive of lesser grip strength, erectile impairment, and lesser functional status in addition to escalation of fat mass in contrast to other2 groups [7]. Certain scientists have advo- cated inflammation associated treatment for amelioration of these inflammation correlated alterations. In view of the key part which T possesses with regards to spermatogenesis, it is possible that deficiency of T possesses a minimum part in the reduction in the sperm parameters, an observation common- ly encountered when the cancer diagnosis is made [8]. Be- sides impacting spermatogenesis is, lesser T can further re- sult in reduction of libido in addition to erectile dysfunction, hence sexual function in addition to reproductive capacity is interfered with.
Testicular Influences of Cancer on Reproduction
Implications on fertility via direct influence on the testis, in cases of primary testicular cancer in addition to less often testicular tumor metastasis from other areas of body is usually visualised. Furthermore local damage of the testicular tissue can be initiated by the tumors that result in normal parenchyma getting replaced with the neoplastic cells. In case of big tumors in addition to tumors that are placed at the superior part In the testis can in theory obstruct or replace the rete testis in addition to the efferent tubules, thus possessing the chances of intra testicular blockade of the transit of sperm to the epidydimis.
This neoplastic tissue might possess endocrine in addition to paracrine actions that exist within the testicular microenvironment. Testicular cancer cells possess the capacity of liberation of hormones like β human chorionic Gonadotropins (βHCG) as well as α fetoprotein, both of which have got correlated with spermatogenesis [9]. Monish, et al. [10] conducted a static along with dynamic evaluation of the HPG axis in addition to endocrine and paracrine function whose outcomes pointed that βHCG that gets liberated by tumor cells can result in stimulation of normal ipsilateral or contralateral testicular parenchyma for the liberation of estradiol (E2) that might result in impairment of spermatogenesis. It has been an observation that escalation of the ghrelin in addition to IL-6 concentration have been correlated with aberrant T generation. A cross sectional study performed by Garcia, et al. [6], observed escalation of ghrelin as well as IL-6 in cancer patients in contrast to the controls. Escalation of Luteinizing hormone (LH) concentrations got demonstrated with reduction of free T In such patients, that points to a partly compensated hypogonadism, which might partly be secondary to interference of the generation of testicular T by ghrelin or IL-6.
Besides hormonal alterations the observation of immune in addition to inflammatory reaction commonlyobserved in cancer possesses the capacity of impairment of spermatogenesis [11]. The histologic alterations usually seen are inclusive of lymphocytes in addition to plasmacytic infiltration, along with granulomatous alterations, specifically in case of patients with seminoma. The leukocyte in flux in addition to correlated liberation of cytokines can result in destruction of germ cells, sertoli cells along with leydig cells that is associated with a total impairment of the micro anatomical structure of the testis
Post Testicular Influences of Cancer on Reproduction in Males
The one more mode by which cancer impairs function of reproduction occur secondary to the disturbance In the normal transportation of sperm from the testis to the vagina at the time of coitus. This event of ejaculation, the liberation along with expulsion of semen via the penis, can get implicated by either neurologic dysfunction or mechanical blockade. Ejaculatory function needs an intact neurologic input through the spinal ejaculation center, which is existent below the 10th thoracic area (T10) in addition to the supporting nerves [12]. In case the tumor impinges directly or infiltrates these structures can result in partial ejaculation, anejaculation, retrograde ejaculation or aspermia. Furthermore tumors can impact the structures which transport sperm from the testis towards the tip of the penis at the time of coitus, causing mechanical blockade. The epididymus, vas deferens, ejaculatory duct might get impacted by the disturbance in the male excurrent ductal system, besides disruption of the fertility capacity. In view of bilateral excurrent ductal system in men there would be a requirement of bilateral impact for the generation of azoospermia in a man.
Influences of Cancer on Treatment of Male Reproduction
Cancer therapies are inclusive of radiotherapy, medical therapy (chemotherapy, hormone modulators, mammalian target of rapamycin inhibitors (mTOR), monoclonal antibodies, as well as tyrosine inhibitors) along with surgical therapy. These treatments can get administered solely or in different combinations. Every treatment strategy possesses particular toxicities, a lot of which might cause secondary robust negative impact on the male reproductive health.
Medical Therapy
Chemotherapy: Chemotherapy is the biggest group of the medical therapies whose utilization is done for the treatment of cancer. These drugs target the neoplastic growth in addition to proliferation of cancer cells In a lot of ways along with their classification is done as per the mode of action. Like the classes of chemotherapeutic drugs are inclusive of alkylating agents, anti-metabolites, anthracyclins, platinum –dependent drugs, plant alkaloids, topoisomerase inhibitors. Modes utilized by these drugs are inclusive of interference with DNA transcription along with generation, hampering of microtubule generation in addition to cross linking of DNA. Usually chemotherapeutic drugs get grouped as high, medium as well as low risk dependent on the chances of impacting the spermatogenesis in addition to male fertility. The injury, which any agent results in is based on besides the utilization of the specific drug, along with the dose got in addition to the age as well as sex of the patients [13].
In maximum chemotherapeutic protocols, a lot of agents utilization is done for obtaining the maximum effectiveness with the utilization of a multitargeted strategy for using the least doses of each agent besides there, toxicity in addition to side actions. In view of utilization of a lot of agents that possess separate toxicities it might become tough to evaluate the probable toxicities of every particular protocol correctly [13, 14, 15, 16, 17]. The researchers have been studying the properties that are implicated in reproductive toxicity of the chemotherapy whose utilization is dependent on this alkylating agent that possesses robust toxicity, further that is dependent on the maximum spermatotoxic alkylating agent [18]. Protocols that possess greater cyclophosphamide equivalent dose, get correlated with the escalation In the chances of generation. Inspite of these results in addition to tools that aid every patient would possess chances of an individual risk description secondary s to his chemotherapeutic protocols, dosage, burden of the cancer, which makes it tough with regards to anticipation of the chances of generation of dysfunctional fertility in a separate patient.
Hormone Therapy: The Hormone therapies for men are inclusive of gonadotropin releasing hormone (GnRH) agonist in addition to antagonist, along with antiandrogenic drugs that block androgen receptor binding [19]. these specific particular agent whose utilization is maximum done for the therapy of prostate cancer, classically cause significant or total repression of spermatogenesis [20]. Despite these side actions on reproductive function of maximum of these agents are reversible on stoppage of therapy, their long term utilization possesses the capacity of hypogonadism, in addition to azoospermia.
Mammalian Target of Rapamycin Inhibitors (Mtor), Monoclonal Antibodies, as Well as Tyrosine Kinase Inhibitors: During the last decade, an enhancement of the numbers of agents that belong to the mammalian target of rapamycin inhibitors (mTOR) monoclonal antibodies, as well as tyrosine kinase inhibitors have got utilized for the cancer therapy in the clinical scenario. What is astonishing is that hardly any preclinical or postmarketing results were done with regards to the particular reproductive actions of these different drugs despite a small series that have got published. Like Scovell, et al. [21], conducted the evaluation of the autopsy specimens that were obtained from men having immune checkpoint inhibitors for malignant melanoma, where they found disturbance in spermatogenesis in their testis. Since at an escalating rate these agents have been believed to become necessary within the standard protocols whose utilization for treatment of various malignancies, a lot of need is there to estimate their impact on the reproductive, capacity.
Radiation Therapy
Radiation therapy is a must in the treatment of cancer, where ionizing radiation tries to target the rapidly proliferating cancer cells in the influenced organs. Secondary to this the other nonmalignant cells that are also rapidly proliferating might get injured that adds significantly to the toxicity contributed [14, 15, 16, 22]. In the testis, the spermatogonial differentiation, that represent the cells undergoing proliferation at the maximum fast pace as well as thus the ones possessing the highest chances of sustenance of actions of the ionizing radiation. As compared to that the gametes that are differentiated possess lesser risks of sustenance of radiation toxicity. This explains the reason of observation of sperms within the ejaculate for various mths following the starting of the radiation treatment, in view of the differentiated sperms possess lesser susceptibility as these differentiated sperms finish the event of spermiogenesis [14]. The least concentration of semen parameters classically take place a little later in men that are receiving radiation therapy as compared to the ones getting systemic chemotherapeutic agents [15].
The spermatogenesis getting recovered is based on a lot of factors, that is inclusive of, the dosage of radiation ii) if fractionation of therapy done, or not iii)age of the patient [15]. Doses to the testis >2.0Gy usually causes azoospermia, while doses of 0.8-2.0 Gy in permanent oligozoospermia, as well as <0.8Gy in transient oligospermia for patients with seminoma treated with radiotherapy [23]. Hence in the ejaculate return of sperms is based significantly on the spermatogonial stem cells survival from their radiation dosages, besides populating the test is once again. Intriguingly, despite survival of these spermatogonia, infertility might still result secondary to injury of the somatic testicular environment, which can disturb the spermatogonial differentiation [24].
Surgical Therapy
Cancer patients undergo a wide type of Surgeries for attaining cure/just with aim of palliation. Any kind of surgery by which the hypothalamus or the –pituitary can get influenced can directly cause hypogonadotropic hypogonadism besides result in repression of spermatogenesis. In the surgeries where part/total testis removal is implicated, then they end up in depletion of germ cell mass in addition to the lending cell mass, hence badly impacting fertility.
Possession of an intact spinal ejaculation center that is correlated with peripheral retroperitoneal nerves are necessary for the innervations of a lot of muscles in addition to other structure that are implicated in seminal emission along with ejaculation. In case this functional anatomy disturbance takes place at the time of surgery, there can be destruction of normal fertility that is usually visualized in cases following retroperitoneal lymph node dissection in case of testicular cancer, though any kind of cataclysmic pelvic surgery might injure these key neurological structures [25]. Lastly the excurrent ductal systems that are inclusive of efferent ductules, epididymides, in addition to vas deferens, besides the prostatic ejaculatory duct as well as urethra, all are required to be open in addition to possess sustenance of the normal continuity that aids In efficacious deposition of sperm out of the tip of the penis at the time of sexual climax. A lot of these structure are remarkably small in addition to vulnerable to iatrogenic damage along with post-operative inflammatory along with fibrotic alteration that results in stenosis or atresia if their existence is in or near the operative field.
Any surgery that impacts these significant anatomical structures possesses chances of creating fertility disturbance. Thus a detailed preoperative strategy needs to discuss the capacity of causing risk, besides what is the anticipation of the patient.
Fertility Preservation Guidelines
Over decades we have concentrated in the field of oncology mainly to obtain cure of cancer in addition to survival of the patients along with excluding a lot of other probabilities of early along with late treatment action. Reproductive dysfunction in the male cancer patient was acceptable as a side effect of a lot of cancer treatment protocols, with a big lot numbers of patients who survived over their cancer, subsequently lost ability for biological fatherhood. Over the last lot of decades a convergence of alterations have taken place that has allowed a switch in this prototype. The biggest reason for the alterations is significant escalation in cancer diagnosis in addition to treatment, which has led to a marked enhancement in survival rates of men who are in the reproductive age. As per this the most recent surveillance in addition to epidemiology end outcome data, documented that the 5yr survival rate amidst men among 15-39 yrs old who had been diagnosed with cancer is 81.2% [26]. Despite an enhancement of the new cancer rates amidst this cohort by about o.4%/yr among 2008-2017, the death rate reduction occurred by about 0.8%/yr among 2009- 2018.The escalation of these advantageous survival rates are secondary to escalation in cancer treatment. With the maximum of men among 15-39 yrs old having survivorship, then other situations like fertility besides sexual function have assumed greater significance at the time of making a plan for the treatment of cancer as per the stages for both physician in addition to the patients.
Of the first guidelines that gave the clinical outlines with regards to fertility preservation was provided by the Ethics Committee of the American Society of Reproductive Medicine. They detailed the various significance, besides ethical problems in the context of reproduction with regards to diagnosis of cancer [27]. In 2006 itself the: fertility preservation guidelines were provided by the American Society for Clinical Oncology on fertility preservation in cancer patients [28]. They advocated for arriving at a diagnosis of cancer to keep these issues in detailing the capacity for infertility in cancer patients of reproductive age just following the diagnosis of cancer is made, besides prior to the starting of treatment for cancer ii) discuss the fertility preservation methods that are available iii) besides referring the patients to a person who has the qualification for the same if patient displays interest. Woodruff, et al. [29]. In 2006 itself used the term Oncofertility for which In 2007 they received an award from the National Institute of Health Interdisciplinary Roadmap Grant [30], for the evaluation of this problem [30]. Later she developed an Oncofertility consortium, that represents an International, multi institutional, Interdisciplinary team comprising of Clinicians, scientists, Clinical laboratory persons, social scientists, policy makers, besides other researchers for evaluation, integration, in addition to further make advances in this field. This group collectively, besides others exhaustively continuously has come out future guidelines for clinicians, patients in this field. Subsequently In the next few years different professional societies in addition to medical organization, that is inclusive of the National Comprehensive Cancer Network, the European Society for Medical Oncology, besides the American Society of Reproductive Medicine, published documents offering guidelines on fertility preservation [31].
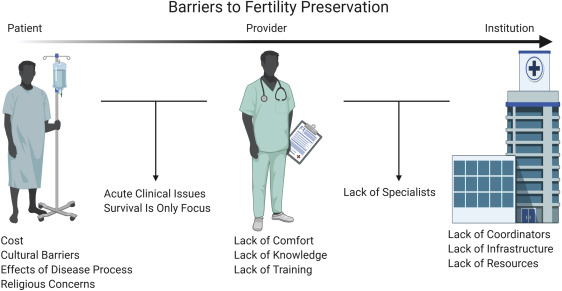
In spite of no controversy on this decision of fertility preservation needs to be taken into account, that is a necessary part of the cancer diagnosis in addition to treatment, a lot of hurdles are existent which may aid In avoidance of patients receiving proper counselling as well as treatment [32]. These hurdles can occur at 3 levels i) patients ii) the ones providing services iii) health care system (Figure 1) [33] i) Once the patient gets diagnosed with cancer might be taken aback with their total concentration over surviving from cancers with similar attitude of the treating physician. Further these men might be suffering from acute illness that makes consideration of fertility preservation tough; with in occasional cases it might become essential to start the cancer treatment immediately. Besides that patients might possess cultural or religious beliefs which limit their capacity or willingness for continuation of fertility preservation. Like some laws in Judaism in addition to Roman Catholicism limit the methodology by which semen samples collection for the purpose of cryopreservation of sperms are got, besides other religious factors might have an influence over the capacity of utilization of cryopreserved sperm in’’ in vitro fertilization’’ (IVF) [34]. For other patients they might possess financial limitations, despite their interest in fertility preservation, with minimal states giving insurance cover for these purposes. ii) Other than patients particular factors, then the care providers might work as barriers for fertility preservation. A lot of Oncology services givers possessing experience in the field of cancer treatment do not possess the knowledge, training/comfort that is required for the counseling of patients with regards to fertility preservation [35]. iii)Lastly, health care system factors might limit the patients accessibility to services of fertility preservation, since not all systems possess laboratory services for conducting semen evaluation, cryopreservation of sperms, with a lot not possessing contact with the reproductive specialists or coordinators with regards to giving guidelines to the patients that require these services.
In this context, the adolescents are specifically prone to such hurdles, thus do not get proper fertility preservation care [36]. Different studies conducted on the adult survivors who got over adolescent cancer have illustrated that these persons have been going through lot of regretfulness for not having borne the cost for the time they had for cryopreservation prior to the cancer treatment [1]. A lot of such men live accepting infertility in adult lives although absence of cryopreservation of sperms avoids their need for biological pregnancies. Further intriguingly, parents of these survivors have marked guilty feeling, besides, regretting for not having opted for fertility preservation care from their child’s point of view with him incapable of such decision making [1].
The particular problems with regards to adolescents usually are correlated with a lot of factors i) the silo action for Paediatric Oncology providers, since reproductive specialists classically do not work within the Paediatric centres ii) in a survey done at National level, Paediatric providers documented being uncomfortable, besides, having absence of knowledge In this context of fertility preservation discussion with paediatric cases in addition to their parents [35]. Intriguingly, in the same study of Paediatric nurses, nurse practitioners in addition to Oncologists, over 90% of every group wanted to get training in Oncofertility [35]. iii) Thirdly that is particular for Paediatric in addition to adolescents, like patients agreement along with difficulties in getting a semen specimen from a generating minor, might prove to be very difficult for patients, families in addition to care providers [37].
The generation of a formal fertility preservation program has proved to be of success to tackle these hurdles at an Institutonal level. A lot of Institutes have initiated formal fertility preservation program, that has ended in escalated numbers of patients getting a consultation with regards to fertility preservation program aiding in utilization of sperm cryopreservation services [38]. In the normal usual co-curriculum of Oncology fellowship to generate a fertility preservation material, academic grand rounds on that subject, other than tackling these problems at the time of clinical staff educational in service sessions are separate ways of tackling these providers in addition to systemic level hurdles for fertility preservation provision.
As documented, earlier, there is marked generation of this area of fertility preservation in clinical, laboratory medicine in addition to basic science domain. With our good fortune, the moment newer generation along with beliefs come out further updated different types of fertility preservation clinical guidelines have got published, in addition to other organizations like the American Urology Association/ American Society of Reproductive Medicine have with combination of their action given Guidelines [39, 40, 41].
Fertility Preservation Techniques
While fertility preservation in case of female patients classically patients invasive techniques like ovarian tissue extraction or ovarian stimulation with oocyte retrieval, in case of males it is the non-invasive collected ejaculated semen specimen that gets received by masturbation in the onsite existence of a laboratory in the OPD which is mostly achieved with success in case of male patients for admitted subjects as well. Particular organization can be done for promoting the collection at the existence laboratory in the hospital or In case of patient’s hospital room. Trying to coordinate with regards to the continuing Oncology diagnosis evaluation in addition to treatment might prove to be a challenge, which is the reason for which the patient’s navigation model has proved to be a significant strategy for promotion of success [42].
In case of certain patients, there might be hurdles in the generation of a semen specimen that is enough for fertility preservation that turns out to be successful. The difficulties that get encountered might be erectile function impairment, unable to ejaculate, aspermia (alias no sperm, retrograde ejaculation as well as, azoospermia. It is the good luck that urologists possess the expertise with regards to the treatment strategies which can in particular take care of all these problems, besides methods that get maximum used with success as far as fertility preservation is concerned. In certain patients, inspite of all the work, either they are unable to ejaculate, have aspermia (alias no sperm), retrograde ejaculation, besides which azoospermia might still continue.
As far as these patients are concerned, then an Oncologic testicular sperm extraction (onco-TESE) is the method that gets used to keep fertility preservation continuing. To start with introduced by Schrader, et al. [43], this method led to a rate of success in retrieval, of the sperms in about 50% of patients that had manifestation of azoospermia that was secondary to testicular germ cells tumors or lymphoma. Figure 2 details the full cotemporary prototype with regards to the clinical strategy in the context of fertility preservation in adult, in addition to adolescent boys that have got a diagnosis of cancer made.
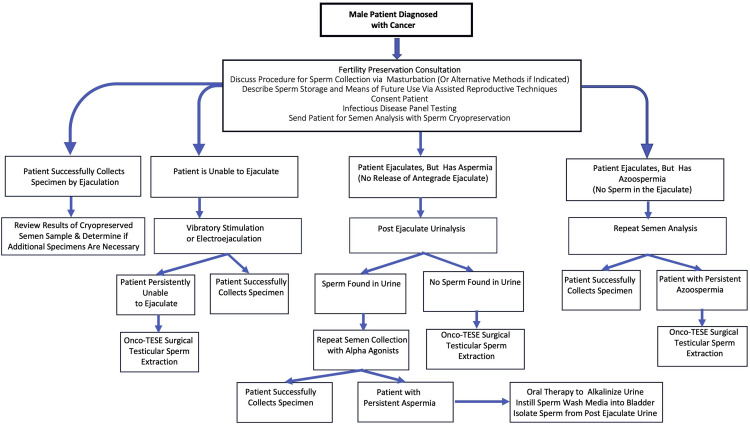
Figure 2: Courtesy ref no -33-Contemporary paradigm for male fertility preservation. A contemporary, comprehensive approach to fertility preservation for male patients diagnosed with cancer is presented. This paradigm incudes numerous methods to obtain sperm from individuals who are otherwise unable to provide a sufficient ejaculated semen specimen. onco- TESE = oncologic testicular sperm extraction.
Prepubertal boys comprise a distinctive paediatric population of patients for whom these above detailed strategies cannot get applied. To our misfortune, at the existent moment there is no clinical strategy for promotion of cryopreservation of sperm for a prepubertal male, in view of lack of active spermatogenesis in these patients [42, 44]. The average age of spermarche is about 13yrs, nevertheless, certain boys even upto 11 years age might have sperms In their ejaculate [45]. A good examination, a detailed generational history (like nocturnal emissions), besides physical examination (inclusive of Tanner staging) can aid in finding if these patients are actually prepubertal. Different experimental strategies are getting presently evaluated with these patients taken in account that hopefully a day will arrive when these studies prove to be fruitful with regards to yielding a pathway forward for giving care to these patients.
Just like in other clinical evaluation strategies, good ethical practices besides the Institutonal Review Board permission is necessary. Further the messages to clinicians are required to emphasize the experimental nature of these new methodologies that might never have translational capacity with regards to clinical effectiveness.
Results of Utilization of Cryopreserved Sperm from Men Post Cancer
Both patients as well as physicians are bothered with regards to the utilization of cryopreserved sperm in case of a patient who had been diagnosed with cancer earlier. Earlier different studies had documented lesser parameters with regards to semen in cases of men post cancer in contrast to controls [8, 9, 46]. Additionally, escalation of sperm aneuploidy along with DNA fragmentation have got documented, besides reduction In semen parameters in these [46, 47]. Inspite of these observations, the results of in vitro fertilization (IVF) in addition to Intracytoplasmic sperm injection (ICSI) with the utilization of cryopreserved sperm prior to the start of cancer treatment have illustrated akin results of pregnancy rate (PR) in addition to live birth rates (LBR), as well as rates with regards to fertilization failure, or miscarriage in contrast to cryopreserved sperm from men without cancer [48]. Further the timing of semen cryopreservation prior to the start of cancer treatment is also significant, in view of both radiation therapy along with chemotherapy can result in significant sperm aneuploidy along with DNA fragmentation [14, 15, 16, 46]. Despite the possibility of achieving success in fertilization being mostly inversely correlated with the quantity of sperm DNA injury, aberrant sperm still possesses sustenance of capacity for fertilization of oocyte in particular when in the setting of IVF/ ICSI [49, 50]. Though the results of reproduction in case of acute along with immediate post therapy are restricted in view of proper ethical as well as practical reasons, proper precautions are required when sperm generation occurs amidst cancer treatment or within a year of trying with regards to attainment of pregnancy [47]. Minimal results are available from the human studies, being restricted as well as maximum are from case studies. In a case report with regards to the reproductive outcome of 2 men having received treatment with chemotherapy for acute myelogenous leukaemia, the son of one of the patients manifestation was the tetralogy of Fallot along with syndactyly, whereas the other had a still birth with anencephaly [51]. Much more extensive data that is available has illustrated that genetic alterations in sperms that manifested at the time of chemotherapy caused new borns with escalation of chances of mutations besides genetic translocational like congenital abnormalities [52]. In view of these the American Urology Association/ American Society of Reproductive Medicine Guidelines with regards to diagnosis in addition to treatment of infertility in men have with formality asked the patients, to prevent natural conception actions besides utilization of contraception for a minimum of a year following finishing of the chemotherapy, as well as or radiotherapy [41]. Akin to that, these Guidelines advocate to not use sperm clinically with regards to assisted reproductive technology (ART). If conception attempts are tried at longer duration subsequent to cancer treatment, the incidence and prevalence of congenital abnormalities in the baby are akin to that of the general population [53]. Due to this patients need to be convinced with regards to utilization of cryopreserved sperm done prior to cancer treatment for ART. Akin to that even natural conception attempted later does not possess significant escalation of chances subsequent to a minimum of a year-2 from the finishing of cancer treatment.
Directions for Future Requirements of Fertility Preservation Still to be Met
As already detailed for certain patients, the methods are not enough for managing a good future reproductive capacity. Hence worldwide researchers inclusive of scientists, laboratory people, Clinicians are trying to tackle this hurdle.
Evaluation of Methods for Protection of Gonadal Tissue In Vivo: One probable strategy is to try for fertility preservation with the idea of protection of germ cells in addition to the somatic tissue that supports it in the natural surroundings at the time of delivery of cancer treatment.
This strategy known as ‘’ferto protection’’ possesses great capacity, despite it having been evaluated in just restricted manner [54]. Supposedly the maximum evaluated strategy with regards to ferto protection’’ has been attempting quiescence of spermatogenesis via repression of gonadotropins as well as testosterone liberation. These asctions have been corroborated by supporting outcomes in case of studies conducted in rats, that have received treatment with different combinations inclusive of GnRH agonist as well as antagonist in addition to /or anti androgens for conferring protection of the cells from the harmful actions of these cytotoxic therapies. Spermatogenesis recovery got escalated in rats that had gone via quiescence, nevertheless, this advantage was not visualized in other species that was inclusive of mice, dogs as well as monkeys [55]. In case of humans the clinical trials comprised of 7 studies where hormonal repression got stimulated prior to in addition to at the time of cytotoxic therapies. Of these 6 did not display any protection action on sperm generation whereas one study pointed little advantage [56]. Finally this hormonal repression does not seem to give any use full pathway for ’ferto protection’’. Nevertheless, the wider thought of delivery of neo adjuvant cancer therapy or adjuvant agents for protection of germ cells in addition to the somatic tissue that supports it in the natural surroundings is a field offering great capacity as well as attention [54].
Evaluation of Methods for Restoring Spermatogenesis: Different evaluation methods have been tried to restore spermatogenesis subsequent to injury to the testicular germ cells in addition to the micro environment around it. Though varying in their strategy most of them implicate removing cells/tissues from the patients prior to exposure to gonadotoxic therapies. Figure 3 for details, besides the details of the procedure.
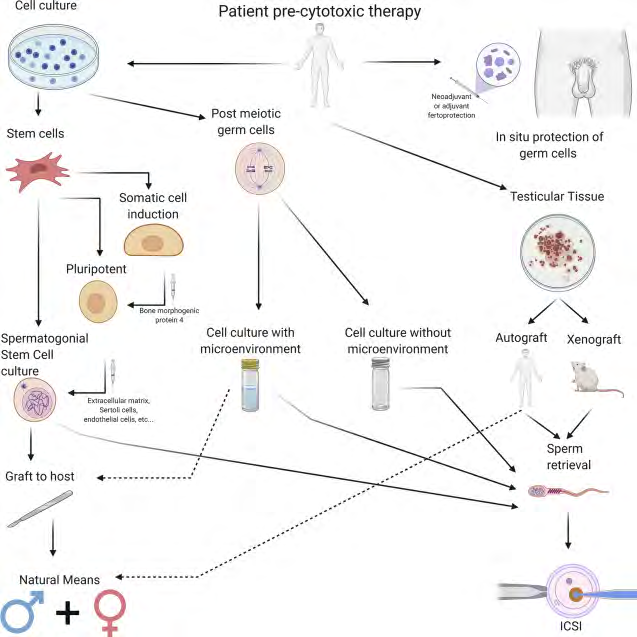
Figure 3: Courtesy ref no -33-Future directions: experimental and investigational approaches to fertility preservation. Numerous experimental and investigational methods are currently under study to facilitate fertility preservation in males. A wide array of techniques is considered, including fertoprotection, tissue grafting, cell culture, and stem cell techniques. ICSI = intracytoplasmic sperm injection.
• Culture of Testicular Tissue: The intricate association among generating germ cells in addition to micro environment that is correlated with testis is necessary for normal spermatogenesis. Certain evaluators have data with regards to generation of post meiotic germ cells in cell culture without requirement of the normal surrounding tissue of the seminiferous tubules [57]. Despite promising it needs future work.
Other researchers have tried exploration of culture of testiculartissue with the micro environment with regards to anatomy remaining intact. Sato, et al. [58, 59], succeeded in growing portion of the newborn murine testicular tissue in cell culture with the subsequent generation of functional sperm that possessed the capacity of fertilization. These evaluations gave an extra proof as well as significant understanding of this kind of study by utilization of froze thawed testicular tissue for generation of haploid cells by tissue culture. Despite the fertility capacity of this sperm was not evaluated the, researchers illustrated a favourable results that possess capacity of translational impact over future fertility preservation [59].
Different researchers have tried engineering biomimetic reproductive tissue which could work as an autonomous in vitro unit that aids in the generation of germ cells in addition to, function [60]. A lot of engineered systems have got evaluated that is inclusive of, decellularized extracellular matrix[ECM scaffolds, 3D bioprinting acellular scaffolds, 3D bioprinting with deposits of ‘’biolinks’’(akin to particular cell kinds) in appropriate areas on scaffolds, scaffolds free hydrogels in addition to microfluidic platforms that possesses multi tissue cultures for the reproducibility of hormone liberation dynamics [60, 61, 62]. These constructs possess the capacity of escalation of capacity of modeling normal tissue organ generation as well as homeostasis, hence with greater intricately reproducing the natural total in vivo reproductive surroundings for spermatogenesis.
• Testicular Tissue Autografting as Well as Xenografting Testicular Tissue: Despite the ovarian tissue transplantation is a method whose utilization has got done in women by the guidelines of proper Institutional, regulatory as well as ethical cover, testicular tissue transplantation has not as yet got generated in the way of a treatment method for men. Nevertheless, a lot of advances have got obtained in case of animal models, where immature testicular tissue from different mammalian species inclusive of mice, rat, cats, pigs, goats have got grafted underneath the skin of immune deficient animals, where spermatogenesis has been obtained with success, that makes sure that sperms can get obtained from these grafts of every one, besides, utilization in case of ART, resulting in pregnancy rates as well as live birth [63, 64, 65]. These rest of researchers, have further moved beyond conducting xenografting in prepubertal rhesus monkey (Macacca mulatta) testis, with acceleration in tissue maturation, besides generation of a functional sperm possessing competency in the xenografts [66].
Further significant advances in this field of transplantation were done in the recent past with autologous grafting of cryopreserved prepubertal rhesus testis [67]. This cryopreserved prepubertal testis tissue got autologously grafted underneath the scrotal in addition to back skin of castrated monkeys. In the subsequent 8-12 months, the escalation of graft size occurred, besides the generation of T. On gathering the grafts total spermatogenesis was observed in every graft. Following that certain of the sperms that had got isolated got utilized for IVF/ICSI for generation of embryo resulting in pregnancy. Finally a healthy female rhesus baby was born subsequent to this event. Despite, a guarded opinion given by these researchers with regards to clinical translation, they have incited future work with regards to fertility preservation in prepubertal boys.
Both testicular tissue autografting as well as xenografting possess inherent risks as well as advantages. Xenografting prevents the probable hazards of transplantation of malignant cells within the graft tissue again in the body of the cancer survivor. Nevertheless, the chances of infection of human graft tissue by viruses from a transplant animal host creates a marked problem that gets correlated with xenografting [68]. Autografting prevents these probable infections as complications yet possess a significant chance of neoplastic cells getting retransmitted back into the patient [69].
• Spermatogonial Stem Cells transplantation as Well as Culture: Brinster, et al. [70] along with his group documented series of publications, where they illustrated in 1994 that showed the success attained at Spermatogonial Stem Cells transplantation. They removed the testis of the donor mice as well as generated a cell suspension that possessed Spermatogonial Stem Cells which were injected into the recipient mouse seminiferous tubules. The mice were infertile with lack of spermatogenesis in their seminiferous tubules. Evaluation of the testes of these recipient mice 48 to 230 days subsequent to transplantation showed that the typical properties of the consecutive stages of spermatogenesis were existent, in addition to mature spermatozoa were observed in the lumen of the seminiferous tubules [70]. At last via this methodology the recipient mice could start a progeny with the utilization of donor obtained spermatozoa [71]. This strategy has got utilized in a lot of species, inclusive of dogs, cows sheep, boars, as well as rhesus monkeys [72, 73]. Spermatogonial Stem Cells from donor animals from all ages, varying from newborn to full grown adults which got transplanted to stimulate spermatogenesis in recipient animals [73]. These techniques got finished with success in cases where the donor sperm had got cryopreserved for upto 14yrs prior to transplantation [74].
How much is the engraftment rate (alias uptake) of the transplantated Spermatogonial Stem Cells is minimal. Subsequent to injections in the seminiferous tubules, these cells are required to transit via the blood testes barrier that is compulsory for achieving success in nesting on the basement membrane (BM) for the starting of spermatogenesis. The pattern in addition to kinetics of Spermatogonial Stem Cells engraftment in mice was evaluated by Nagano, et al. [75], as well as observed that for each million testicular cells that got transplanted, just about 19 Spermatogonial Stem Cells got colonized with spermatogenesis getting initiated. Maximum of transplanted cells got washed off or were actively phagocytosed by the native cells that were inclusive of the sertolicells [76]. His generation of colonies in this particular study took place in 1-4wks following a transplantation method [75].
In human beings, total In vitro Spermatogenesis from SSCs to Spermatozoa has not taken place. Maximum differentiated germ cells obtained from immature testicular tissue is the spermatid stage [77]. A lot of studies have emphasized on the probable methods that might aid in overcoming the problems encountered during In vivo Spermatogenesis. As per Medano, et al. [78], it was shown that if immature testicular tissue got cultured at a temperature of 340 C, it decreased the degree of apoptosis rate within the tubules as well as caused a slowing of rate of alteration in morphogenesis as compared to immature testicular tissue cultured at a temperature of 370C. On exposure to follicle stimulating hormone (FSH)/luteinizing hormone (LH), enhanced amount of undifferentiated as well as premeiotic Spermatogonia having enhanced survival of sertoli cells, pointing that gonadotropin administration might be essential for efficacy in In vitro Spermatogenesis. Other trials to simulate the testicular niche with extra T, HCG, as well as retinoic acid lead to enhanced numbers of premeiotic Spermatogonia, which pointed that the supplementation of these might also facilitate differentiation of SSCs [79].
One significant process that takes place at the initiation of in vivo spermatogenesis (or puberty is the development of the Blood-testis barrier (BTB), that has a key part in Spermatogenesis [80]. Mice possessing knockouts or mutations in the BTB proteins mostly present with aberrations in spermatogenesis [81], as well as it is feasible that humans having similar aberrations would also present with subfertility. Expression of BTB structural proteins connexin 43 as well as claudin 11 within In vitro testicular culture, pointing that BTB generation even takes place outside of natural testis, was seen by De Michaele, et al. [82], despite that, what it suggest is not clear.
Methodologies are getting studied for promotion of the Spermatogonial Stem Cells getting enriched for the escalation of transplantation event [83]. Fluorescence and magnetic activated cell sorting, a particular kind of flow cytometry, is getting evaluated in the form of a method that besides enrichment of the Spermatogonial Stem Cell populations, separates the malignant cells from the suspension prior to transplantation [84]. The other strategies with regards to enrichment of the Spermatogonial Stem Cells are trying generation of Spermatogonial Stem Cell populations which are not expanded in a clonal fashion, with this strategy aids in preventing the neoplastic cells re-entering from the patients point of view [85].
A clinical trial that evaluated germ cell transplantation was started in a case of Hodgkin’s lymphoma in 1999 [86]. Radford, et al. [86], documented that 11 men had testicular tissue collected, besides generation of a cell suspension. In case of 5 patients, injection of the suspension was done into the donor testes, however no evaluation of semen followed by the procedure was later given [86].
Later Kanatsu-Shinohara, et al. [87], documented long time proliferation of mouse Spermatogonial Stem Cell with success in vitro in addition to illustrated restored fertility in cases of congenitally infertile mouse, that were recipients of the transplanted germline Stem Cells in 2003 [87]. Subsequently Sadri-Ardekani, et al. [88], in 2009 followed, with the utilization of an akin methodology for generation of a long time culture of the adult human Spermatogonial Stem Cells in vitro. Following that they documented success after utilization of testes from prepubertal boys for the generation of Spermatogonial Stem Cells cultures for a longer time [89]. Since then a lot of groups have managed the sustenance of akin Spermatogonial Stem Cells cultures.Here there concentration has now switched to generation of new plating techniques along with culture media with the idea of getting ideal results [90].
Success of this mouse Spermatogonial Stem Cell lines have got estimated by transplantation along with generation of spermatogenesis in the recipient organism. In view of both practical in addition to ethical purposes human- human transplantation is not being done, however, human to immunodeficient mouse transplantation is a technique utilized for the evaluation of function. Till date, human Spermatogonial Stem Cells from culture have not generated total spermatogenesis in recipient mice, however, they have been restricted to the BM to develop maintaining clusters which possess capacity of survival for long time [91].
Attempting to translate these methodologies towards patient care gets negated by the kind of recipient testicular microenvironment. This niche can get deleteriously influenced by a lot of factors inclusive of i) systemic inflammation along with fibrosis that is correlated with the history of cancer, ii) the harmful structural as well as functional alterations subsequent to chemotherapy along with radiotherapy exposure, iii) besides aging associated alterations [54].
• Pluripotent Stem Cell Methods: Stem Cells represent undifferentiated or just partly differentiated cells possessing the capacity to differentiate into other cell kinds or keep proliferating as the same cell kinds. Pluripotent Stem Cells represent embryonic Stem Cells that possess the capacity to self renew or to generate into one of the 3 primary germ cell layers of the body, namely endoderm, ectoderm, as well as mesoderm. Induced pluripotent Stem Cells represent a kind of pluripotent Stem Cells which are generated directly from somatic cells. [92]. This significant method was invented by Takahashi as well as Yamanaka in 2006 with the utilization of fibroblast cultures subsequent to supplementation with a lot of factors [93]. On injection of these cells into blastocyst, aids in embryonic generation.
This method that got pioneered by Takahashi as well as Yamanaka, et al. [93] has been put into use for reproductive science evaluations, A lot of centers have got demonstrated that murine, monkeys in addition to human embryonic Pluripotent Stem Cells or Induced Pluripotent Stem Cells can get differentiated into germ cells [94]. Successful differentiation of embryonic Stem Cells as well as Induced Pluripotent Stem Cells was illustrated by Hayashi, et al. [94], into epiblast-like cells which propagated to germ-like cells on incubation in culture with Bone morphogenetic protein4 (BMP4). Subsequent to transfer into immunodeficient mice, these germ cells started spermatogenesis, besides causing the generation of gametes. These gametes were garnered as well as utilized for IVF/ICSI for fertilization of oocyte in addition to generate embryos. These embryos were subsequently transferred into recipient females, with live babies were born. Certain of these children had the, generation of neck tumors, dying later, that resulted in tension with regards to these procedures, that is inclusive of the strategies utilized for differentiation as well as the culture media utilized [94]. Despite the favourable response that is offered by Spermatogonial Stem Cell culture methodologies with regards to getting over infertility, presently, these strategies are just in experimental stage.
In case of setting with regards to fertility preservation, in case there is no existence of mature gametes for cryopreservation, testicular tissue cryopreservation, that is still investigational might be thought off [95]. This strategy, which is specifically applicable to prepubertal boys in view of lack of spermatogenesis, is being offered via certain centers in the form of an experimental methodology in the supervision of the Institutional Review Board permission. Hopefully, a day will arrive once basic science would advance till we are capable of -translation of these in the clinical scenario. The testicular tissue extractional methodology can usually get conducted simultaneously with rest of procedures like BM biopsy as well as portacath placement. A documentation from a single Institution showed significantly good tolerance in addition to lesser complications rate (1of 23 patients, besides minor grade 1 complication) in case of young males that went via this methodology [96].
Subsequent to their earlier documentation of Cryopreservation programme for immature testicular tissue, the group of Goosens, et al. [97], earlier detailed by us in ref 2, they further [98], reviewed how future fertility was significant for long-term quality of life in patients who had got chemotherapy along with/or radiotherapy at the time of childhood. Hence newer approaches for rising hope of patients with regards to becoming a father of their own child has become necessary to be generated besides got into clinical practice. Testicular tissue cryopreservation is currently the only possibility to preserve fertility potential in children because sperm are not generated until puberty.
Strategies for getting mature sperm from prepubertal testicular tissue are under evaluation in addition to studies in monkeys having documented the possibility. Thus, an escalating amount of centres worldwide now recommend testicular tissue cryobanking as an experimental method for patients with the aim of obtaining mature sperm from the tissue in the future. Approaches under investigation include in vitro culture or autologous transplantation of testicular tissue or cells. Further destailing the current progress in fertility preservation for prepubertal boys, besides, the limitations that need tackling prior to these strategies can be implemented in clinical practice.
Similarly Doungkamchan in addition to Orwig reviewed the same aspects with regards to so much cryopreserved testicular tissue is existent with a moral responsibility of translation into Clinical practice for these prepuertal boys with aim of finding ways and means of the same [99].
Recently del Vento, et al. [100] detailed how avascular transplantation of frozen–thawed testicular tissue fragments represents a technique for the coming future with regards to future fertility restoration in boys with cancer. A significant loss of spermatogonia was observed in xeno-transplants of human tissue most probably secondary to the hypoxic period prior to revascularization. For reduction of the actions of hypoxia–reoxygenation damages, various strategies have already been evaluated, like encapsulation in alginate hydrogel in addition to supplementation with nanoparticles that administer a necrosis inhibitor (NECINH) or VEGF. While these approaches enhanced short-term (5 days) vascular surfaces in grafts, neovessels were not maintained up to 21 days; i.e., the time required for attaining vessel stabilization. For obtaining better support tissue grafts, nanoparticles loaded with VEGF, PDGF and NECINH were developed. Testicular tissue fragments from 4–5-week- old mice were encapsulated in calcium-alginate hydrogels, either non-supplemented (control) or supplemented with drug-loaded nanoparticles (VEGF-nanoparticles; VEGF- nanoparticles+PDGF-anoparticles; NECINH-nanoparticles; VEGF-nanoparticles + NECINH-nanoparticles; and VEGF – nanoparticles + PDGF-nanoparticles + NECINH- nanoparticles) before auto-transplantation. Grafts were recovered after 5 or 21 days for analyses of tissue integrity (hematoxylin–eosin staining), spermatogonial survival (immuno-histo-chemistry for promyelocytic leukemia zinc finger) and vascularization (immuno-histo-chemistry for α-smooth muscle actin and CD-31). Our results showed that a combination of VEGF and PDGF nanoparticles increased vascular maturity and induced a faster maturation of vascular structures in grafts [100].
Human male reproductive development has a prolonged prepubertal period characterized by juvenile quiescence of germ cells with immature spermatogonial stem cell (SSC) precursors (gonocytes) present in the testis for an extended period of time. The metabolism of gonocytes is not defined. Furthermore, Laura Voigt, et al. [101], illustrated with the utilization of mitochondrial ultrastructure studies through transmission electron microscopy (TEM) in addition to Immunohistochemistry (IHC) as well as metabolic flux studies with UHPLC-MS that a distinctive metabolic transition occurs at the time of the maturation to SSCs. The mitochondrial ultrastructure of prepubertal human spermatogonia is common to that of prepubertal pig spermatogonia. The metabolism of early prepubertal porcine spermatogonia (gonocytes) has the properties of dependence on Oxidativephosphorylation (OXPHOS) that needs fuelling by oxidative decarboxylation of pyruvate. Intriguingly during, the same time, a large quantity of the intake of pyruvate gets further reduced in addition to excreted as lactate. With maturation, prepubertal spermatogonia demonstrate a metabolic switch with reduction in OXHPOS along with upregulation of the anaerobic metabolism- correlated uncoupling protein 2 (UCP2). This switch is associated with stem cell specific promyelocytic leukemia zinc finger protein (PLZF) protein expression, besides glial cell-derived neurotropic factor (GDNF) pathway activation. The outcome of their study illustrated that gonocytes separately from mature spermatogonia demonstrate individual metabolic demands that need to be obtained to ensure their maintenance and growth in vitro [101].
Conclusion
Cancer in the form of a disease event in addition to Oncology therapies like chemotherapy can badly influence male reproductive capacity, which results in permanent infertility in a lot of men. During the course of last 2 decades generation of fertility preservation has become a crucial subject in cases of survivors of cancer, with a lot of medical organizations in addition to professional societies giving guidelines that necessitate routine fertility preservation during oncology treatment. Whereas maximum male cancer patients have the capacity of generation of an ejaculated semen specimen for the promotion of fertility preservation, alternate techniques of trying isolation of sperms are existent for those patients not capable of yielding an ejaculated specimen that is enough. Although, besides, the existence of these additional techniques fertility preservation keeps being not possible for certain patients that is inclusive of prepubertal boys, besides certain adult mature patients who do not, possess the capacity of sperm generation. For these persons a lot of experimental techniques are presently getting evaluated, hoping that a day will arrive when we will possess the capacity of translation with the advances in technology for efficaciously aiding such patients.
References
-
Stein DM, Victorson DE, Choy JT, Walmey KE, Pearman TP, et al. (2014) Fertility preservationpreferences and perspectives among male survival of paediatric Cancer and their parents. J Adolesc Young Oncol 3(2): 75-82.
-
Anderson RA, Clatot F, Demestere I, Lamertini M, Morgan A, et al. (2020) Cancer survivorship: reproductive health outcomes should be Included in Standard toxicity assessments. Eur J Cancer 144: 310-316.
-
Kulvinder KK, Allahbadia GN, Singh M (2019) An Update on Management of Oncofertility-Does the Use of Vsels Appear Practical in the Near Future in Human Malignancies Replacing Cortical Tissue/Testicular Tissue Transplantation. Int J Stem Cell Regen Med 1(1): 1-11.
-
Kulvinder KK, Allahbadia GN, Singh M (2020) How Far Have We Reached with Regards to Our Endeavours in Testicular Tissue Transplantation Along with in Vitro Spermatogenesis After Success in Animals-A Systematic Review. Arch Urol 3(2): 1-15.
-
Van Norren K, Dwarkasig JT, Witkamp RF (2017) The role of hypothalamic inflammation, the hypothalamic- pituitary-adrenal axis and serotonin in the Cancer anorexia cachexia syndrome. CurrOpi Clin Nutr Metab 20(5): 396-401.
-
Garcia JM, Li H, Mann D, Epner D, Hayes TG, et al. (2006) Hypogonadism in male patients with cancer. Cancer 106(12): 2583-2591.
-
Burney BO, Hayes TG, Smiechowska J, Cardwell G, Papusha V, et al. (2012) Low testosterone levels and increased inflammatory markers in patients with Cancer and relationship with cachexia. J Clin Endocrinol Metab 97(5): E700-709.
-
Williams DH, Karpman E, Sander JC, Spies PE, Pisters LL, et al. (2009) Pre treatment semen parameters in men with Cancer. J Urol 181: 736-740.
-
Berthelsen JG, Skakkaebaek NE (1983) Gonadal function in men with testis Cancer. Fertil Steril 39(1): 68-75.
-
Monish DW, Venner PM, Sly O, Barron G, Bhardwaj D, et al. (1990) Mechanisms of endocrine dysfunction in patients with testicular cancer. Cancer Inst 82(5): 412-418.
-
Klein B, Haggeney T, Fietz D, Indumathy S, Loveland KL, et al. (2016) Specific immune cell and cytokine characteristics in human testicularneoplasia. Hum Reprod 31(10): 2192-2202.
-
Allard J, Trust WA, MacKenna KE, Coolen LM (2005) Spinal cord control of ejaculation. World J Urol 23(2): 119-126.
-
Wallace WHB, Anderson RA, Irvine DS (2005) Fertility preservation for young patients with cancer: who is at risk and what can be offered?. Lancet Oncol 6(4): 299- 318.
-
Meistrich ML (2009) Male gonadal toxicity. Pediatr Blood Cancer 53(2): 261-266.
-
Meistrich ML (2013) Effects of chemotherapy and radiotherapy on spermatogenesis in human men. Fertil Steril 100(5): 1180-1186.
-
Meistrich ML (1993) Effects of chemotherapy and radiotherapy on spermatogenesis. Eur Urol 23(1):136- 141.
-
Poorvu PD, Frazier AL, Feraco AM, Manley PE, Ginsberg ES, et al. (2019) Cancer treatment related infertility: a critical review of the evidence. JNCI Cancer Spectr 3(1): pkz008.
-
Green DM, Liu W, Kutteh WH, Shelton KC, Sklar CA, et al. (2014) Cumulative alkylating agentexposure and semen parameters in adult survivors of childhood Cancer:areport from the St Jude lifetime cohort study. Lancet Oncol 15(11): 1215-1223.
-
Tammela T (2004) endocrine treatment of prostate Cancer. J Steroid Biochem Mol Biol 92(4): 287-295.
-
Wood GJ, Hayden RP, Tannikut C (2017) Succesful sperm extraction and live birth after radiation, androgen deprivation and surgical castration for treatment of metastastic prostate Cancer. Andrologia 49(1): e12578.
-
Scovell JM, Benz K, Samarska I, KohnTP, Hooper JE, et al. (2020) Association of impaired spermatogenesis with the use of immune checkpoint inhibitor in patients with malignant melanoma. JAMA Oncol 6(8): 1297-1299.
-
Dubey P, Wilson G, Mathur KK, Hagemeister FB, Fuller LM, et al. (2000) Recovery of sperms production following radiation therapy for Hodgkin’s disease after induction Chemotherapy with mitoxantrone, vincristine, vinblastine and prednisone(NOVP). Int J Radiat Oncol Biol Phys 46(3): 609-617.
-
Gordon W, Seigmund K, Stanisic DH, McKnight B, Harris IT, et al. (1997) A study of reproductive function in patients with seminoma treated with radiotherapy and orchidectomy (SWOG-8711). Int J Radiat Oncol Biol Phys 38(1): 83-94.
-
Zhang Z ,Shao S, Meistrich ML (2007) The radiation induced block In spermatogonial differentiation is due to damage to the somatic environment, not the germ cells. J Cell Physiol 211(1): 149-158.
-
Ohl DA, Quallich SA, Sonksen J, Brackett NL, Lynne CM (2008) Anejaculation and retrograde ejaculation. Urol Clin North Am 35(2): 211-220.
-
Howlander M, Krapcho M, Miller D, Brest A, Yu M, et al. (2020) SEER Cancer Statistics Review, 1975-2016, National Cancer Institute. SEER Database.
-
Ethics Committee of the American Society of Reproductive Medicine (2005) Fertility preservation and reproduction in cancer patients. Fertil Steril 83(6): 1622-1628.
-
Lee SJ, Schover LR, Patridge AH, Patrizio P, Wallace WH, et al. (2006) American Society for Clinical Oncology recommendations on fertility preservation in cancer patients. J Clin Oncol 24(18): 2917-2931.
-
Woodruff TK, Ataman Milhouse L, Acharya KS, Almeda Santos T, Anazodo A, et al. (2021) A view from the past into our collective future: the Oncofertility consortium vision statement. J Assoc Reprod Genet 38(1): 3-15.
-
Smith BM, Ducan FE, Ataman L, Smith K, Quinn GP, et al. (2018) The National Physicians Cooperative transforming fertility management in the cancer setting and beyond. Future Oncol 14(29): 3059-3072.
-
Ethics Committee of the American Society of Reproductive Medicine (2013) Fertility preservation and. and reproduction in patients facing gonadotoxic therapies. Fertil Steril 100(5): 1224-1231.
-
Halpern JA, Das A, Faw CA, Braanigan RE (2020) Oncofertilityin adult andpaediatric populations. Transl Androl Urol 9(Suppl 2): S227-S238.
-
Brannigan RE, Fantus RJ, Halpern JA (2021) Fertility preservation in men :a contemporary overview and a look toward emerging technologies. Fertil Steril 115(5): 1126-1139.
-
Ramstein JJ, Halpern J, Gadzinski AJ, Brannigan RE, Smith JF (2017) Ethical, moral, and theological insights into advances in male paediatric and adolescent fertility preservation. Andrology 5(4): 631-639.
-
Fuchs A, Kashanian JA, Clayman ML, Gosiengfiao Y, Lockart B, et al. (2016) Paediatric Oncol ogy providers attitudes and practice patterns regarding fertility preservation in adolescent male cancer patients. J Paediatr Haematol Oncol 38(2): 118-122.
-
Kohler TS, Kondapalli LA, Shah A, Chan S, Woodruff TK, et al. (2011) Results from the survey for preserva- tion of adolescent reproduction(SPARE) study: gen- der disparity In delivery of fertility preservation message to adolescents with cancer. J Assoc Reprod Genet 28(3): 269-277.
-
Fallat ME, Hutter J, AmericanAcademy of Paediatrics Committee on Bioethics, American Academy of Paediatrics Section on Haematology,/Oncology, AmericanAcademy of Paediatrics Section on Surgery. (2008) Preservation of fertility in paediatric and adolescent patients with cancer. Paediatrics 121(5): e1461-1469.
-
Lopategui DM, Ibrahim E, Abdalla TC, Brackett NL, Yachieli R, et al. (2018) Effect of a formal Oncofertility program on fertility preservation rates –first year experience. Transl Androl Urol 7(S3): S271-S275.
-
Ethics Committee of the American Society of Reproductive Medicine (2018) Fertility preservation and. and reproduction in patients facing gonadotoxic therapies: an Ethics Committee opinion. Fertil Steril 110(3): 380-386.
-
Schlegel PN, Sigman M, Collura M, deJonge CJ, Eisenberg ML, et al. (2021) Diagnosis and treatment of in fertility in men:AUA/ASRMguideline part 1. Fertil Steril 115(1): 54-61.
-
Schlegel PN, Sigman M, Collura M, deJonge CJ, Eisenberg ML, et al. (2021) Diagnosis and treatment of in fertility in men: AUA/ASRMguideline part II. Fertil Steril 115(1): 62-69.
-
Redig AJ, Braanigan RE, Stryker SJ, Woodruff TK, Jeruss JS (2011) Incorporating fertility preservation into the care of Young Oncology patients. Cancer 117(1): 4-10.
-
Schrader M, Muller M, Sofikitis N, Straub B, Krause H, et al. (2003) ‘’Oncotese’’ testicular sperm extraction in azoospermic Cancer patients before chemotherapy-new Guidelines. Urology 61(2): 421-425.
-
Johnson EK, Finlayson C, Rowell EE, Gosiengfiao Y, Pavone ME, et al. (2017) Fertility preservation for paediatric patients:current state and future possibilities. J Urol 198(1): 186-194.
-
Halpern JA, Thrumavalan N, Kohn TP, Patel AS, Leong JY, et al. (2019) Distribution of semen parameters among adolescent males undergoing fertility preservation in a multicenter International cohort. Urology 127: 119-123.
-
Martinez G, Walsschaerts M, Le Mitouard M, Bory R, Thomas C, et al. (2017) Impact of Hodgkin’s or non Hodgkin’s lymphoma and their treatments on sperm aneuploidy:a prospective study of the French CECOS Network. Fertil Steril 107(2): 341-350.
-
Choy T, Braanigan RE (2013) The determination of reproductive safety in men during and after cancer treatment. Fertil Steril 100(5): 1871-1891.
-
Horvitz A, Goldschlag DE, Davis OK, Gorden LV, Palermo GD, et al. (2008) Intracytoplasmic sperm injection (ICSI) using cryopreserved sperm from men with malignant neoplasms yield high pregnancy rates. Fertil Steril 90(3): 557-563.
-
Aitken RJ (2004) Founder’s lectue. Human spermatozoa: fruits of creation, seeds ofdoubt. Reprod Fertil Dev 16(7): 655-664.
-
Tesarik J, Mendoza C, Greco E (2002) Paternal effects acting during the first cell cycle of human preimplantation development after ICSI. Hum Reprod 17(1): 184-189.
-
Russell JA, Powles RL, Oliver RT (1976) Conception and congenital abnormalities after chemotherapy of acute myelogenoous leukaemia in two men. Br Med J 1(6024): 1508.
-
Trasler JM, Doerksen T (1999) Teratogen update: paternal exposures- reproductive risks. Teratology 60(3): 161-172.
-
Green DM, Zevon M, Lowrie D, Seigestein N, Hall B (1991) Congenital anomalies in patients who received chemotherapy for cancer in childhood and adolescence. N Engl J Med 325(3): 141-146.
-
Duncan FE, Feinberg E, Braanigan RE, Edmonds M, Ataman L, et al. (2019) Fertility preservation. In: Strauss IIIJF, Barbieri RL, et al. (Eds.), Yen & Jaffes reproductive endocrinology. 8th (Edn.), Philadelphia Elsevier pp: 857- 886.
-
Meistrich ML, Shetty G (2008) Hormonal suppression for fertility preservation in males and females. Reproduction 136(6): 691-697.
-
Masala A, Faedda R, Alagna S, Satta A, Chiarelli G, et al. (1997) Use of testosterone to prevent Cyclophosphamide- induced azoospermia. Ann Int Med 126(4): 292-295.
-
Abu Elhija M, Lunenfeld E, Schlatt S, Huleihel M (2012) Differentiation of murine male germ cells to spermatozoa in a soft culture system. Asian J Androl 14(2): 285-293.
-
Sato T, Katagiri K, Gohbara A, Inoue K, Ogonuki N, et al. (2011) In vitro production of functional sperm in cultured neonata mouse testis. Nature 471: 504-507.
-
Sato T, Katagiri K, Kubota Y, Ogawa T (2013) In vitro Sperm production from mouse Spermatogonial Stem Cell lines using an organ culture method. Nat Protoc 8(11): 2098-2104.
-
Gargus ES, Rogers HB, M Kinnon KE, Edmonds ME, Woodruff TK (2020) Engineered reproductive tissue. Nat Biomed Eng 4(4): 381-393.
-
Murdoch MH, David S, Swine hart IT, Reing JE, Tran K, et al. (2019) Human extra cellular matrix enhances Human Spermatogonial Stem Cells in vivo. Tissue Eng Part A 25(7-8): 663-676.
-
Edmonds ME, Woodruff TK (2020) Testicular organoid formation is a property of immature somatic cells, which self-assemble and exhibit long term–hormone responsive endocrine function. Biofabrication 12(4): 045002.
-
Schlatt S, Honaramooz A, Boiani M, Scholer H, Dobrinsky I (2003) Progeny from Sperm obtained after ectopic grafting of neonatal mouse testes. Biol Reprod 68(6): 2331-2335.
-
Honaramooz A, Snedaker A, Boiani M, Scholer H, Dobrinsky I, et al. (2002) Sperm from neonatal mammalian testis grafted in mice. Nature 418(6899): 778-781.
-
Snedaker AK, Honaramooz A, Dobrinsky IA (2004) game of cat and mouse: xenografting oftestis tissue from domestic kittens results in complete catspermatogenesis in a mouse host. J Androl 25(6): 926-930.
-
Honaramooz A, Li MW, Penedo MC, Meyers S, Dobrinsky I (2004) Accelerated maturation of primate testis by xenografting into mice. Biol Reprod 70(5): 1500-1503.
-
Fayomi AP, Peters K, Sukhmami M, Valli-Pulansky H, Shetty G, et al. (2019) Autologous grafting of cryopreserved prepubertal rhesus testis produces Sperm and offspring. Science 363(6433): 1314-1319.
-
Kimsa MC, Strzalika-Mrozik B, Kimsa MW, Gola J, Nich- olson P, et al. (2014) Porcine endogenous retroviruses in xeno transplantation-- molecular aspects. Viruses 6(5): 2062-2083.
-
Gassei K, Orwig KE (2016) Experimental methods to preserve male fertility and treat male factor fertility. Fertil Steril 105(2): 256-266.
-
Brinster RL, Zimmermann JW (1994) Spermatogenesis following male germ cells transplantation. Proc Natl Acad Sci USA 91(24): 11298-11302.
-
Brinster RL, Avarock ME (1994) Germline transmission of donor haploid following Spermatogonial transplantation. Proc Natl Acad Sci USA 91(24): 11303- 11307.
-
Herrid M, Olejnik J, Jackson M, Suchowerska N, Stockwell S, et al. (2009) Irradiation enhances the Efficiency of testicular germ cells transplantation in sheep. Biol Reprod 81(5): 898-905.
-
Hermann BP, Sukhwani M, Winkler F, Pascarella JN, Peters KN, et al. (2012) Spermatogonial Stem Cells transplantation in rhesus testis regenerates Spermatogenesis producing functional Sperms. Cell Stem Cell 11(5): 715-726.
-
Wu X, Goodyear SM, Abramowitz LK, Bartolomei MS, Tobias JW, et al. (2012) Fertile offspring derived from mouse Spermatogonial Stem Cells Cryopreserved for more than 14 years. Hum Reprod 27(5): 1249-1259.
-
Nagano M, Avarock MR, Brinster RL (1999) Pattern and kinetics of mouse donor Spermatogonial Stem Cells colonization in recipient testes. Biol Reprod 60(6): 1429-1436.
-
Parreira GG, Ogawa T, Avarbock MR, Franca R, Brinster RL, et al. (1998) Development of germ cells transplants in mice. Biol Reprod 59(6): 1360-1370.
-
Abofoul Azab M, Abumadhighem A, Lunenfeld E, Kapelushnik J, Shi Q, et al. (2018) Development of post meiotic cells In vitro from Spermatogonial Cells of prepubertal cancer patients. Stem Cells Dev 27(15): 1007-1020.
-
Medrano JV, Vilanova Perez T, Fernez Ferrer V, Navarro Gomezlechon A, Martinez Tiguero ML, et al. (2018) Influence of temperature, serum and gonadotropin supplementation in short and longterm organotypic culture of human immature testicular tissue. Fertil Steril 110(6): 1045-1057.
-
De Michaele F, Poels J, Weerens L, Petit C, Evrard Z, et al. (2017) Preserved seminiferous tubules integrity with Spermatogonial survival and induction of sertoli and leydig cells maturation after longterm organotypic culture of prepubertal humantesticular tissue. Hum Reprod 32(1): 32-45.
-
Giudice MG, De Michaele F, Poels J, Vermuelen M, Christine W (2017) Update on Fertility restoration from prepubertal Spermatogonial Stem Cells: how far are we from clinical practice?. Stem Cells Res 21: 171-177.
-
Jiang XH, Bukhari I, Zheng W, Yin S, Wang Z, et al. (2014) Blood-testis barrier and Spermatogenesis: lessons from genetically modified mice. Asian J Androl 16(4): 572- 580.
-
De Michaele F, Poels J, Giudice MG, De Smedt F, Ambroise J, et al. (2018) In vitro formation of the Blood-testis barrier during longterm organotypic culture of prepubertal human testicular tissue: comparison with a large cohort of pre/peripubertal boys. Mol Hum Reprod 24(5): 271-282.
-
David S, Orwig KE (2020) Spermatogonial Stem Cells Culture in Oncofertility. Urol Clin North Am 47(2): 227- 244.
-
Fujita K, Ohta H, Tsujimura A, Takao T, Miyagawa Y, et al. (2005) Transplantation of Spermatogonial Stem Cells isolated from leukaemic mice restores fertility without inducing leukaemia. J Clin Invest 115(7): 1855-1861.
-
Sadri Ardekani H, Atala H (2014) testicular tissue cryo- preservation and Spermatogonial Stem Cells transplan- tation to restore fertility: from bench to bedside. Stem Cell Res Ther 5(3): 68.
-
Radford J, Shalet S, Leberman B (1999) Fertility after treatment for cancer: questions remain over ways of preserving ovarian and testicular tissues. BMJ 319(7215): 935-936.
-
Kanatsu Shinohara M, Ogonuki N, Inoue K, Miki H, Ogura A, et al. (2003) Long-term proliferation in culture and germline transmission of mouse male germline Stem Cells. Biol Reprod 69(2): 612-616.
-
Sadri Ardekani H, Mizrak SC, Van daalen SKM, Korver CM, Roepers Gajadien HL, et al. (2009) Propagation of human Spermatogonial Stem Cells in vitro. JAMA 302(19): 2127-2134.
-
Sadri Ardekani H, Akhondi MA, Van der Veen F, Repping S, Van Pelt AMM (2011) In vitro propagation of human prepubertal Spermatogonial Stem Cells. JAMA 305(23): 2416-2418.
-
Liu S, Tang Z, Xiong T, Tang W (2011) Isolation and characterization of human Spermatogonial Stem Cells. Reprod Biol Endocrinol 9: 141.
-
Valli H, Sukhmami M, Dovey SL, Peters KA, Donohue J, et al. (2014) Fluorescence and magnetic activated cell sorting strategies to isolate and enrich human Spermatogonial Stem Cells. Fertil Steril 102(2): 566-580.
-
Kulvinder KK, Allahbadia GN, Singh M (2016) Induced Pluripotent Stem Cells-Emphasis on Transcriptomics and Recent Advances in Therapeutic Potential. Transcriptomics 4: 1(1-6).
-
Takahashi K, Yamanaka S (2006) Induction of pluripotent Stem Cells from mouse embryonic and fibroblast cultures by defined factors. Cell 126(4): 633-676.
-
Hay ashi K, Ohta H, Kurimoto K, Aramaki S, Saitou M (2011) Reconstitution of the mouse germ cells specification pathway in culture by pluripotent Stem Cells. Cell 146(4): 519-532.
-
Valli Pulaski H, Peters KA, Gassei K, Steimer SR, Sukhwani M, et al. (2019) Testicular tissue cryopreservation: 8 years of experience from a coordinated network ofacademic centers. Hum Reprod 34(6): 966-977.
-
Corkum KS, Lautz TB, Johnson EK, Reimann MB, Waltz AL, et al. (2019) Testicular wedge biopsy for fertility preservation in children at significant risk for azoospermia after gonadotoxic therapy. J Pediatr Surg 54(9): 1901-1905.
-
Braye A, Tournaye H, Goosens E (2019) Setting up a Cryopreservation programme for immature testicular tissue: lessons learnt after more than 15 years of experience. Clin Med Insights Reprod Health 13: 1179558119886342.
-
Goosens E, Jahnukainen K, Mitchell RT, van Pelt AMM, Pennings G, et al. (2020) Fertility preservation in boys:recent developments and new insights. Hum Reprod Open 2020(3): hoaa016.
-
Doungkamchan C, Orwig KE (2021) Recent advances: fertility preservation and fertility restoration in males and females. Fac Rev 10: 55.
-
del Vento F, Poels G, Vermuele M, Uckaker B, Giudice MG, et al. (2021) Accelerated and Improved Vascular Maturity after Transplantation of Testicular Tissue in Hydrogels Supplemented with VEGF- and PDGF-Loaded Nanoparticles. Int J Mol Sci Open 22(11): 5779.
-
Laura Voigt A, Andrew Kondro D, Powell D, Valli- Pulaski H, Ungrin M, et al. (2021) Unique metabolic phenotype and its transition during maturation of juvenile male germ cells. FASEB J 35(5): e21513.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty