Frequency and Antimicrobial Susceptibility Pattern of Pseudomonas Aeruginosa in Human Pus Samples at Holy Family Hospital Rawalpindi
Background: Nosocomial infections are great threat for hospitalized patients and Pseudomonas aeruginosa has emerged as one of the most potent nosocomial pathogens along with its diverse mechanisms to counter the various antimicrobial agents such as aminoglycosides, fluoroquinolones, monobactems, third generation cephalosporins, carbapenams and broadspectrum penicillins. P. aeruginosa is one of the well-known pyogenic bacteria and is 3rd leading cause of pyogenic infections with the variable frequency depending on geographical region and clinical setting. P. aeruginosa is intimately associated with pyogenic nosocomial infections. Objectives: Since multidrug resistant strains of P. aeruginosa have posed serious threats and are frequently implicated in nosocomial infections. Methods: Pus swab were sampled under aseptic conditions and cultured on blood and Muller Hinton agar. Gram reaction, pigment production, Oxidase, indole reaction and citrate test were used to confirm isolate. Antibiotic susceptibility was performed b Kirby Bauer technique. Results compiled by us in this cross sectional study, showed 58 cases of P. aeruginosa out of 289 cases. This included 43% males and 57% females. Majority of the patients were of young age, with mean age 38 years. Antibiotic sensitivity revealed resistance to gentamicin was 50%, amikacin was 64%, ciprofloxacin and Aztronem 66%, Cefaparazone 69%, Tzaocin 71% and meropenem and sulzone was 79%. While Colistin and Ceftazidime were the most effective in 85% and 89% of cases respectively. The multidrug resistant strains of P. aeruginosa infections accounted for 32.76% of total P. aeruginosa infections. This study reveals high prevalence of multidrug resistant organisms at the set of our study. Based on this study, we suggest adopting the strategies to minimize the risk of nosocomial infections to slow down the rapidly growing multidrug resistance. These strategies may include, stricter antiseptic measures, fastening the recovery process and reducing the hospital stay and considering other alternates. Besides this, we would like to suggest the precise use of antibiotic susceptibility facility to reduce the nosocomial infection associated complications.
Introduction
Pseudomonas aeruginosa (P. aeruginosa) is a Gram- negative rod, is a part of our non-glucose fermenting normal microbial flora and widely distributed in natural environments (such as water and soil) [1]. It resides as an opportunistic pathogen, mostly involved in nosocomial infections in the immunocompromised patients [2]. P. aeruginosa is one of the well-known pyogenic bacteria and it is one of the leading causes of pyogenic infections with the variable frequency depending on geographical region and clinical setting. P. aeruginosa is intimately associated with pyogenic nosocomial infections as it is commonly found in hospital instruments [3]. The pyogenic infections caused by P. aeruginosa are characterized by the production of green- blue, foul smelling pus [4]. In the United States, every year 51,000 bacterial infections and 440 deaths are attributed to P. aeruginosa infections [5].
With the passage of time, P. aeruginosa has emerged as one of the most potent nosocomial pathogens along with its diverse mechanisms to counter the various antimicrobial agents such as aminoglycosides, fluoroquinolones, monobactems, 3rd generation cephalosporins, carbapenams and broad-spectrum penicillins [6]. The resistance to the above-mentioned antibiotics is attributed to low permeability of cell wall, production of inducible cephalosporinase, an active efflux and poor activity for target [7]. Studies suggest that the susceptibility pattern of P. aeruginosa depends on the site/specimen from which it is isolated. The multidrug resistance P. aeruginosa predominates in pus specimens [8]. The multidrug resistant P. aeruginosa infections account for 13% of total P. aeruginosa infections [5].
Since multidrug resistant strains of P. aeruginosa have posed serious threats and are frequently implicated in nosocomial infections. Risk factors for multidrug resistant P. aeruginosa infection include prolonged hospitalization, exposure to antimicrobial therapy and immunocompromised states. The increasing frequency of multidrug resistant strains has been the cause of concern for not only clinicians but also for microbiologists [9]. In the field of Microbiology, it is necessary to periodically assess the pathogenic characteristics/properties of microorganisms in order to keep an eye on the arsenal of resistance mechanisms they possess. Antimicrobial sensitivity testing is the cornerstone in the treatment of bacterial infections. With the passage of time, bacteria have developed resistance to various antimicrobial agents which has resulted in greater mortality and morbidity associated with infectious diseases. The present study is aimed to find out the frequency and antimicrobial susceptibility pattern of P. aeruginosa isolated from pus specimens. The study would enable physicians and microbiologists to detect the trends in the susceptibility profile of P. aeruginosa to commonly prescribe antipseudomonal antibiotics.
Materials and Methods
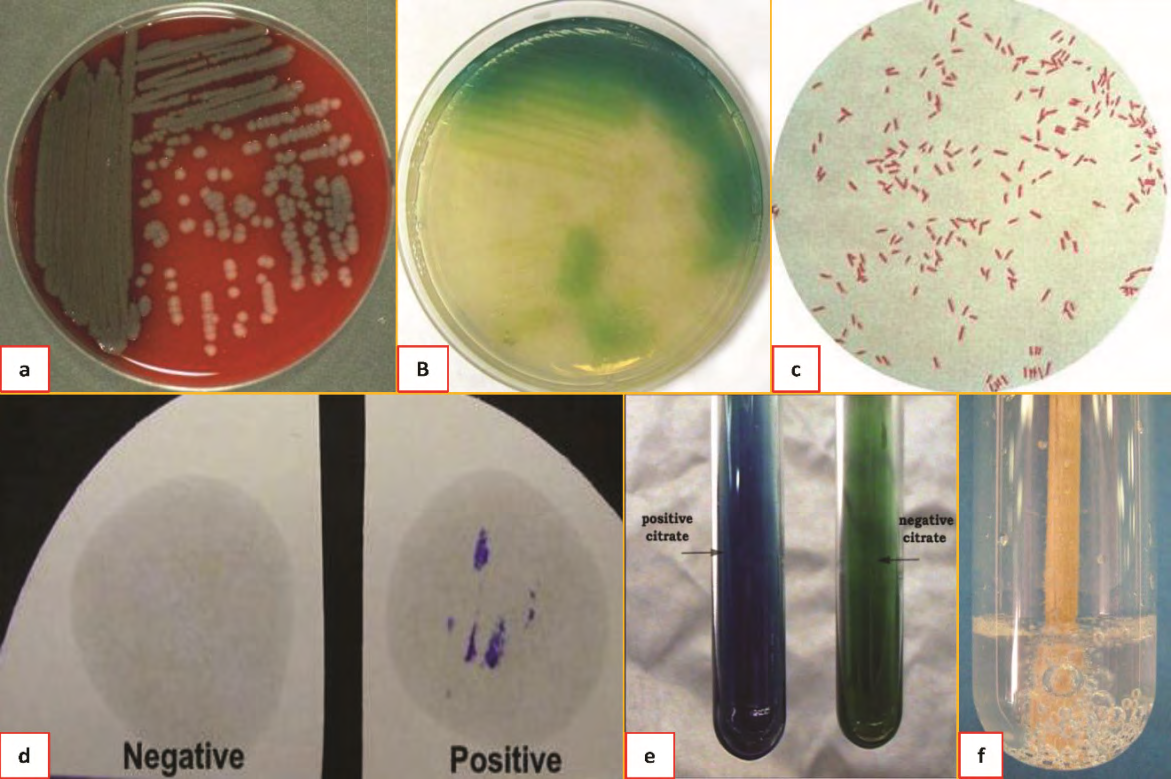
The study was a cross-sectional observational study carried out at the Department of Microbiology, Holy family Hospital, Rawalpindi which is a tertiary care hospital between April and December 2020. Two hundred and eighty-nine patients suspected with pyogenic infections were included in the study population irrespective of their age and gender. All pus specimens/swabs were collected passible aseptic conditions, irrespective of oozing site. Non- probability convenient sampling technique was used for sampling. Study was concluded after ethical approval from the ethical committee of Rawalpindi Medical University and Allied Hospitals Rawalpindi. For the identification of isolates, pus specimens were cultured on Blood agar and MacConkey’s agar plates and incubated aerobically at 37°C for 24 to 48 hours. The plates were observed after overnight incubation for growth which was identified by colony morphology, Gram staining and biochemical characteristics. In-addition isolates were also identified by commercially available API 20NE (BioMerieux, France). Moreover, isolates were identified as Pseudomonas aeruginosa on the basis of colony morphology, Gram staining, oxidase positivity, nitrate reduction, positive catalase test, production of pyocyanin pigment, citrate utilization and ability to grow at 42°C.
The inoculum for susceptibility testing was prepared by touching the top of colonies of isolates with sterile wire loop and suspended in 0.5ml of broth (Equal to 0.5 McFarland standards). The susceptibility testing was performed by Modified Kirby Bauer disc diffusion method on Muller Hinton agar as per previously reported criteria [10, 11]. The antibiotic disks were purchased from Oxoid, England. The surface of Muller Hinton agar plate was inoculated by streaking the plate with swab moistened with inoculum. The antibiotic disks were placed on the surface of streaked Mueller Hinton agar plate. The disks were placed about 15 mm away from the edge of the plate and 24 mm from each other.
The antibiotic disks used were; gentamicin (10µg), amikacin (30µg), ciprofloxacin (5µg), aztreonam (30µg), ceftazidime (30µg), cefoperazone (75µg), tazocin (10µg), meropenam (10µg), colistin (10µg) and sulzone (105µg). The plates were incubated at 37°C for 24 hours. The plates were examined and zone sizes were measured with ruler after overnight incubation. P. aeruginosa American type control culture (ATCC) 27853 was used as quality control for susceptibility testing. The numerical data was entered in SPSS (version 20) software. Coding of variables was done to facilitate data analysis (Figure 1 & Table 1).
| Antibiotic Disk | Disk Content (In µg) | Diameter of zone (in millimeters) | ||
|---|---|---|---|---|
| Sensitive (S) | Intermediate (I) | Resistant (R) | ||
| Gentamicin | 10 | ≥15 | 13-14 | ≤12 |
| Amikacin | 30 | ≥17 | 15-16 | ≤14 |
| Ciprofloxacin | 5 | ≥21 | 16-20 | ≤15 |
| Aztreonam | 30 | ≥22 | 16-21 | ≤15 |
| Ceftazidime | 30 | ≥18 | 15-17 | ≤14 |
| Cefoperazone | 75 | ≥21 | 16-20 | ≤15 |
| Tazocin | 10 | ≤21 | 18-20 | ≤17 |
| Colistin | 10 | ≥11 | _ | ≤10 |
| Meropenam | 10 | ≥19 | 16-18 | ≤15 |
| Sulzone | 105 | ≥21 | 20-18 | ≤17 |
Table 1: Kirby Bauer Disk Diffusion Technique, Zone Diameter According to CLSI Guidelines.
Results
Frequency of P. Aeruginosa in Pus Specimens
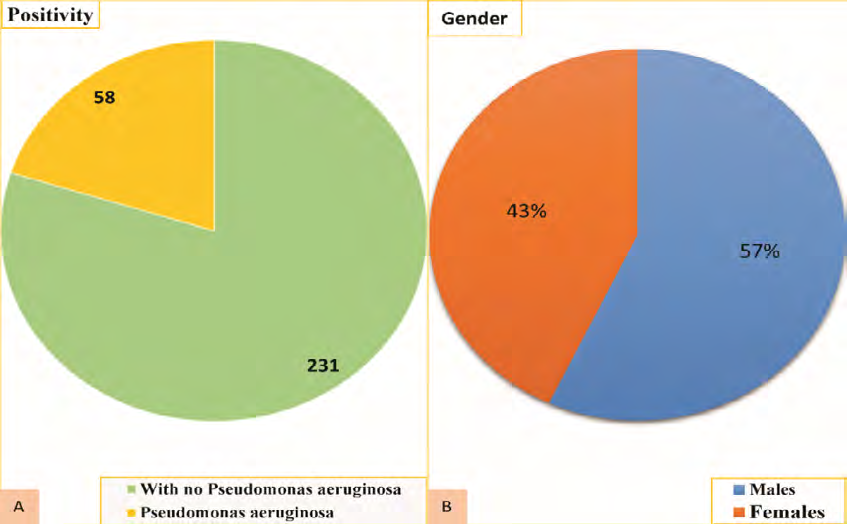
Out of 289 positive pus samples, 58 were identified as P. aeruginosa with the frequency of 20% (58 x 100/289 = 20%) (Figure 2a).
Gender-wise Distribution
Gender-wise distribution showed that out of 58 isolates of P. aeruginosa, 33 (57%) were from males and 25 (43%) from females (Figure 2b).
Age-wise Distribution
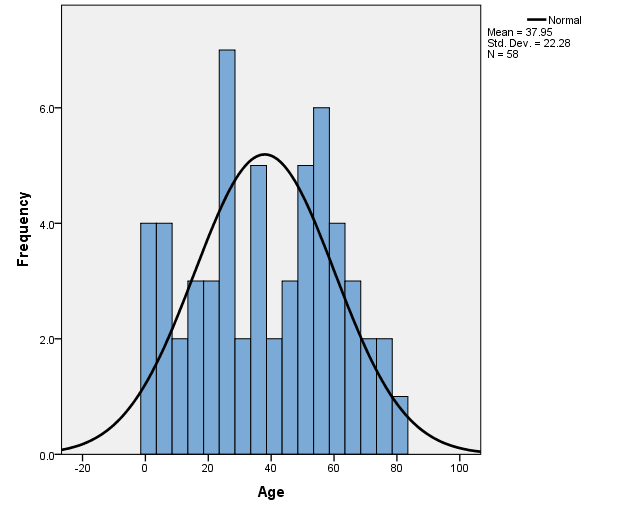
The age distribution of patients ranged from 1 year to 80 years with mean age of approximately 38 years and standard deviation of 22.28. Patients belonging to the age group ≥ 50 years showed highest incidence of P. aeruginosa infections followed by age group ≤ 10 years (Figure 3).
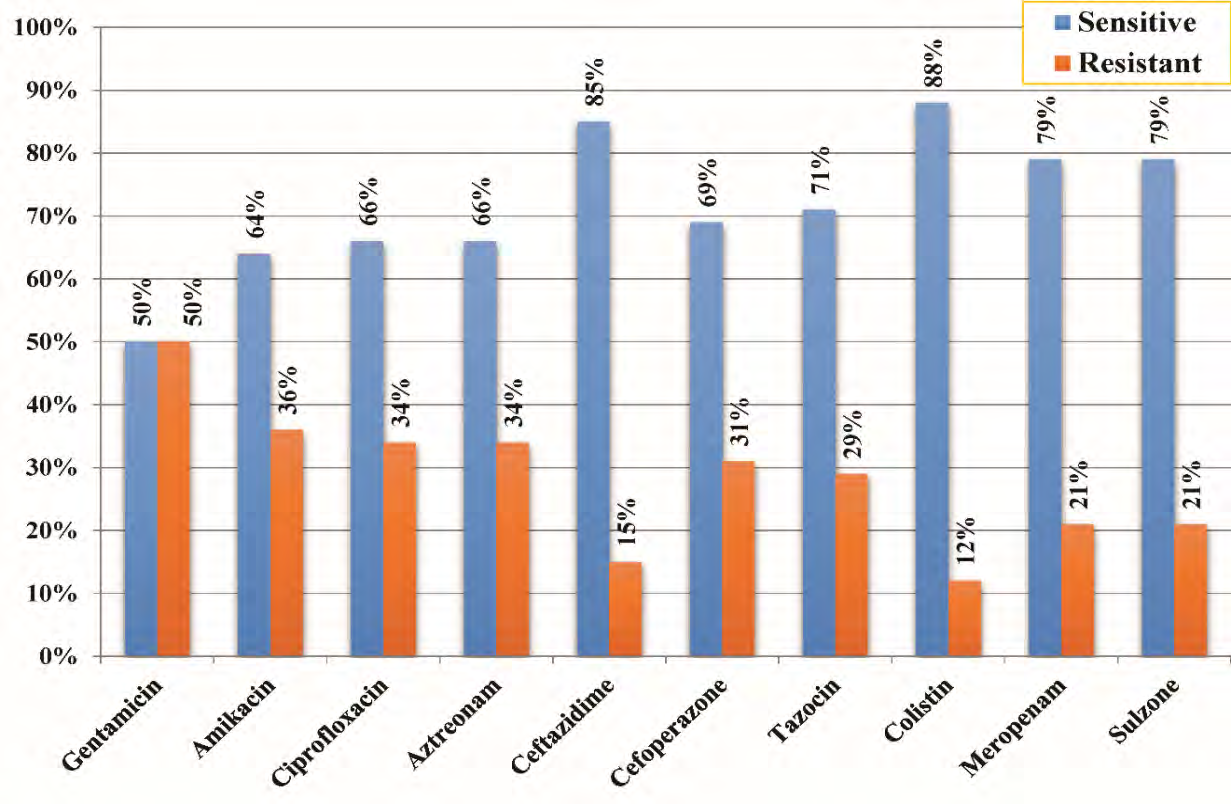
Antimicrobial Susceptibility Profile of P. Aeruginosa Isolated from Pus Specimens Antimicrobial sensitivity testing of P. aeruginosa isolates revealed that colistin and ceftazidime are the most potent antipseudomonal antibiotics. About 88% isolates were found to be susceptible to colistin and 85% to ceftazidime. Meropenam and sulzone also showed considerable antipseudomonal activity as 79% isolates were susceptible to each antimicrobial agent. Among the ten antimicrobial agents used in study, gentamicin showed poorest activity with only 50% isolates being susceptible to it. 66% isolates showed susceptibility to ciprofloxacin and aztreonam and tazocin showed antipseudomonal activity against 71% isolates and cefoperazone to 69% isolates. (Figure 4 & 5) Out of 58 isolates of P. aeruginosa, 19 were multidrug resistant strains. According to CDC, strain of P. aeruginosa is classified as multidrug resistant if it is simultaneously resistant to at least three classes of antimicrobial agents including beta- lactams, aminoglycosides, fluoroquinolones, monobactems and polymyxins (Table 2).
| Antibiotic | Sensitive (%age) | Resistant (%age) |
|---|---|---|
| Gentamicin | 50% | 50% |
| Amikacin | 64% | 36% |
| Ciprofloxacin | 66% | 34% |
| Aztreonam | 66% | 34% |
| Ceftazidime | 85% | 15% |
| Cefoperazone | 69% | 31% |
| Tazocin | 71% | 29% |
| Colistin | 88% | 12% |
| Meropenam | 79% | 21% |
| Sulzone | 79% | 21% |
Table 2: Showing susceptibility profile of P. aeruginosa isolated from pus specimens.
Discussion
Treatment of infection diseases are a great challenge for medical sciences during this evolving state of infectious agents. Very often, infectious diseases are associated with mortal/morbid complication or disabilities [12, 13]. P. aeruginosa is common in the environment, which belongs to the Pseudomonadaceae family. It remains to be a major opportunistic pathogen especially of infections of nosocomial origin. It is considered as one of the most challenging pathogens globally because of its high rate of resistance to antimicrobial agents. The injudicious use of antibiotics in our country has resulted in increased resistance to commonly prescribed antibiotics which have consequently greater mortality and morbidity as well as high cost to treat infectious diseases. The gender distributions of our study showed that 57% of isolates were from males while the other 43% from females. This finding is consistent with studies around the globe which reported the higher isolation rate from males and it is supported by study from Iraq and a study from Karachi [8, 14].
According to our study, among 289 positive isolates, 58 were identified as P. aeruginosa. The frequency of P. aeruginosa in pus specimens is calculated to be 20% which is in agreement with study from India by Verma [4] who reported the frequency of P. aeruginosa in pus specimens to be 18%. The similar frequency i.e. 19% was obtained by Ojentibeju and Nwobu [15] from Nigeria. Another study from Nigeria revealed that the frequency of P. aeruginosa in pus specimens was 11% which is not in agreement with our study Idowu et al., [16]. Considerably different results were obtained by Ranjan, et al. [17] from India, who concluded that P.aeruginosa has the frequency of 30% in pus specimens. Jamsahaid, et al. [14] from Pakistan determined the frequency around 6.67% which is very less as compared to our results. From America, Masaadeh, et al. [18] found that the frequency of P. aeruginosa was 28%. Aminizadeh and Sadat [19] from Iran reported the prevalence of P. aeruginosa as 13.2%.
According to results of our study, gentamicin was found to be the least effective antibiotic against P. aeruginosa. Among 58 isolates tested, half of P. aeruginosa isolates (50%) were susceptible while other half (50%) were resistant to gentamicin which indicates the development of resistance to it. A study from Karachi reported the susceptibility of 59% isolates of P. aeruginosa to gentamicin [20] while from India a researcher reported the susceptibility of 60% isolates to gentamicin [21]. However, a very high rate of susceptibility was shown by gentamicin as reported from Malaysia (85% isolates susceptible) and United Kingdom (87% isolates susceptible) which is quite a higher susceptibility rate as compared to our results [22, 23].
In this study, we found that 64% isolates tested were susceptible while 36% isolates showed resistance to amikacin. Our results are in concordance with results of study from Karachi which reported the same susceptibility rate (64% isolates susceptible) of amikacin to P. aeruginosa isolates [20]. Similar study from Egypt revealed that resistance to amikacin was 44% [24]. In contrast, a very high susceptibility rate of 94% with 652 isolates susceptible out of 692, was reported from Japan and low susceptibility rates of 18% was reported from Iraq [8, 25]. In our study, 34% isolates were resistant to ciprofloxacin. This resistance rate is in accordance with studies from India and Nepal which reported the resistance rate to be 39% and 28% respectively [21, 26]. A researcher from Karachi also reported the exact same resistance rate i.e. 34% [20]. The resistance rate is 8% in Turkey, 11% in the United Kingdom and 16% in Malaysia which is in contradiction with results of our study [22, 23].
Our study revealed that the resistance rate to aztreonam was 34% which is perfectly in agreement with the resistance rate reported from Japan (32%) and India (39%) [27]. The resistance rate from Iran is reported to be 20% which is less than the resistance rate claimed by our study [28]. According to our study, ceftazidime showed great susceptibility rate against P. aeruginosa isolates. Only 15% isolates were resistant to it. The low resistance rate is comparable to the resistance rate reported from the United Kingdom (11%), Turkey (13%) and Japan (16%) [23, 25]. Significantly higher resistance rates are reported from Iran (69%) and India (70%) which are contradictory to our results [29, 30]. It also highlights the fact that emergence of resistance to third generation cephalosporins like ceftazidime needs immediate attention.
Results of our study revealed that 31% isolates were resistant to cefoperazone. This finding is supported by a study from India which reported the resistance rate of P. aeruginosa isolates to cefoperazone to be 33% [31]. Another study from India contradicts our results and it has reported the resistance rate to be 69% which is way too much as compared to the resistance rate provided by our study [29]. The lower resistance rate (15%) has been reported from the United Kingdom [23]. Tazocin is a combination of penicillin ‘piperacillin’ and beta-lactamase inhibitor ‘tazobactam’. In this study, 29% isolates were found to be resistant to tazocin. The researchers from Japan and India have also reported the similar resistance rates of 29% and 34% respectively [25]. According to a study conducted in India, the resistance rate was reported to be 4% which is not in accordance with results of our study [29].
According to our study, colistin was the most effective antipseudomonal antibiotic as 88% isolates were susceptible to it. Only 12% isolates exhibited resistance to it. Recently a study from India reported the resistance rate to be 13% which is in concordance with results of our study [21]. Researchers from the United Kingdom reported that among 505 clinical isolates of P. aeruginosa, all were susceptible to colistin and none was found resistant to it [23]. Results of our study revealed that meropenam exhibited significant antipseudomonal activity as 79% isolates were susceptible with only 21% isolates exhibiting resistance to it. This finding has been supported by results of other studies from different parts of the world which also reported similar resistance rate. The resistance rate is 16% in India, 21% in Japan and 23% in Malaysia [22, 25, 32]. In a study from Karachi, the resistance rate of P. aeruginosa isolates from patients with chronic suppurative otitis media was 24% [33]. A study from Egypt has reported a very high resistance rate of 68% to meropenam by P. aeruginosa isolates which contradicts the with the result of our study [34].
Sulzone is a combination of cephalosporin ‘cefoperazone’ and beta-lactamase inhibitor ‘sulbactam’. According to our study, the resistance rate to sulzone was found to be 21% which indicates a significant activity against the P. aeruginosa isolates. Studies from Japan and India validate our results as they have reported the resistance rate to be 22% [21, 27]. The resistance rate in Nepal has been reported to be 34% and in the United Kingdom 40% which is higher than the resistance rate revealed by this study [23]. According to our study, among 58 isolates of P. aeruginosa, 19 were classified as multidrug resistant i.e. resistant to at least 3 different classes of antimicrobial agents. The prevalence of MDR P. aeruginosa was found out to be 32.7%. Researchers from Iran revealed the prevalence of MDR P. aeruginosa to be 28% which is slightly less than prevalence found by our study [28]. A study from Malaysia reported the prevalence of MDR P. aeruginosa to be 19.6% as 19 isolates out of 97 were multidrug resistant [22]. Another study from India has reported a higher prevalence (45.2%) of MDR P. aeruginosa. Out of 53 isolates, 24 were found out to be multidrug resistant [35]. The prevalence of MDR P. aeruginosa has been reported to be 42.3% in burn patients which is not in accordance with our results [30].
Conclusion
We can conclude from our study that the frequency of P. aeruginosa isolated from pus specimens is 20%. Antimicrobial susceptibility pattern of P. aeruginosa isolates showed that colistin is the most effective antimicrobial agent against P. aeruginosa followed by ceftazidime, meropenam and sulzone. None of the antimicrobial drugs exhibited 100% susceptibility rate. Gentamicin is found to be least effective. Moderate antipseudomonal activity is shown by other antimicrobial agents such as ciprofloxacin, aztreonam and amikacin. Low resistance rate is obtained against cefoperazone and tazocin. Study also revealed the prevalence of MDR P. aeruginosa. 32.7% isolates are classified as MDR strains.
Findings of study need to be interpreted in the light of certain limitations as under.
- Results are limited to the individuals assessing to the Pathology department of Holy Family Hospital Rawalpindi. So, results of study cannot be generalized to the overall population.
- Modified Kirby Bauer disk diffusion method was used for Antimicrobial susceptibility testing. Further studies may be carried out using MIC by either broth or agar dilution which is standard procedure.
- Study was conducted by using a small sample size. Studies with large sample size are required to accurately assess the susceptibility profile of isolates.
References
-
Fazeli H, Akbari R, Moghim S, Narimani T, Arabestani MR, et al. (2012) Pseudomonas aeruginosa infections in patients, hospital means, and personnel’s specimens. J Res Med Sci 17(4): 332-337.
-
Zhapouni A, Farshad S, Alborzi A (2009) Pseudomonas aeruginosa: burn infection, treatment and antibacterial resistance.
-
Singh G, Taneja S (2020) Study Of Most Common Bacterial Isolates Causing Pyogenic Infections. European Journal of Molecular & Clinical Medicine 7(7): 4029-4041.
-
Verma P (2012) A study on isolation of different type of bacteria from pus. International Journal of Pharmacy & Life Sciences 3(11): 2107-2110.
-
Solomon SL, Oliver KB (2014) Antibiotic resistance threats in the United States: stepping back from the brink. Am fam physician 89(1): 938-941.
-
Giamarellou H, Kanellakopoulou K (2008) Current therapies for Pseudomonas aeruginosa. Crit care clin 24(2): 261-278.
-
Al-Tawfiq JA (2007) Occurrence and antimicrobial resistance pattern of inpatient and outpatient isolates of Pseudomonas aeruginosa in a Saudi Arabian hospital: 1998-2003. Int J Infect Dis 11(2): 109-114.
-
Al-Marzoqi AH, Al Taee ZM (2013) Pseudomonas aeruginosa: Antibiotic resistance pattern to different isolates in Al-Hillah city, Iraq. Journal of Natural Sciences Research 3(3): 69-74.
-
Aloush V, Navon-Venezia S, Seigman-Igra Y, Cabili S, Carmeli Y (2006) Multidrug-resistant Pseudomonas aeruginosa: risk factors and clinical impact. Antimicrob Agents Chemother 50(1): 43-48.
-
Khan MI, Xu S, Ali MM, Ali R, Kazmi A, et al. (2020) Assessment of multidrug resistance in bacterial isolates from urinary tract-infected patients. Journal of Radiation Research and Applied Sciences 13(1): 267-275.
-
Humphries RM, Abbott AN, Hindler JA (2019) Understanding and Addressing CLSI Breakpoint Revisions: a Primer for Clinical Laboratories. J Clin Microbiol.
-
Almani MIK, Kazmi A, Mansoor R (2012) Prevalence of Diabetes Mellitus in Patients of Chrpnic Hepatitis C. Journal of Islamabad Medical & Dental College 1: 183- 186.
-
Khan MI, Kalsoom F, Batool F, Kazmi A, Zahra Q-u-a, et al. (2020) Undiagnosed Hepatitis B and C Virus Infection at a Teaching Hospital in Rawalpindi. J Pure Appl Microbiol 14(2): 1279-1286.
-
Khan JA, Iqbal Z, Rahman SU, Farzana K, Khan A (2008) PREVALENCE AND RESISTANCE PATTERN OF PSEUDOMONAS AERUGINOSA AGAINST VARIOUS ANTIBIOTICS. Pak J Pharm Sci 21(3): 311-315.
-
Oguntibeju O, Rau N (2004) Occurrence of Pseudomonas aeruginosa in post-operative wound infection. Pak J Med Sci 20(3): 187-191.
-
Idowu AO, Oluremi BB, Seidu NI (2011) Incidence and susceptibility pattern of clinical isolates from pus producing infection to antibiotics and Carica papaya seed extract. Afr J Biotechnol 10(9): 1700-1704.
-
Ranjan KP, Ranjan N, Bansal SK, Arora D (2010) Prevalence of Pseudomonas aeruginosa in post-operative wound infection in a referral hospital in Haryana, India. J Lab Physicians 2(2): 74.
-
Masaadeh HA, Jaran AS (2009) Incident of Pseudomonas aeruginosa in post-operative wound infection.Am J Infect Dis 5: 1-6.
-
Aminizadeh Z, Kashi MS (2011) Prevalence of multi- drug resistance and pandrug resistance among multiple gram-negative species: experience in one teaching hospital, Tehran, Iran. Int Res J Microbiol 2(3): 90-95.
-
Naqvi ZA, Hashmi K, Rizwan QM, Kharal SA (2005) Multidrug resistant Pseudomonas aeruginosa: a nosocomial infection threat in burn patients. Pak J Pharmacol 22(2): 9-15.
-
Ramana BV, Chaudhury A (2012) Antibiotic resistance pattern of Pseudomonas aureuginosa isolated from healthcare associated infections at a tertiary care hospital. J Sci Soc 39(2): 78-80.
-
Pathmanathan SG, Samat NA, Mohamed R (2009) Antimicrobial susceptibility of clinical isolates of Pseudomonas aeruginosa from a Malaysian Hospital. Malays J Med Sci 16(2): 27-32.
-
Raja NS, Singh NN (2007) Antimicrobial susceptibility pattern of clinical isolates of Pseudomonas aeruginosa in a tertiary care hospital. J MicrobiolImmunol Infect 40(1): 45-49.
-
Gad GF, El-Domany RA, Ashour HM (2008) Antimicrobial susceptibility profile of Pseudomonas aeruginosa isolates in Egypt. The Journal of Urology 180(1): 176- 181.
-
Fujimura T, Anan N, Sugimori G, Watanabe T, Jinushi Y, et al. (2009) Susceptibility of Pseudomonas aeruginosa clinical isolates in Japan to doripenem and other antipseudomonal agents. Int J Antimicrob Agents 34(6): 523-528.
-
Anil C (2013) Antimicrobial susceptibility patterns of Pseudomonas aeruginosa clinical isolates at a tertiary care hospital in Kathmandu, Nepal. Asian J Pharm Clin Res 6(S3): 235-238.
-
Tsuji A, Kobayashi I, Oguri T, Inoue M, Yabuuchi E, et al. (2005) An epidemiological study of the susceptibility and frequency of multiple-drug-resistant strains of Pseudomonas aeruginosa isolated at medical institutes nationwide in Japan. J Infect Chemother 11(2): 64-70.
-
Tavajjohi Z, Moniri R (2011) Detection of ESBLs and MDR in Pseudomonas aeruginosa in a tertiary-care teaching hospital. Arch J Clin Infect Dis 6(1): 18-23.
-
Srinivas B, Devi D, Rao B (2012) A prospective study of Pseudomonas aeruginosa and its antibiogram in a teaching hospital of rural setup. J Pharm Biomed Sci 22: 1-5.
-
Nikokar I, Tishayar A, Flakiyan Z, Alijani K, Rehana- Banisaeed S, et al. (2013) Antibiotic resistance and frequency of class 1 integrons among Pseudomonas aeruginosa, isolated from burn patients in Guilan, Iran. Iran J Microbiol 5(1): 36-41.
-
Bhatiani A, Chandna A (2015) Antibiotic resistance pattern in Pseudomonas Aeruginosa isolated at a tertiary care hospital. Journal of Evolution of Medical and Dental Sciences 4: 12169-12174.
-
Mohanasoundaram K (2011) The antimicrobial resistance pattern in the clinical isolates of Pseudomonas aeruginosa in a tertiary care hospital; 2008-2010 (A 3 year study). Clinic Diagnost Res J 5(3): 491-494.
-
Mansoor T, Musani MA, Khalid G, Kamal M (2009) Pseudomonas aeruginosa in chronic suppurative otitis media: sensitivity spectrum against various antibiotics in Karachi. J Ayub Med Coll Abbottabad 21(2): 120-123.
-
Kamel GM, Edeen NA, Yousef El-Mishad M, Ezzat RF (2011) Susceptibility pattern of Pseudomonas aeruginosa against antimicrobial agents and some plant extracts with focus on its prevalence in different sources. Global Veterinaria 6(1): 61-72.
-
Amutha R, Padmakrishnan MT, Renuga Devi M (2009) Studies on multidrug resistant Pseudomonas aeruginosa from pediatric population with special reference to extended spectrum beta lactamase. Indian J Sci Technol 2(11): 11-13.
- Antifungal Activity of New Acetophenone Derivatives
- Interconnected Microbiomes Human Health Within an Environmental Framework
- Silkworm-Based Vaccine Production for H5N1: A One Health Approach to Pandemic Preparedness
- Microbial Diversity and Lipolytic Activity of Bacteria and Fungi from Oil-Contaminated Sites in Makurdi Metroplois
- Antibiotic Resistance Profile of Bacteria Isolated at the Central Laboratory of the National Hospital Center of Nouakchott
- Epidemiology and Sensitivity to Antibiotics of Germs Isolated from Blood Cultures in the Laboratory of the National Hospital Center of Nouakchott-Mauritania