Prevalence of Extended Spectrum Beta-Lactamase Producing Enterobacteriaceae Isolated From Clinical Samples in Illorin Metropolis, Kwara State Nigeria
Background: This study investigated the prevalence of extended spectrum beta-lactamase producing enterobacteriaceae in Illorin metropolis using standard methods. The prevalence of ESBLs is increasingly being reported worldwide, and it varies according to geographic location and is directly linked to the use and misuse of antibiotics extended spectrum lactamases (ESBLs) are a major challenge in hospitalized patients worldwide and cause epidemic outbreaks in health care facilities, spreading in the community leading to various infections. Objectives: Screen for the extended spectrum β-lactamase producing Enterobacteriaceae and also determine the prevalence of ESBL producing Enterobacteriaceae in relation to gender, age and sample source. Methods: One hundred and sixty eight samples collected from routine clinical specimen such as high vagina swabs, urine, urethra swabs and wound swabs and sputum from October to December 2018 were studied. Fifty two enterobacteriaceae were isolated using spread plate method on macConkey and Cystein lactose electrolyte deficient media. The organisms were Klebsiella pneumoniae, Escherichia coli, Salmonella sp, Shigella sp, and Proteus sp. The isolates were subjected to antibiotic susceptibility testing using modified Kirby-Bauer standardized disc diffusion method. The antibiotics used were ceftazidine (30ug), cefuroxime (30ug), gentamicin (10ug), ciprofloxacin (5ug), ofloxacin 5ug, amoxicillin/clavulanate 30ug, nitrofurantoin 30ug and ampicillin 10ug. Ceftazidime showed a susceptibility percentage of 84.6%,, cefuroxime 61.5%, gentamicin 71.2% ciprofloxacin 46.2%, ofloxacin 51.9%, augmentin 61.5%, nitrofurantoin 71.2% and ampicillin, 44.2% with a significant difference (P< 0.05).Extended spectrum beta-lactamase ESBL, production by clinical and laboratory standards institute (CLSI) methods showed that 15(28.9%) of isolates belonging to the genera Escherichia, Klebsiella and Proteus expressed ESBL production. The order of ESBL production by the isolates were Escherichia coli 9 (17.3%), Klebsiella pneumonia 5(9.3%) and Proteus 1(1.9%). Thus, attention needs to be given by health care personnel’s to ESBL producing organisms in order to reduce the spread.
Introduction
A major threat in human health care is drug resistance by the microorganisms [1, 2, 3]. The rise in the incidence of antibiotic resistant bacteria is of trepidation not only to health care givers but also patients, due to outcomes such as; treatment ineffectiveness, delayed patients’ stay in hospital and nosocomial infections [4, 5]. Drug resistance among Enterobactericeae is largely ascribed to its production of β-lactamase enzyme that can hydrolyze or inactivate the β-lactam drugs that obstruct bacterial cell wall synthesis [6]. β-lactam drugs include the antibiotics penicillins, cephalosporins, cephamycins, carbapenems, monobactams and β-lactamase inhibitors [7]. Infections produced by members of Enterobacteriaceae such as Escherichia coli and Klebsiella Pneumoniae, are most often problematic to treat due to their resistance particularly to β-lactam drugs [8]. Advances in drug technology, brought about new offshoots of β-lactam drugs that are more powerful, broader in spectrum of target organisms and more unaffected by the hydrolytic activity of β-lactamase enzyme. When a new β-lactam drug derivative is derived, new β-lactamase derivatives usually surface, because of the selective pressure associated with the use and abuse of the β-lactam drug. As a result of the increased range of bacterial activity against new expanded- spectrum β-lactams, particularly the cephalosporins, these β-lactamase enzymes have been given the name extended- spectrum β-lactamases (ESBLs) [9]. ESBLs, however, are inhibited by β-lactamase inhibitors such as clavulanic acid [10].
The new β-lactamase derivatives are able to successfully hydrolyse oxymino- cephalosporins and split the amide bond in the β-lactam ring conferring resistance to third generation cephalosporins such as cefotaxime, ceftazidime and ceftriaxone as well as to monobactam such as aztreonam [11]. Extended spectrum lactamases (ESBLs) are a major challenge in plhospitalized patients worldwide and cause epidemic outbreaks in health care centers [12]. Usually, nosocomial outbreaks were linked with previous antibiotic treatments, especially ceftazidime monotherapy. Hospital colonization by ESBL producing bacteria is often a complicated phenomenon involving many different mechanisms, distribution of several epidemic strains and transfer of plasmids and resistant genes [11]. Specific risk factors include; prolonged hospital stay, severity of illness, intensive care unit urinary or arterial catheterization, intubation and mechanical ventilation. ESBL E. coli commonly occur in surgical, frequently from patients from extended care facilities [12].
Increasing frequency of infections caused by antibiotic resistant extended-spectrum β-lactamase (ESBL) producing Enterobactericeae strains needs to be addressed by continuous tailing and accurate recognition for more effective treatments [13]. The prevalence of ESBLs is increasingly being reported worldwide, and it varies according to geographic location and is directly linked to the use and misuse of antibiotics extended spectrum lactamases (ESBLs) are a major challenge in hospitalized patients worldwide and cause epidemic outbreaks in health care facilities, spreading in the community leading to various infections [1]. This study aims to provide information on the prevalence of extended spectrum β-lactamase producing Enterobacteriaceae isolated from clinical samples in Illorin metropolis, kwara state Nigeria. The study would help the health sector to minimize the drug resistance posed by extended-spectrum β-lactamase (ESBL) producing Enterobactericeae.
Materials and Methods
The study was carried out in Ilorin, capital of Kwara State, north-central, Nigeria. Ilorin is divided into four local government areas, Asa, Ilorin East, Ilorin South and Ilorin West. The major activity in the city is commercial in nature, but some are farmers and civil servants. A total of one hundred and sixty-eight clinical specimens were collected in this study, conducted between July 2018 and January 2019 involving 69 high vaginal swabs, 87 urine 5 sputum, 2 wound swabs and 5 urethra swabs. From both male and female patients referred to the medical laboratory. Sterile cotton swabs and universal bottles were used to collect pus, vaginal discharge, urine and sputum from patients using standard techniques. The macroscopic features of the specimen were examined to checkout for colour, turbidity and presence of blood. All specimens were cultured within 3hours of collection.
The specimens were inoculated on nutrient agar, macConkey agar, Cystein Lactose Electrolyte Deficient Agar (CLED) and Eosin methylene blue agar using pour plate and spread plate methods. The plates were incubated at 37°C for 24 hours [14]. The colonies that emerged were counted and subculture onto fresh nutrient agar plates. Biochemical test and morphological characteristics described by Cheesbrough were used to identify pure cultures of the isolates [15]. Antimicrobial Susceptibility test was done using the modified Kirby Bauer disc diffusion method [16]. A suspension made from a 24 h growth of the organisms in saline to match the 0.5 McFarland turbidity standards. This was then seeded on the entire surface of Mueller Hinton agar plates and the antibiotic discs were embedded on the agar. The plates were then incubated at 37°C for 24hours, after which the diameter of zones of growth inhibition around the discs were measured in millimeter (mm). Multiple drug resistant microorganisms were identified as resistant to three or more antibacterial classes. Isolates showing inhibition zones of ≤ 27mm for cefotaxime and ≤ 22 mm for ceftazidime were screened as potential ESBL producers.
The ESBL production was done using Modified Double Disc Synergy Test (MDDS) [17]. Mueller Hinton agar plates were seeded with test organisms pre-adjusted to 0.5 MacFarland standards. A combination disc of amoxicillin (20μg) and clavulanic acid (10μg) was placed at the centre of the plates between two cephalosporin antibiotics 30mm apart. The set up was incubated at 37ºC for 24hours [17]. Any increase in the zone towards the disc of amoxicillin- clavulanate was considered positive for the ESBL production [1]. Data analysis was carried out using the Statistical Package for the Social Sciences (SPSS) version 20 (Armonk, New York: IBM Corp). Results from this study were presented in frequency tables and in percentages. The association between ESBL producing organisms, ESBL non-producing organisms and patient demographics was determined using Chi square test at significance level of P = 0.05 [18].
Results
A total of five (5) bacterial species were identified which include Escherichia coli, Klebsiella pneumoniae, Salmonella, Proteus and Shigella species. The distribution of the isolates obtained were shown in Figure 1 below, where Escherichia coli recorded the highest percentage of 42.3%, Klebsiella pneumoniae of 25%, Salmonella species 9.6%, Shigella species of 17.3% and the least Proteus species of 5.8%. Figure 2 below, shows the susceptibility pattern of the isolated bacteria, high antibiotic resistance was observed in ampicillin, Ciprofloxacin and ofloxacin, 55.8%, 53.8% and 48.1% respectively. Majority of the isolates encountered in this study were multidrug resistant strains showing resistance to 4 to 5 antimicrobials or more. Ciprofloxacin, ampicillin, gentamycin, ofloxacin and nitrofurantoin showed the highest multiple resistance patterns at 33.3%. Figure 3 shows the Plate of ESBL producing Escherichia coli with double disk synergy test while Figures 4 & 5 show the ESBL producing Klebsiella species dish undergoing double disk test and Dump bell inhibition zone of positive double disk synergy test (DDST) characteristics of ESBL producing Proteus respectively.
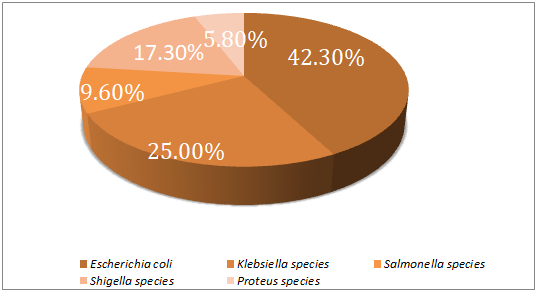
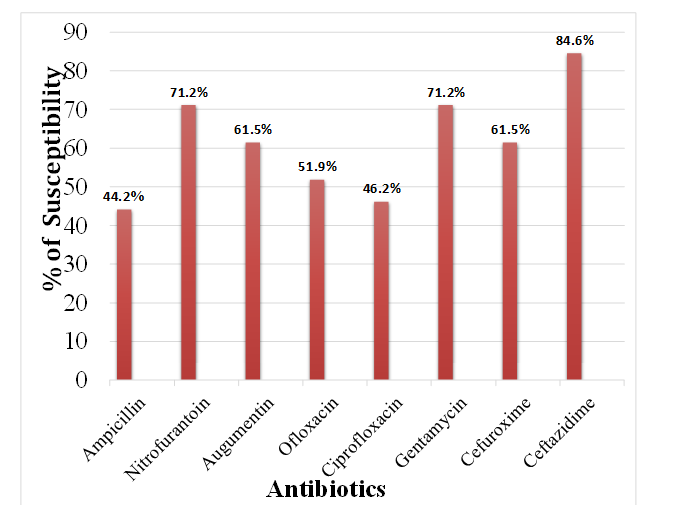
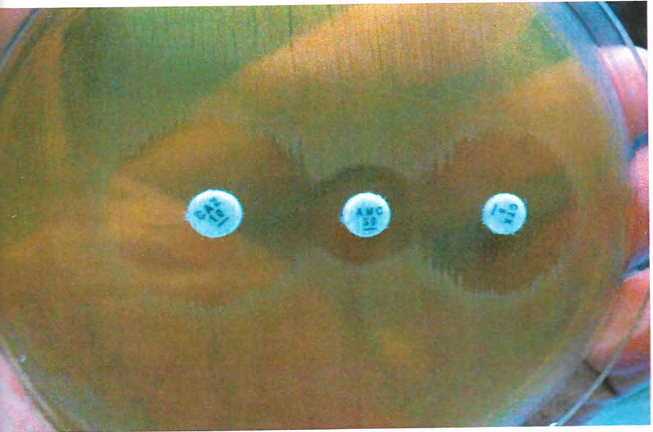
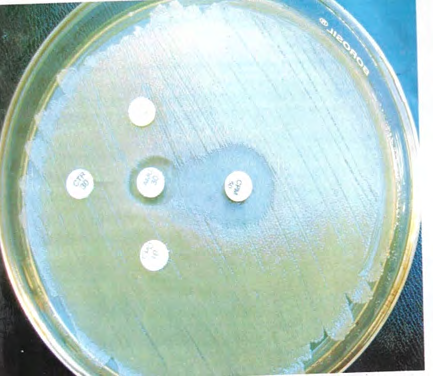
Table 1 below reveals the distribution of extended spectrum Beta-Lactamase (ESBL) producing Enterobactericeae among clinical samples in Ilorin metropolis. Out of 52 isolates, 15 were extended spectrum producing isolates giving a prevalence of 28.9%. Out of these, 15 were extended spectrum beta Lactamase producing isolates, E. coli was the major producer 9(60%) followed by K. pneumoniae, 5(33.3) and the smallest proteus species of 6.7%. The age and gender distribution of extended spectrum beta-lactamase producers showed that age 21-30 years had a relatively high prevalence of 53.3% of ESBL producing isolates than the others.
| Samples | Number Tested | Number of Isolates (ESBL producers) | ||
|---|---|---|---|---|
| Escherichia coli | Klebsiella pneumonia | Proteus species | ||
| High Vaginal Swab | 69 | 6(3) | 5(1) | 0(0) |
| Urine | 87 | 10(4) | 7(3) | 2(0) |
| Sputum | 5 | 1(0) | 0(0) | 0(0) |
| Wound | 2 | 1(1) | 1(1) | 0(0) |
| Urethral Swab | 5 | 3(1) | 0(0) | 1(1) |
| Total | 168 | 22(9) | 13(5) | 3(1) |
Table 1: Distribution of Extended spectrum Beta-Lactamase (ESBL) producing Enterobactericeae among clinical samples in Ilorin met
While females were recorded with a higher rate of 73.3% of ESBL producing isolates as compared to the male counterpart 26.7%. The fact that more ESBL producing organisms were recovered from females than their male counterparts, was however not statistically significant.
Discussion
The prevalence of ESBL-producing organisms has been increasing rapidly worldwide. This situation is alarming because ESBL producers have been reported to exhibit co- resistance to many other classes of antibiotics resulting in limited therapeutic options [13]. In addition, the prevalence of ESBL, type of enzyme, gender and age group of persons affected varies in different geographical areas. In this study, the overall prevalence of ESBL producing isolates from clinical samples was 28.9%. However, the prevalence recorded in this study is much higher than a prevalence of 9.25% recorded amongst genera of Enterobacteriaceae in Muhammad Abdullahi Wase Specialist Hospital, Kano [19].
This is comparable to 39.8% reported in Enugu [20] and 33.6% in Abuja [21]. Higher prevalence rates of 58.6% (Enugu) and 76.9% (Ibadan) have been reported in other Nigerian studies [22]. Global reports show that Pakistan, Sudan and India [23, 24, 25] recorded 29.45%, 59.6% and 57.5% prevalence respectively. The variation in ESBLs prevalence rates reported between geographical areas, institutions and countries may be attributed to the complex epidemiology of ESBLs, specific type of bacteria involved, study design and patient selection and methods used for ESBL detection among other factors [26]. Moreover, geographical differences occur in clinical isolates which are also rapidly changing with time [27].
In this study, E. coli was identified as the major ESBL producer (40.9%) followed by K. pneumoniae (38.5%). E. coli has recently been reported as the major ESBL producer in similar studies conducted in Enugu [20], Osun [28], Ogun States [29], Zaria which reported 50% ESBL E. coli [8] as well as in Bangladesh [30] and Pakistan [24]. However, other Nigerian reports, Ogun [31], Benin [32] and Abuja [13] as well as foreign reports of Ghana [33] and Sudan [25] indicated K. pneumonia as the major ESBL producer. Although both organisms have been identified in various studies within and outside Nigeria as the major ESBL producing microorganisms, there has been no consensus on this has a greater capacity to produce ESBL.
Regarding gender classification, the fact that more ESBL producing organisms were recovered from females than their male counterparts, the difference was however not statistically significant and similar results have been documented elsewhere, Abuja, Nigeria [21] and Pakistan [24]. Young adults of ages 21-30 were among the age brackets with high prevalence of ESBL producing organisms in this study (53.3%). Majority of the isolates encountered in this study were multidrug resistant strains showing resistance to 4 to 5 antibiotics or more. The gross misuse or over-use of antimicrobials in the hospital, non-compliance or adherence of antimicrobial use by patients, could lead to development of multidrug resistant bacteria [20]. The existence of ESBL- producers in an individual could lead to increased antibiotic resistance because the plasmid which carries the ESBL enzymes also harbors resistance genes to other classes of antimicrobials [13].
In the west, the ESBL production in Enterobacteriaceae varies from 5 to 52 per cent and in other Asian countries, it varies from 10 to 46.5 per cent [34]. Other studies from India have reported a high prevalence of the ESBL production, which ranges from 41.0 to 63.6 per cent in E. coli and 40 to 83.3 per cent in K. pneumoniae [35]. ESBLs constitute a serious threat to the β-lactam therapy. Due to the difficulty in their detection by the current clinical methods, many of these strains have been falsely reported to be susceptible to the widely used broad-spectrum β-lactams [36]. The ESBL producers are intrinsically resistant to all the cephalosporins even if they exhibit an in vitro susceptibility [9, 37].
Conclusion
Antibiotic resistance has raised as one of the pre- eminent public health concerns without sufficient attention in developing countries like Nigeria. This study found a high rate of ESBL production (40.9%) in isolated Enterobactericeae with multidrug resistance. This is of great concern in healthcare settings which requires sound, committed and sustainable infectious control measures including antimicrobial management and routine detection of ESBL producing isolates.
References
-
Khan SA, Feroz F, Noor R (2013) Study of extended- spectrum β- lactamase- producing bacteria from urinary tract infections in Bangladesh. Tzu Chi Medical Journal 25(1): 39-42.
-
Hasan R, Acharjee M, Noor R (2016) Prevalence of vancomycin resistant Staphylococcus aureus (VRSA) in methicillin resistant S. aureus (MRSA) strains isolated from burn wound infections. Ci Ji Yi Xue Za Zhi 28(2): 49-53.
-
Cordoba G, Holm A, Hansen F, Hammerum AM, Bjerrum L (2017) Prevalence of antimicrobial resistant Escherichia coli from patients with suspected urinary tract infection in primary care, Denmark. BMC Infect Dis 17(1): 670.
-
Alam SS, Kalam A, Munna S, Munshi SK, Noor R (2014) Isolation of pathogenic microorganisms from burn patients admitted in Dhaka Medical College and Hospital and demonstration of their drug resistance traits. Asian Pacific Journal of Tropical Disease 4(5): 402-407.
-
Oli AN, Eze DE, Gugu TH, Ezeobi I, Maduagwu UN, et al. (2017) Multi-antibiotic resistant extended-spectrum beta-lactamas producing bacteria pose a challenge to the effective treatment of wound and skin infections. Pan Afr Med J 27: 66.
-
Sule H, Kumurya AS (2016) Beta-Lactamase production among uropathogens in patients attending some hospitals in Kano, Nigeria. International Journal of Biomedical Materials Research 4(3): 58-62.
-
Thakuria B, Lahon K (2013) The Beta Lactam Antibiotics as an Empirical Therapy in a Developing country: An update on Their Current Status and Recommendations to Counter the Resistance against Them. J Clin Diagn Res 7(6): 1207-1214.
-
Giwa FJ, Ige OT, Haruna DM, Yaqub Y, Lamido TZ, et al. (2018) Extended-Spectrum beta lactamase production and antimicrobial susceptibility pattern of uropathogens in a Tertiary Hospital in Northwestern Nigeria. Annals of Tropical Pathology 9(1): 11-16.
-
Cruz MC, Hedreyda CT (2017) Detection of plasmid- borneβ-Lactamase genes in extended spectrumβ**-** Lactamase (ESBL) and Non-ESBL-producing Escherichia coli clinical Isolates. Philipine Journal of sciences 146(2): 167-175.
-
Salma J, Karama R (2015) Antibiotics. Journal of Antimicrobial chemotherapy 67(6): 1311-1320.
-
Latifpour M, Gholipour A, Damavandi MS (2016) Prevalence of extended spectrum Beta Lactamase producing Klebsiella pneumoniae isolates in nosocomia and community Acquired urinary Tract Infections. Jundishapur J Microbiol 9(3): e31179.
-
Yahaya M, Gadzama GB, Zailani SB, Aboderin AO (2016) Characterization of extended spectrum beta lactamase from Escherichia coli and Klebsiella species from North Eastern Nigeria. Journal of clinical and diagnostic Research 10(2): DC07-DC10.
-
Azekhueme I, Anietie E, Abbey SD (2015) Extended Spectrum Beta-Lactamases in Clinical Isolates of Escherichia coli and Klebsiella pneumoniae from University of Uyo Teaching Hospital, Uyo, Nigeria. Journal of Advances in Medical and Pharmaceutical Sciences 2(3): 117-125.
-
Bailey WR, Scott EG (2000) Diagnostic Microbiology, Second Edition. Toppan company ltd Japan, pp: 342.
-
Cheesbrough M (2009) District Laboratory Practice in Tropical Countries. 2nd(Edn), Cambridge University Press, UK, pp: 159-163.
-
Bauer AW, Kirby WM, Sherris JC, Turck M (1966) Antibiotic susceptibility testing by a standardized single disk method. Am J Clin Pathol 45(4): 493-496.
-
Magiorakos AP, Srinivasa A, Carey RB, Carmeli Y, Falagas ME, et al. (2012) Multidrug-resistant, extensively drug resistant and pandrug resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect 18(3): 268-281.
-
(2013)Alle Berechnungen wurden mitder Analyse software SPSS Version 22.0, IBM Inc, Armonk NY, USA durchgefuhrt.
-
Yashau M, Aliyu HM, Kumurya AS, Suleiman K (2010) Prevalence of extended spectrum **β-** Lactamases (ESBLs) among Enterobacteriaceae in Murtala Mohammed Specialist Hospital, Kano, Nigeria. Bayero Journal of pure and Appied sciences 3(1): 169-172.
-
Iroha IR, Adikwu MU, Esimone CO, Abinu I, Amadi ES (2009) Extended Spectrum **β** lactamase (ESBL) in E. coli isolated from a tertiary hospital in Enugu state, Nigeria. Pakistan Journal of medical Sciences 25(2): 279-282.
-
Akanbi BO, Ojonuba BD, Njoku R (2013) Detection of extended spectrum **β** lactamase producing Klbesiella pneumniae and Escherichia coli in Two Hospitals in the Federal capita Territory, Abuja Nigeria. Open Journal of Medical Microbiology 3(4): 207-212.
-
Okesola T, Adeniji A (2010) Pattern of extended spectrum beta lactamase production among clinical isolates of Proteus species in Western Nigeria. World journal of medical sciences 5 (4): 94-97.
-
Raiz B, Khatoon H (2013) Evaluation of the use of cephalosporin antibiotics in Pediatrics. Journal of Applied Pharmaceutical sciences 3(4): 63-66.
-
Ahmed OI, El-Hady SA, Ahmed TM, Ahmed IZ (2013) Detection of bla SHV and bla CTXM genes in ESBL producing Klebsiella pneumoniae isolated from Egyptian patients with suspected nosocomia infections. Egyptiasn journal of medical human genetics 14(3): 277-283.
-
Rao R, Sumathi S, Anuradha K (204) Bacteriology of postoperative wound infections. International J Pharma Biomed Res 4(2): 72-76.
-
Khalaf NG, Eletreby MM, Hanson ND (2009) Characterization of CTX-M ESBLs in Enterobacter cloacae, Escherichia coli and Klebsiella pneumonia clinical isoates from Cairo, Egypt. BMC Infect Dis 9: 84.
-
Bajpai T, Pandey M, Varma M, Bhatambare GS (2014) Prevalence of extended spectrum beta lactamase producing uropathogens and their antibiotic resistance profile in patients visiting a tertiary care hospital in central India: Implications on empiric therapy. Indian J Pathol Microbiol 57(3): 407-412.
-
Ogbolu DO, Daini OA, Ogunledun DA, Terry OAT, Webber MA (2013) Dissemination of Inf plasmids carrying beta- lactamase genes in gram negative bacteria from Nigerian hospitals. J Infect Dev Ctries 7(5): 382-390.
-
Adeyankinnu FA, Motayo BO, Akinduti A, Akinbo J, Ogiogwa JI, et al. (2014) A Multicentre study of beta lactamase Resistant Escherichia coli and Klebsiella pneumoniae Reveals high level chromosome mediated extended spectrum beta lactamase resistance in Ogun state, Nigeria. Interdiscip Perspect Infect Dis pp: 819- 896.
-
Akujobi CN, Ewuru CP (2010) Detection of extended spectrum beta lactamases in gram negative bacilli from clinical specimens in a teaching hospital in South Eastern Nigeria. Niger Medical Journal 51(4):141-146.
-
Olowe OA, Aboderin BW (2010) Detection of extended spectrum beta lactamase producing strains of (Escherichia coli) and (Klebsiella sp) in a tertiary health centre in Ogun state. International Journal of Tropical Medicine 5(3): 62-64.
-
Osazuwa F, Osazuwa E, Osime C, Igharo EA, Imade PE, et al. (2011) Etiological Agents of Otitis media in Benin city, Nigeria. N Am J Med Sci 3(2): 95-98.
-
Hackman HK, Osei-Adjei G, Ameko E, Kutsanedzie F, Gordon A (2013) phenotypic determination and antimicrobial resistance profile of extended spectrum beta lactamase in Escherichia coli and Klebsiella pneumoniae in Accra Ghana. Journal of Natural sciences Research 3(12): 75-83.
-
Dhillon HR, Clark J (2012) ESBLs: A clear and present Danger? Crit Care Res Pract, pp: 625170.
-
Goyal A, Prasad KN, Prasad A, Gupta S, Ghoshal U, et al. (2009) Extended spectrum beta lactamases in Escherichia coli and Klebsiella pneumoniae associated risk factors. Indian J Med Res 129(6): 695-700.
-
Kaur J, Chopra S, Sheevani, Mahajan G (2013) Modified Double Disc synergy Test to Detect ESBL Production in urinary isolates of Escherichia coli and Klebsiella pneumoniae. J Clin Diagn Res 7(2): 229-233.
-
Livermore DM, Canton R, Gniadkowski M, Nordmann P, Rossolini GM, et al. (2007) Changing the face of ESBLs in Europe. J Antimicrob Chemother 59(2): 165-174.
- Antifungal Activity of New Acetophenone Derivatives
- Interconnected Microbiomes Human Health Within an Environmental Framework
- Silkworm-Based Vaccine Production for H5N1: A One Health Approach to Pandemic Preparedness
- Microbial Diversity and Lipolytic Activity of Bacteria and Fungi from Oil-Contaminated Sites in Makurdi Metroplois
- Antibiotic Resistance Profile of Bacteria Isolated at the Central Laboratory of the National Hospital Center of Nouakchott
- Epidemiology and Sensitivity to Antibiotics of Germs Isolated from Blood Cultures in the Laboratory of the National Hospital Center of Nouakchott-Mauritania