Switch from IV to SC Administration of Vancomycin-D-Arginine (STM-001) Maintains Effectivity to Combat NDM-1 E. Coli Burden in a Murine Model of Complicated Urinary Tract Infection (cUTI)
Intravenous (IV)-bolus administered vancomycin-D-arginine (STM-001) was previously shown to be effective against E. coli in a mouse model of complicated urinary tract infection (cUTI) at a putative low, humanized-dose. Herein, we investigated if a switch in its route of administration from IV to SC during a 3-day treatment window, could still maintain the conjugate's antimicrobial effects. Mice were treated with IV STM-001, BID at 50 mg/kg four days following infection driven by a carbapenem-resistant E. coli (NDM-1 positive) strain. Thereafter, identical treatment was maintained with IV or switched to SC on days 5 and 6 or just during day 6. Bacterial burdens in urine were determined kinetically as well as in various organs on day 7. As compared to vehicle groups which ranged throughout from log10 mean (± SEM) of 4.79 ± 0.51 to log10 mean (± SEM) of 5.56 ± 0.53 CFU/mL urine), SC STM-001 treatment groups reduced urinary burden to log10 mean (± SEM) from of 1.89 ± 0.33 to log10 mean (± SEM) 2.47 ± 0.47 CFU/mL, (p < 0.05 Cf. to vehicle), very similar to IV treatment throughout. In kidney, bladder, liver and spleen, irrespective of the mode of administration, STM-001 was highly effective in lowering bacterial load from baseline, ranging from mean log10 1.4 to 2.65 CFU/tissue reductions (p < 0.05). These data underscore the promise of SC-administered STM-001 as an alternative parenteral route to IV administration in the effective targeting of highly resistant E. coli strains. STM-001 could represent an attractive clinical candidate for outpatient subcutaneous antimicrobial therapy (OSCAT) in contrast with demanding outpatient parenteral antimicrobial therapy (OPAT) to treat cUTIs in the clinic
Introduction and Background
Antimicrobial resistance (AMR) is a global pandemic that caused and was associated with 1.27 and 4.95 million deaths worldwide respectively in 2019 [1]. In response to the anticipated annual mortality of 10 million deaths due to AMR by 2050 [2], innovative antibiotics are urgently required which ideally conform to expeditious regulatory paths and offer significantly improved clinical benefits for patients worldwide. Therefore, in contrast to the total syntheses for many antibiotics [3], it would be advantageous if newer antibiotics were amenable for production requiring minimal synthetic steps (e.g. using an approved antibiotic as the bulk, starting material) as well as allowing a more simplified route of parenteral administration (e.g. SC). The latter would allow a swifter clinical application with minimal monitoring, especially for low-dose antibiotics. This is in marked contrast with the majority of approved antibiotics during the last decade which require high doses (10s g), are critically-dependent upon slow IV infusion with the necessity for TID dosing [4]. As a result, such drugs significantly complicate their adaptation for OPAT since extensive clinical management is required (e.g. infectious disease consultants, pharmacy and nursing support) together with much patient education and compliance [5].
E. coli, a priority-1 pathogen [6] is a member of the Enterobacteriaceae family of Gram-negative bacteria and was categorized as the leading death-causing pathogen in the Global Burden report [1]. Indeed, E. coli is the predominant pathogen that drives > 2.8 million annual cases of cUTIs in the USA [7, 8, 9] due to its propensity to generate high levels resistance, including cross-resistance to many first and second-line antibiotics [9, 10, 11]. As a result, cUTIs cause a major financial burden on annual total healthcare costs exceeding $6 billion with inpatient care being a significant contributor [12, 13, 14]. Therefore, antibiotics that might be amenable for SC administration using OSCAT [15, 16], could substitute for OPAT, yielding improved clinical outcomes and reduced healthcare burden. For example, OSCAT could help to avoid unnecessary emergency department (ED) visits, reduce readmissions often associated with OPAT use, lower hospitalization rates and even facilitate early discharge [5, 12].
An interesting vancomycin-L-arginine conjugate that exhibited an unexpected antibacterial activity towards Gram-negative pathogens, yet retained Gram-positive efficacy was initially described in 2019 [17]. Following up from these studies using vancomycin-D-arginine (“STM- 001”), we demonstrated that its physicochemical properties were essentially identical to vancomycin with the exception of the conjugate’s Gram-negative properties towards E. coli, including all resistant types [18]. Inspired by these findings together with many reports demonstrating a very high renal elimination of vancomycin in humans as a nonmetabolized form [18, 19], it seemed a reasonable hypothesis that STM- 001 might be active in a mouse model of E. coli-associated cUTI. Indeed, IV STM-001 was highly effective in combatting urinary and tissue bacterial burdens following infection with fluoroquinolone and carbapenem-resistant E. coli strains [19]. Using the same latter, NDM-1 infecting strain in a follow-up cUTI model herein, we aimed to determine if maintenance therapy with SC administered STM-001 could support its efficacy using a previously defined, optimal dose and dosing regimen [19].
Material and Methods
Animal Ethics
All work conducted at Pharmacology Discovery Services (Taiwan Ltd) complied with the International Guiding Principles for Biomedical Research (CIOMS) under an IACUC that operates according to the “Regulation for Establishing the Committee of Care and Use of Laboratory Animals” (2011).
Vancomycin-arginine (STM-001) Manufacturing
STM-001 was prepared on 50 g scale from commercially available vancomycin HCl (Shanghai Haoyuan, China) and D-arginine amide dihydrochloride (WuXi CSU, Shanghai, China) as previously described [19]. The quality of the API met target specifications (assay >90% on dry basis; any impurity ≤ 2.0%; Total impurity ≤ 8.0%).
AMR Gene of Infecting E. coli Strain for in-vitro and in-vivo Experimental Studies
The E. coli strain AR-BANK#0055 was derived from the CDC and FDA Antimicrobial Resistance (AR) isolate bank [20] and consisted of aac(3)-IIa, aadA5, CMY-6, dfrA17, mph(A), NDM-1, OXA-1, rmtC, sul1 and tet(A) AMR genes.
Antimicrobial Susceptibility Testing
The MICs for STM-001 and colistin against E. coli AR- BANK#0055 were performed as previously described using MHB and CAMHB media respectively [19].
In-vivo Efficacy Studies (Ascending cUTI Model)
The cUTI model using E. coli AR-BANK#0055 was established as previously reported [19] using 60 female C3H/HeJ mice group (7-8 weeks old) with an infecting E. coli dose of log10 9.16 CFUs administered by the transurethral route. Drugs were freshly prepared each day in vehicle (0.9% NaCl) and maintained at 4°C for the second dose. Volumes of drug for IV dosing were 5 mL/kg and for SC, 10 mL/kg. All vehicle or drug interventions were initiated at 4 d post- infection with BID dosing starting from day 4 until the end of day 6, i.e. 6 dosings in total. All animals were sacrificed on day 7. Three groups of 10 mice per group were assigned to the following experimental groups: a) determination of baseline bacterial burden (i.e. 96 h harvesting; Group 1); b) IV 0.9% saline-treated mice (Group 2); c) SC colistin-therapy at a dose of 20 mg/kg (Group 3). STM-001 treatment groups were arranged as outlined: Following treatment of 30 mice with IV STM-001 on day 4, 10 mice were switched to SC therapy during days 5 and 6 (Group 4, IV+SC+SC). Following treatment of the remaining 20 mice with IV STM-001 during day 5, 10 mice received SC STM-001 during day 6 (Group 5, IV+IV+SC) and the remaining 10 animals continued with IV treatment (Group 6, IV+IV+IV). Bacterial burdens were determined kinetically in urine (CFUs/mL) and on day 7, in kidney, bladder, liver and spleen (CFUs/tissue).
Post-challenge, Data and Statistical Analysis
Bacterial counts in urine for the baseline group were determined on day 4 with counts from all experimental groups determined daily from days 5-7. On day 7, animals were humanely sacrificed and appropriate organs aseptically harvested followed by homogenization in 1 mL sterile PBS (pH 7.4) with a Polytron homogenizer. Bacterial burdens in urine and tissue homogenates were determined by plating 10-fold serial dilutions to a nutrient agar plate as previously described [19]. Daily urinary bacterial burden data (CFUs/ ml) for all groups is presented as the mean ± SEM. Statistical differences (p < 0.05) in urinary burden between all treatment groups (i.e. STM-001 groups 4-6 and colistin group 3) as compared to the vehicle (group 2) were determined by one- way ANOVA and Dunnett’s test. For the tissue homogenates, mean ± SEM CFUs/tissue were determined for all groups with the mean value per treatment group deducted from the baseline mean to generate mean log10 reduction in bacterial burden. Statistical differences between treatment groups and the baseline group were determined with one-way ANOVA analysis and Dunnett’s test.
Results
Antimicrobial Susceptibility Testing
The MICs of STM-001 and vancomycin towards AR0055 were 16 mg/L and > 128 mg/L as previously reported [18, 19]. Of 21 additional antibiotics (amikacin, gentamicin, amoxicillin/clavulanic acid, ampicillin/sulbactam, piperacillin/tazobactam, aztreonam, aztreonam/avibactam, cefazolin, cefepime, cefoxitin, ceftazidime, ceftazidime/ avibactam, ceftriaxone, imipenem, imipenem and chelators, meropenem, ciprofloxacin, levofloxacin, colistin, tigecycline and trimethoprim/sulfamethoxazole) taken for screening, only colistin (MIC = 1 mg/L) and tigecycline (MIC = 0.25 mg/L) were active.
Effect of STM-001 on Bacterial Burden in Urine and Tissues
Following establishment of the cUTI model, kinetic plots of E. coli urinary burdens from all 6 experimental groups are shown in Figure 1.
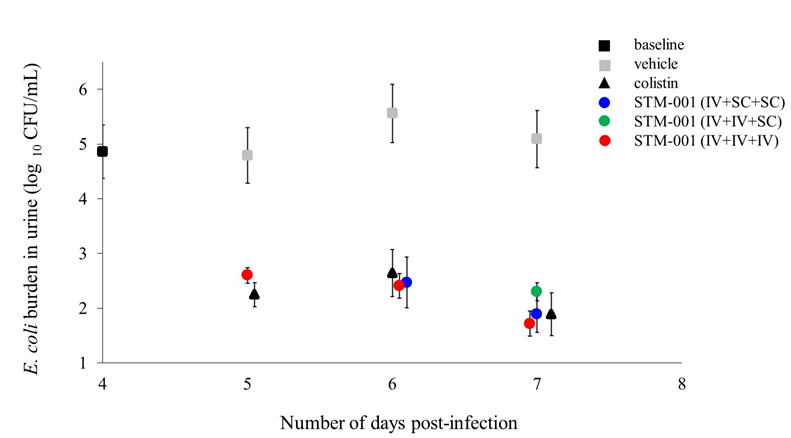
Figure 1: Therapeutic effects of IV or SC BID STM-001 (50 mg/kg) on urinary bacterial burden in a mouse model of cUTI administered during days 4-6 post-infection. Following the transurethral inoculation of 60 mice with NDM-1 E. coli, infection was allowed to proceed for 4 days. On day 4, 1 group of 10 mice (Group 1) were sacrificed to determine baseline urinary infection (and also tissues, see below). A further 10 mice were treated from days 4-6 with vehicle (Group 2) and 10 mice (Group 3) with SC colistin (20 mg/kg). The 30 remaining mice were the basis for three (3) different STM-001 treatment groups corresponding to treatment days 4-6 as follows: IV+SC+SC (Group 4); IV+IV+SC (Group 5); IV+IV+IV (Group 6). The entire experiment was terminated on day 7. Data for each experimental arm shows the mean (± SEM) log10 urinary bacterial burden (CFU/ml at days 4-7 post-infection). Significance was determined one-way ANOVA and Dunnett’s test by comparing all drug treatment groups to vehicle. (p < 0.05 for all treatment groups).
Basal bacterial counts in urine on day 4 were mean (± SEM) log10 4.86 ± 0.49 CFU/mL. Mean (± SEM) urinary bacterial counts (CFUs/ml) from vehicle-treated infected mice were similar on days 5 (log10 4.79 ± 0.51), 6 (log10 5.56 ± 0.53) and 7 (log10 5.09 ± 0.52). Burdens were significantly reduced in mice treated with IV STM-001 throughout to log10 1.71-2.47 CFU/mL (Group 6) as compared to the vehicle group (p < 0.05). In mice that received SC STM-001 during days 5 and 6 (Group 4), urinary burdens (CFUs/mL) on days 6 and 7 were log10 2.47 ± 0.47 and log10 1.89 ± 0.33, respectively. In Group 5, day 7 burden as a result of a switch to SC therapy on day 6 also remained significantly below the vehicle group at log10 2.3 ± 0.17 CFU/mL (p < 0.05).
For tissue bacterial burdens, irrespective of the mode of administration, STM-001 caused a significant mean log10 reduction in bacterial burdens from the baseline for all 4 organs (Figure 2) ranging from mean log10 1.4 CFU/tissue (Group 5, spleen; p < 0.05) to mean log10 2.65 (Group 4, kidney; p < 0.05). The impact of the comparator colistin was very similar to the effects of STM-001.
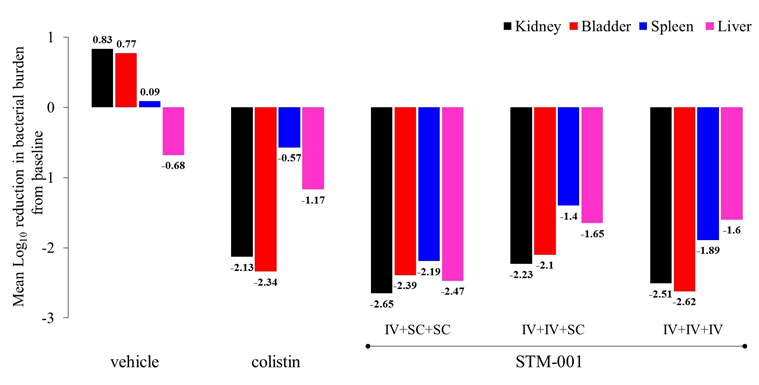
Figure 2: Effect of IV or SC STM-001 on mean log10 bacterial burden reduction from baseline in different tissues at day 7 post- infection in a mouse cUTI model. At 7 days post-infection, bacterial counts were enumerated in various organs from all 6 experimental groups (see methods) and deducted from 96 h baseline readings to determine load reduction.Significance was determined one-way ANOVA and Dunnett’s test by comparing bacterial burdens from all experimental groups to the baseline group (* p < 0.05). Baseline means (± SEM) log10 bacterial burdens (CFUs/tissue) were:kidney, 5.22 ± 0.31 CFU; bladder, 5.40 ± 0.24; liver, 4.61 ± 0.18; spleen, 3.60 ± 0.20. STM-001 groups were as follows: group 4 IV+SC+SC; group 5 IV+IV+SC; group 6 IV+IV+IV.
Discussion
The aim of this study was to determine if deployment of SC administration of STM-001 following an initial IV therapy, could continue to treat an established infection in a mouse model of cUTI driven by a carbapenem-resistant E. coli strain. To that end, we attempted to mimic in the model, a potential clinical scenario whereby specific cohorts of cUTI patients presenting at the ED might be eligible for an initial and brief IV STM-001 infusion. Thereafter, patients would be discharged for continued OSCAT either at home or different facilities (e.g. physicians’ office, skilled nursing facilities, infusion centers) for completion of a possible short treatment therapy [21].
From the data described, it is evident that SC administration of STM-001 clearly maintained the drug’s antibiotic effects since there was no recrudescence in urinary bacterial burdens towards the no treatment (vehicle) group during the experiment. Furthermore, at day 7 for STM-001 group 4 (IV+SC+SC), there was a trend for further reductions in bacterial burden which confirms the appropriate PK/PD exposure using the BID regimen. Importantly, for all STM- 001 groups, urinary bacterial burdens were ≤ 103 CFUs/ mL, which defines the microbiological cut-off point for clinical success [22]. In parallel with urinary burden data, STM-001’s effect to reduce tissue kidney bacterial burden is of clinical importance since the annual incidence of acute pyelonephritis associated with cUTIs is high with ~ 30% of 250,000 patients requiring eventual inpatient care [13, 14, 23]. In addition, reduction in bacterial load in bladder, liver and spleen with STM-001 could offer clinical utility for cUTI patients who develop urosepsis.
With a calculated number of 2,882,195 cUTI cases in the USA during 2017 [12], it is not surprising that associated healthcare costs exceeded $6 billion annually, primarily due to the in-patient care cohort [12, 13, 14]. A major reason for such costs is presumably attributable to the AMR profiles of the infecting E. coli and other Enterobacteriaceae strains [9, 10, 11]. Such phenotypes would be responsible for recurrent infections that necessitate readmissions as well as admissions from outpatient cohorts due to treatment failure. Therefore, to tackle AMR, there is a desperate need to develop improved antibiotics in conjunction with rapid, point-of- care diagnostics for use especially in the ED. Additionally, alignments in clinical guidelines should be implemented to more effectively treat a large number of young, adult cUTI patients with minimal comorbidities who present at the ED and are reliant upon inpatient IV therapy [25, 26]. Such a cohort might be an appropriate study group to assess the value of STM-001 in clinical trials whereby STM-001 could be given IV or SC at the ED with infected patients discharged the same day for continued OSCAT over 4-5 days. This approach could reduce hospitalization by as much as ~ 20% [25] with potential significant healthcare savings [26].
In a retrospective cohort study of cUTI outpatients (n=80,070) over a 12-month period investigating outcomes [14], ~50% patients received OPAT within a physicians' office or infusion suite. Although OPAT is increasingly being used as a cost-efficient approach to reduce length of stay and minimize hospitalization, average costs were high with treatment failures ranging from 23-34% for different cohorts. This confirms that OPAT is not a straightforward intervention and demands extensive clinical management and patient compliance. Indeed, OPAT-associated readmissions and admissions are often due to vascular access complications and adverse drug events [5]. In contrast, OSCAT [15, 16] offers a viable parenteral alternative to OPAT especially for antibiotics that are a) easily soluble; b) stable in solution; c) absorbed completely; d) possess favorable PK/PD (i.e. Cmax independent); e) eliminated in the urine; f) well tolerated. STM-001 clearly conforms to all these criteria [18, 19]. In addition, the remarkably low, putative humanized STM-001 dose of ~1-3 mg/kg with a potential for once-a-day dosing [19], further lends itself as highly feasible for OSCAT in the form of a pen injection or via an on-body delivery system [15, 16].
In summary, we have further confirmed the antibiotic effects of STM-001 to treat an established, carbapenem- resistant E. coli-driven cUTI and demonstrated its utility when given by SC administration. This finding supports the notion that STM-001 could be considered for OSCAT to treat cUTIs within various clinical cohorts and ultimately reduce healthcare burden. Importantly, this approach could offer significant clinical benefit for patients worldwide, especially those within low and lower middle income countries, in similar vein to recent efforts to ensure global accessibility to cefiderocol [27]. In an era of increasing incidences of MDR and pan-resistant resistant bacteria including NDM- containing E. coli isolates [28, 29], STM-001 offers a novel treatment approach to bolster the fragmented clinical pipeline of antibiotics [30] in a global pandemic that should no longer be referred to as “silent” [31]. Our current efforts are focused on guiding STM-001 through late-stage, preclinical development to fully scrutinize its safety profile including local tolerance prior to Phase 1 evaluation in healthy human volunteers. Ultimately, this approach might assist to avert the need for costly inpatient therapy and reduce the excessive healthcare burden costs associated with cUTIs.
Acknowledgements
We would like to thank Lynn Miesel, Pony Lee, Kun-Yuan Lin, Lucy Chia, Tim Yeh, Jui-Che Chien, Chin-Wei Chiang, Mei-Lee Hsieh, Candace Lee, Gin-Feng Lai, Timmy Huang, Yu-Chuan Chiu, Polly Li and Wei-Ting Liao (Pharmacology Discovery Services Taiwan, Ltd) for their outstanding and dedicated efforts in the conduct of the described studies. We are also extremely grateful to Noam B. Neville for expertise in the graphical and data analysis support. This work utilized NIAID’s suite of pre-clinical services for in-vivo assessment (Contract No. HHSN272201700020I). STM-001 and related molecular transporter technologies constitute part of a worldwide exclusive licensing agreement acquired by SuperTrans Medical from Stanford University, California, USA.
Transparency Declaration
LFN and JTR have none to declare. IS and PAW serve as consultants to SuperTrans Medical. The sponsor provided support and did not exercise control over the conduct or reporting of the research.
References
-
Antimicrobial Resistance Collaborators (2022) Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 399(10325): 629-655.
-
WHO (2019) New report calls for urgent action to avert antimicrobial resistance crisis. World Health Organization.
-
Tatsuta K (2013) Total synthesis of the big four antibiotics and related antibiotics. J Antibiot (Tokyo) 66(3): 107-129.
-
Yahav D, Shepshelovich D, Tau N (2021) Cost analysis of new antibiotics to treat multidrug-resistant bacterial infections: Mind the gap. Infect Dis Ther 10(1): 621-630.
-
Ng N, Bailey P, Pryor R, Fung L, Veals C, et al. (2021) Experiences in outpatient parenteral antimicrobial therapy (OPAT): Barriers and challenges from the front lines. Antimicrob Steward Healthc Epidemiol 1(1): e42.
-
CDC (2019) 2019 AR Threats Report. National Infection & Death Estimates, Centers for disease control and prevention.
-
Nicolle LE (2013) Urinary tract infection. Crit Care Clin 29(3): 699-715.
-
Wagenlehner FME, Johansen TEB, Cai T, Koves B, Kranz J, et al. (2020) Epidemiology, definition and treatment of complicated urinary tract infections. Nat Rev Urol 17(10): 586-600.
-
Zilberberg MD, Nathanson BH, Sulham K, Shorr AF (2020) Antimicrobial susceptibility and cross-resistance patterns among common urinary tract infections in U.S. hospitals, 2013-2018. Antimicrob Agents Chemother 64(8): e00346-e00420.
-
Bidell MR, Palchak M, Mohr J, Lodise TP (2016) Fluoroquinolone and third generation-cephalosporin resistance among hospitalized patients with urinary tract infections due to Escherichia coli: Do rates vary by hospital characteristics and geographic region? Antimicrob Agents Chemother 60(5): 3170-3173.
-
Critchley IA, Controneo N, Pucci MJ, Mendes R (2019) The burden of antimicrobial resistance among urinary tract isolates of _Escherichia coli_ in the United States in 2017. PLoS One 14(12): e0220265.
-
Carreno JJ, Tam IM, Meyers JL, Esterberg E, Candrilli SD, et al. (2020) Longitudinal, Nationwide, Cohort Study to assess incidence, outcomes, and costs associated with complicated urinary tract infection. Open Forum Infect Dis 7(1): ofz536.
-
Zilberberg MD, Nathanson BH, Sulham K, Shorr AF (2022) Descriptive epidemiology and outcomes of emergency department visits with complicated urinary tract infections in the United States, 2016-2018. J Am Coll Emerg Physicians Open 3(2): e12694.
-
Lodise TP, Manjelievskaia J, Marchlewicz, EH, Rodriguez M (2022) Retrospective cohort study of the 12 month epidemiology, treatment patterns, outcomes and health care costs among adult patients with complicated urinary tract infections. Open Forum Infect Dis 9(7): ofac307.
-
Jumpertz M, Guilhaumou R, Million M, Parola P, Lagier JC, et al. (2022) Subcutaneously administered antibiotics: a review. J Antimicrob Chemother 78(1): 1-7.
-
Ferry T, Lodise TP, Gallagher JC, Forestier E, Goutelle S, et al. (2020) Outpatient Subcutaneous Antimicrobial Therapy (OSCAT) as a measure to improve the quality and efficiency of healthcare delivery for patients with serious bacterial infections. Front Med (Lausanne) 7: 585658.
-
Antonopolis A, Zang X, Wegner T, Wender PA, Cegelski L (2019) Vancomycin-arginine conjugate inhibits growth of carbapenem-resistant _E. coli_ and targets cell-wall synthesis. ACS Chem Biol 14(9): 2065-2070.
-
Neville LF, Shalit I, Warn PA, Scheetz MH, Sun J, et al. (2021) _In-vivo_ targeting of _Escherichia coli_ with vancomycin-arginine. Antimicrob Agents Chemother 65(4): e02416-e02420.
-
Neville LF, Shalit I, Warn PA, Rendell JT (2022) Vancomycin-arginine (STM-001) abrogates ESBL carrier and carbapenem-resistant Escherichia coli burden in a murine complicated urinary tract infection model. J Antimicrob Chemother 77(6): 1706-1709.
-
CDC (2022) CDC & FDA Antimicrobial Resistance (AR) Isolate Bank. Centers for disease control and prevention.
-
Dickler NW, Spellberg B (2019) Short-course antibiotic therapy-replacing Constantine units with “shorter is better”. Clin Infect Dis 69(9): 1476-1479.
-
FDA (2018) Guidance Document: Complicated urinary tract infections: Developing drugs for treatment. U. S. Food & Drug Administration.
-
Brown P, Ki M, Foxman B (2005) Acute pyelonephritis among adults: cost of illness and considerations for the economic evaluation of therapy. Pharmacoeconomics 23(11): 1123-1142.
-
Dimitrijevic Z, Paunovic G, Tasic D, Mitic B, Basic D (2021) Risk factors for urosepsis in chronic disease patients with urinary tract infections. Sci Rep 11(1): 14414.
-
Lodise TP, Chopra T, Nathanson BH, Sulham K (2021) Hospital admission patterns of adult patients with complicated urinary tract infections who present to the hospital by disease acuity and comorbid conditions: how many admissions are potentially avoidable? Am J Infect Control 49(12): 1528-1534.
-
Zilberberg MD, Nathanson BH, Sulham K, Shorr AF (2022) Descriptive epidemiology and outcomes of hospitalizations with complicated urinary tract infections in the United States, 2018. Open Forum Infect Dis 9(1): ofab591.
-
Shionogi (2022) Antimicrobial resistance is an urgent and important public health threat.
-
Linkevicius M, Bonnin RA, Alm E, Svartstrom O, Apfalter P, et al. (2023) Rapid cross-border emergence of NDM- 5 producing _Escherichia coli_ in the European Union/ European Economic Area, 2012 to June 2022. Euro Surveill 28(19): 2300209.
-
Simner PJ, Bergman Y, Conzemius R, Jacobs E, Tekle T, et al. (2023) An NDM producing _Escherichia coli_ clinical isolate exhibiting resistance to cefiderocol and the combination of ceftazidime-avibactam and aztreonam: Another step towards pan-**β-** lactam resistance. Open Forum Infect Dis, pp: ofad276.
-
Prasad NK, Seiple IB, Cirz RT, Rosenberg OS (2022) Leaks in the pipeline: a failure analysis of Gram-negative antibiotic development from 2010-2020. Antimicrob Agents Chemother 66(5): e0005422.
-
Mendelson M, Sharland M, Mpundu M (2022) Antibiotic resistance: calling time on the “silent pandemic”. JAC Antimicrob Resist 4(2): dlac016.
- Antifungal Activity of New Acetophenone Derivatives
- Interconnected Microbiomes Human Health Within an Environmental Framework
- Silkworm-Based Vaccine Production for H5N1: A One Health Approach to Pandemic Preparedness
- Microbial Diversity and Lipolytic Activity of Bacteria and Fungi from Oil-Contaminated Sites in Makurdi Metroplois
- Antibiotic Resistance Profile of Bacteria Isolated at the Central Laboratory of the National Hospital Center of Nouakchott
- Epidemiology and Sensitivity to Antibiotics of Germs Isolated from Blood Cultures in the Laboratory of the National Hospital Center of Nouakchott-Mauritania