Demographical Investigations of Iraqi Patients with Nasopharyngeal and Sinonasal Neoplasms
Introduction: Age is important risk factor for nasopharyngeal and sinonasal cancers, but data regarding whether patient age at diagnosis is related to such malignancies survival are conflicting. This population-based study tried to evaluate the impact of some demographical characteristics of patients with nasopharyngeal and sinonasal tumors for updating the recent insights of these challenging tumors in our country, on the hope that it may serve in speculation of the related outcomes. This study included 183 formalin-fixed, paraffin-embedded tissue blocks from 35 inflammatory nasal polyps (INP), 35 sinonasal papillomae (SNP), 65 nasopharyngeal carcinomas (NPC), 18 sinonasal carcinomas (SNC) as well as 30 healthy nasal tissues as a control for this study. Results: It was observed from the data in this research that the age group of those patients mostly affected with NPC is the age stratum of 41-60 years (46.2%:30), while the more influenced age of SNC was 41-60 and 61-80 years (50%:9). Regarding gender distribution of the patients with NPC and SNC lesions, the percentage of the males with NPC was higher (73.8%: 48) than of their female counterparts (26.2%: 17). Whereas, the level of males with sinonasal cancers was lower (38.9%: 7) than the level of their female counterparts (61.1%: 11). Anatomically, NPC cases, 19(29.2%) cases were as nasal masses and 46 (70.8%) were as post nasal masses. On the other hand, SNC was 16 (88.9%) as nasal masses and only 2 (11.1%) were as para nasal masses. In regard to histopathological features of carcinoma tissues, the undifferentiated carcinoma was the most frequent type in nasopharyngeal carcinoma in this study, constituting (75.4%), while the moderately differentiated carcinoma was the most frequent type in sinonasal cancer tissues group founding (44.4%) of the cases. Conclusions: We found age and gender-specific inequalities in time to diagnosis for some, but not all cancer sites studied. While these need further explanation, these findings can inform the development and evaluation of interventions intended to achieve a timely diagnosis and improved cancer outcomes, such as to provide equity across all age and gender groupings.
Introduction
Nasopharyngeal cancer is a type of head and neck cancer; it starts in the upper part of your throat, behind the nose [1]. Sinonasal malignant neoplasms are rare tumors that constitute about 3% of tumors in the upper respiratory tract; these include malignancies of the nasal cavity and paranasal sinuses (maxillary sinus, ethmoid sinuses, frontal sinus, and sphenoid sinus) [2]. The age was recognized as a risk factor for sinonasal malignant tumorigenesis, in which older age was associated with higher incidence. However, the frequency was also influenced by the duration of carcinogenic exposure [3].
In high-risk populations, NPC incidence rises after the age of 30 years with peaks at 40-60 years and after that declines [4, 5]. Sinonasal papillomas (SNP) and inflammatory nasal polyps (INP) are the benign tumors of the nasal cavity that result from chronic inflammation, allergens, pollutants, infectious agents, and cystic fibrosis [6, 7]. In nasal cavity, paranasal sinuses and nasopharynx, a variety of neoplastic and non-neoplastic lesions, are commonly encountered [8, 9] where polypoid masses are the most common form of these lesions; these polyps can be either benign or malignant [10] and nasal inflammatory polyps are the most common lesions affecting nearly 4% of the general population [11], and malignant tumors being rare (less than 1% of all carcinomas) [12].
On the other hand, sinonasal undifferentiated carcinoma of the paranasal sinus is extremely rare, accounting for <3% of all head and neck tumors and 0.2–0.8% of all cancers and is known to arise from Schneiderian epithelium which lines the nasal cavity and the paranasal sinus [13]. However, Shirazi, et al. [6] in reported that tumors of the nasal cavity are often grouped with those in the paranasal sinuses in the sinonasal region [6]. Malignant neoplasms are extending from the mucosal membrane of the nasal cavities, paranasal sinuses, and nasopharynx and are classified into three major histologic subtypes: keratinizing, non-keratinizing and undifferentiated squamous cell carcinoma [14].
The Studied Groups and Sample Collection
A total number of one hundred eighty-three (183) randomly selected nasopharyngeal, and sinonasal tissues were enrolled in the present study which was collected from patients admitted to surgical wards and from patients subjected to biopsies and archived at histopathological laboratories in several hospitals at Baghdad (Al-kindy Teaching Hospital, Al-Yarmouk Teaching Hospital, and Ghazi Al-Hariri Teaching Hospital / Baghdad Medical City); the collected samples were divided into following study groups:
1. Eighty-three malignant tissue blocks (65 nasopharyngeal carcinomas and 18 sinonasal carcinomas) have been obtained from patients who had undergone surgical operations or biopsies.
2. Seventy benign sinonasal tissue blocks have been obtained from patients who had undergone surgical operations or biopsies for different benign masses which are classified into two groups:
a. Thirty-five sinonasal papillomas.
b. Thirty-five inflammatory nasal polyps.
3. Thirty sinonasal healthy tissue biopsies (sinonasal tissues without remarkable pathological changes) from patients subjected to nasal bridge re-construction operation were used as a control group.
These tissues were re-examined for final confirmation of their initial diagnosis as nasopharyngeal and sinonasal carcinoma tissues, sinonasal benign tumors (sinonasal papilloma and polyps) and healthy tissues.
Statistical Analysis
IBM SPSS statistics program Version 21 was used to do the statistical analysis of the current study & Microsoft Excel 2010 for graphics presentation.
The usual statistical methods were used to assess and analyze the results; they include:
Descriptive Statistics
1. Statistical tables including observed frequencies, percentages, mean standard deviation, standard error & range (Minimum & Maximum).
2. Graphical presentation through using Bar- charts.
Inferential Statistics
They were used to accept or reject the statistical hypotheses; they include: 1. Chi-Square test (χ2)
2. Binomial test (Z- test).
3. The (ANOVA) test with multi comparison, less significant difference (LSD) test.
Results
Clinic Pathological Findings
Distribution of patients with sinonasal and nasopharyngeal lesions in relation to their age: The archival specimens collected in this study were related to nasopharyngeal cancer patients whose ages ranged from
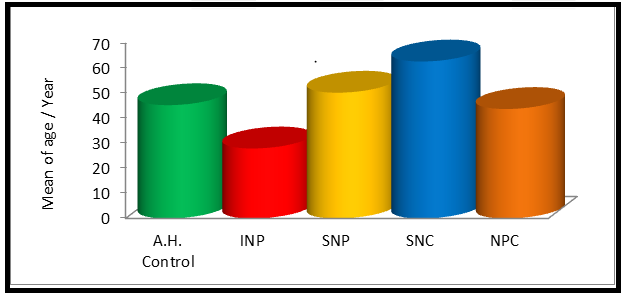
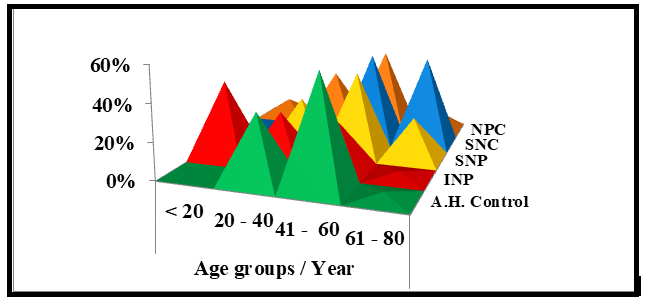
13 -73 years, and the mean age of those patients was (43.71 ± 15.67) years. Whereas the sinonasal cancer patients’ age was ranging from 42 to 82 with a mean of (62.67 ± 9.10) years. The mean age of patients with sinonasal papilloma was (50.21 ±15.12) years, while their age ranged from 3- 71 years. However, the mean age of patients with inflammatory nasal polyps was (27.94 ± 16.57) years, and their age ranged from 6 – 64 years. Furthermore, the mean age of apparently healthy individuals was (45.23 ± 7.88) years, and their age ranged from 30- 62 years and as shown in table 1 and figure 1. Also, it was observed in (Table 2 & Figure 2) that age group of those patients mostly affected with nasopharyngeal cancers is the age stratum of 41-60 years (46.2%:30), followed by the age stratum of 20-40 years (30.8%:20), then the age stratum of 61-80 years (12.3%:8) and lowest affected group of nasopharyngeal cancers was the age stratum of < 20 years with the percentage (10.8%: 7). Furthermore, the more influenced age of sinonasal carcinoma patients was 41-60 and 61-80 years (50%:9), while no patients with sinonasal carcinoma were found in < 20 and 20-40 years.
Regarding those patients who were suffering from sinonasal papillomas, the most affected age group was 41- 60 years (45.7%:16), followed by 20-40 years (28.6%:10), then 61-80 years (22.9%: 8) and lastly the lowest affected group of sinonasal papillomas was those in the age stratum < 20 years (2.9%:1). Regarding inflammatory nasal polyps patients, the most affected age group was those < 20 years (42.8%:15), followed by those aged 20-40 years (28.6%: 10), then age group of 41-60 years (25.7%:9) and finally the age group of 61-80 years (2.9%:1). The statistical analysis shows highly-significant differences (P<0.01) among the distribution of age strata studied herein.
| Studied groups | N | Mean Age / Years | Std. Deviation | Std. Error | Range* | |
|---|---|---|---|---|---|---|
| Mini. | Maxi. | |||||
| Apparently healthy Control | 30 | 45.23 | 7.88 | 1.44 | 30 | 62 |
| Inflammatory nasal polyp(INP) | 35 | 27.94 | 16.57 | 2.8 | 6 | 64 |
| Sinonasal papilloma (SNP) | 35 | 50.21 | 15.12 | 2.49 | 3 | 71 |
| Sinonasal carcinoma (SNC) | 18 | 62.67 | 9.1 | 2.14 | 42 | 80 |
| Nasopharyngeal carcinoma (NPC) | 65 | 43.71 | 15.67 | 1.94 | 2 | 73 |
| Total | 183 |
Table 1: Distribution of groups in relation to the mean and range of their age. * Mini: minimum, Maxi: maximum
| Age groups/ Year A.H. Control | Studied groups | Pearson Chi- Square(P-value) | |||||
|---|---|---|---|---|---|---|---|
| Inflammatory nasal polyp (INP) | Sinonasal Papilloma (SNP) | Sinonasal carcinoma (SNC) | Nasopharyngeal carcinoma (NPC) | ||||
| < 20 | N | 0 | 15 | 1 | 0 | 7 | P=0.00 Highly Sign. (P<0.01) |
| % | 0% | 42.80% | 2.90% | 0% | 10.80% | ||
| 20 - 40 | N | 11 | 10 | 10 | 0 | 20 | |
| % | 36.70% | 28.60% | 28.60% | 0% | 30.80% | ||
| 41 - 60 | N | 18 | 9 | 16 | 9 | 30 | |
| % | 60% | 25.70% | 45.70% | 50% | 46.20% | ||
| 61 - 80 | N | 1 | 1 | 8 | 9 | 8 | |
| % | 3.30% | 2.90% | 22.90% | 50% | 12.30% | ||
| Total | N | 30 | 35 | 35 | 18 | 65 | |
| % | 100% | 100% | 100% | 100% | 100% |
Table 2: Age stratification of patients about to their histopathological diagnosis.
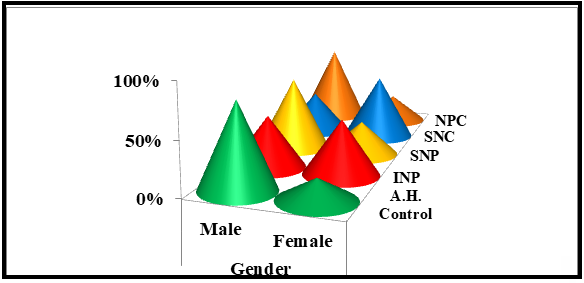
Gender distribution of the patients with sinonasal and nasopharyngeal lesions In this study, and as shown in table 3 and figure 3, the level of the males with nasopharyngeal cancers was higher (73.8%: 48) than the level of their female counterparts (26.2%: 17). Whereas, the level of males with sinonasal cancers was lower (38.9%: 7) than the level of their female counterparts (61.1%: 11).
| Gender A.H. Control | Studied groups | Pearson Chi-Square (P-value) | |||||
|---|---|---|---|---|---|---|---|
| Inflammatory nasal polyp (INP) | Sinonasal papilloma (SNP) | Sinonasal carcinoma (SNC) | Nasopharyngeal carcinoma (NPC) | ||||
| Male | N | 24 | 17 | 24 | 7 | 48 | P=0.005 Highly Sign. (P<0.01) |
| % | 80% | 48.60% | 68.60% | 38.90% | 73.80% | ||
| Female | N | 6 | 18 | 11 | 11 | 17 | |
| % | 20% | 51.40% | 31.40% | 61.10% | 26.20% | ||
| Total | N | 30 | 35 | 35 | 18 | 65 | |
| % | 100% | 100% | 100% | 100% | 100% | ||
| Male / Female Ratio | 4 | 0.94 | 2.18 | 0.64 | 2.82 |
Table 3: Distribution of study groups about their gender.
Regarding the patients who suffer from sinonasal papillomas, the level of males was also higher (68.6%: 24) than the level of female (31.4%:11) while the level of males with inflammatory nasal polyps (48.6%:17) was lower than the level of females (51.4%:18). The male /female ratio of the patients with nasopharyngeal cancers was 2.8:
1. Furthermore, male / female ratio of the sinonasal cancer patients was 0.6: 1, and the male/ female ratio of sinonasal benign tumors (papilloma and polyps) was 2.2: 1 and 0.9: 1, respectively. The statistical analysis showed a high- significant difference (P<0.01) among the studied groups.
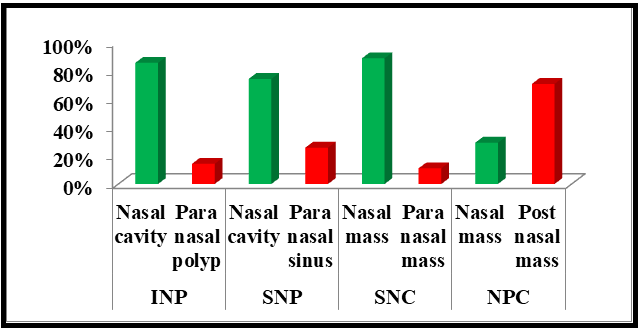
Anatomical distribution of benign and malignant cases: Anatomically, inflammatory polyps 30 (85.7%) cases were diagnosed in the nasal cavity while only 5(14.3%) as paranasal polyps and sinonasal papillomas 26 (74.3%) cases were diagnosed in the nasal cavity while only 9 (25.7%) at paranasal sinuses. Regarding malignant group (NPC), 19(29.2%) cases were as nasal masses, and 46 (70.8%) were as post nasal masses. On the other hand, sinonasal cancers were 16 (88.9%) as nasal masses and only 2 (11.1%) were as Para nasal masses.
The results revealed highly significant differences at (P<0.01) inflammatory polyp and among sinonasal papilloma groups. Likewise, highly significant differences were found at (P<0.01) between sinonasal and nasopharyngeal carcinoma groups (Table 4 and Figure 4).
| Specimen Sites | N | % | Binomial Z-test (P-value) | |
|---|---|---|---|---|
| Inflammatory Sino-nasal polyp (INP) | Nasal cavity | 30 | 85.70% | P=0.00 Highly Sign. (P<0.01) |
| Inflammatory Sino-nasal polyp (INP) | paranasal polyp | 5 | 14.30% | P=0.00 Highly Sign. (P<0.01) |
| Inflammatory Sino-nasal polyp (INP) | Total | 35 | 100% | P=0.00 Highly Sign. (P<0.01) |
| Sino-nasal papilloma (SNP) | Nasal cavity | 26 | 74.30% | P=0.006 Highly Sign. (P<0.01) |
| Sino-nasal papilloma (SNP) | paranasal sinus | 9 | 25.70% | P=0.006 Highly Sign. (P<0.01) |
| Sino-nasal papilloma (SNP) | Total | 35 | 100% | P=0.006 Highly Sign. (P<0.01) |
| Sinonasal carcinoma (SNC) | Nasal mass | 16 | 88.90% | P=0.001 Highly Sign. (P<0.01) |
| Sinonasal carcinoma (SNC) | Para nasal mass | 2 | 11.10% | P=0.001 Highly Sign. (P<0.01) |
| Sinonasal carcinoma (SNC) | Total | 18 | 100% | P=0.001 Highly Sign. (P<0.01) |
| Nasopharyngeal carcinoma (NPC) | Nasal mass | 19 | 29.20% | P=0.001 Highly Sign. (P<0.01) |
| Nasopharyngeal carcinoma (NPC) | Post nasal mass | 46 | 70.80% | P=0.001 Highly Sign. (P<0.01) |
| Nasopharyngeal carcinoma (NPC) | Total | 65 | 100% | P=0.001 Highly Sign. (P<0.01) |
Table 4: Anatomical distribution of the studied benign and malignant lesions.
Histopathological Features of Carcinoma Tissues
Grading of carcinomas: The carcinoma group grading in the present study revealed that well differentiated (keratinizing) carcinomas constituted 10(15.4%) tissues of NPC group, while 2(3.1%) tissues of NPC have moderately differentiated grade. The poorly differentiated grade was observed in 4(6.2%) cases while undifferentiated carcinomas grade noticed in 49(75.4%) (Table 5 & Figure 5).
Well, differentiated (keratinizing) carcinomas were
not seen in any tissues in SNC group, while 8(44.4%) SNC tissues have moderately differentiated grade, 7(38.9%) tissues have poorly differentiated grade and undifferentiated carcinomas grade were observed in 3(16.7%) (Table 5 & Figure 5). The statistical analysis of the grading distribution of nasopharyngeal and sinonasal carcinomas revealed highly significant differences (P<0.01). The undifferentiated carcinoma was the most frequent type in nasopharyngeal carcinoma in this study founding (75.4%) of the tissues, while the moderately differentiated carcinoma was the most frequent type in sinonasal cancer tissues group constituting (44.4%) of the cases.
| Diagnosis (Dx.) Sinonasal Carcinoma (SNC) | Studied groups | Pearson Chi-Square (P-value) | ||
|---|---|---|---|---|
| Nasopharyngeal carcinoma (NPC) | ||||
| Well differentiated | N | 0 | 10 | P=0.00 Highly Sign. (P<0.01) |
| % | 0% | 15.40% | ||
| Moderately differentiated | N | 8 | 2 | |
| % | 44.40% | 3.10% | ||
| Poorly differentiated | N | 7 | 4 | |
| % | 38.90% | 6.20% | ||
| Undifferentiated | N | 3 | 49 | |
| % | 16.70% | 75.40% | ||
| Total | N | 18 | 65 | |
| % | 100% | 100% |
Table 5: Distribution of Carcinoma Group According to their Grading.
Discussion
The patient’s age in the present results coincide with the results of many other studies: [11, 15] found that the mean age of Nigerian patients with head and neck cancers, including nasopharyngeal cancers, was 43.3 years. Also, several studies are in agreement with the current results, which have stated that nasopharyngeal cancers increased with the advancing age with a peak age of 41-60 years and decreased above 60 years [16, 17]. However, the results of the present study are consistent with the results of other studies that revealed a mean age of patients with SNC was 62.3 years with age ranging from 8 to 82 years, where the most common age stratum found was 71–80 years [9, 18]. Another study by d’Errico, et al. reported that 60 – 69 years old as the highest age group of patients [3].
The age was recognized as a significant factor for sinonasal malignant tumorigenesis, in which older age was associated with a higher incidence. However, the frequency was also influenced by the duration of carcinogenic exposure [3].
Regarding the benign sinonasal lesions, the current study agrees with study conducted of Dewan, et al. [19] who revealed that among sinonasal neoplasms (including sinonasal papilloma) the most common age stratum was 41- 50 years and also agreed with study conducted by Singh, in (2016) who found among the benign neoplasms of nasal and paranasal cavity, sinonasal papilloma was common in the age stratum of 11-30 years and 41-60 years [18, 19]. Another similar study by Gupta S, et al. [20] has indicated that sinonasal papilloma was common in the 5th and 6th decades of age with a mean age of 52 years, and an age ranged from 10-74 years. Also Bhattacharya, et al. and Sivalingam et al. found in their studies that all the benign cases were seen to have an age of <40 years with a mean age of 20 years [16, 17].
However, the present observed results, as well as the reported similarities and differences of the results among these mentioned studies regarding the age distribution of patients with different sinonasal and nasopharyngeal lesions have supported the theory of an association of sinonasal and nasopharyngeal carcinomas to the age. This could be explained by the presence of immune system defect in those older ages. This might lead to the accumulation of DNA mutations in the cells, and then being an additional significant risk factor in cancer development [21]. Also, genetic susceptibility has been reported as an etiological co-factor responsible for the risk of developing NPC, which has a relation to differences in ethnicity and geographical areas with various levels of risk. Undoubtedly HLA is playing important role in NPC predisposition by playing a functional role in modulating an innate and adaptive immune response [22]. Also, it has been reported that specific HLA alleles (including HLA-A2, HLA-B17, and HLA-Bw46) about to the prevalence of NPC especially in the Chinese population, although reasons for these associations or differences are still elusive [23].
Also, present percentage of NPC which was increased with the patients age could be related by many risk factors that enhance appearance of malignant nasopharyngeal tumor in young age group about the proceeding of age such as genetic predisposition, smoking and changes in life style (a highly caloric diet-rich in fat, refined carbohydrate, alcohol uptake) which in turn supporting a previous study done by Abdulamir AS, et al. [24]. It was observed in most of the studies that mean age was least for non-neoplastic lesions, starting to increase for benign lesions and was at highest for malignant lesions [25].
Regarding of gender, in nasopharyngeal carcinoma and sinonasal papilloma, the results of the current study are consistent with the results of most of the other studies [9, 26, 27] who found that the affected men were more than predominance their counterpart women. This prevalence a male in NPC may be belongs essentially to the nature of the risk factors [28]. In our study, the male to female ratio was 1:1.6 for SNC patients. This result is consistent with Shirazi, et al. [6], who found the results of sinonasal undifferentiated carcinoma (SNUC) regarding male to female ratio was 1:2 [6]. This may be attributed to various genetic, hormonal, menstrual, an immune system in female and environmental factors since women have been more exposing themselves to known carcinogens, such as cigarette smoking and alcohol consumption. Moreover, stress and an increasing number of females working in factories, exposing themselves to carcinogens can be considered as other factors [29].
Regarding nasal polyps, the results of the current study agree with the study of Mumbuc, et al. who found a slight female preponderance in the nasal polyp group [30]. Also, this study agrees with a study conducted by Bakari, et al. [31] in which found a higher preponderance of females than males as well as agrees with the study conducted by Parajuli, et al. [32] in which found a slight female preponderance with a male: female ratio of 1:1.31 [31, 32]. Overall, the variance in incidence rate between the two sexes are not understood, but could likely involve the interactions between gender-related differences in exposure to hormones and risk factors [5, 31].
In relation with the anatomical distribution of benign and malignant cases, The results of this study in accordance with other studies by [11, 33, 34] who found that the nasal cavity is the most common site for the non–neoplastic and neoplastic tumors followed by paranasal sinuses. Also, the present results are consistent with previous studies by Khan, et al. who found that nasopharynx and paranasal sinus are the most common sites for malignant tumors [35]. Several researchers reported that the most common location of tumors is the nasal cavity (57%), followed by the maxillary sinus (27 %). Moya-Plana, et al. found that squamous cell carcinoma is the most recurrent form of sinonasal malignancy, especially in the maxillary sinuses and nasal cavity [26]. In the nasal cavity, paranasal sinuses and nasopharynx, a variety of neoplastic and non-neoplastic lesions, are commonly encountered [8, 9] where polypoid masses are the most common form of these lesions [10]. However, Shirazi, et al. reported that tumors of the nasal cavity are often grouped with those in the paranasal sinuses in the sinonasal region [6].
The histological grading of cancer is important parameter of risk assessment in nasopharyngeal patients and reflected that in the histological subtype of this type of cancer [36]. Malignant neoplasms are extending from the mucosal membrane of the nasal cavities, paranasal sinuses, and nasopharynx, and are classified into three major histologic subtypes: keratinizing, non-keratinizing and undifferentiated squamous cell carcinoma [14, 37]. The grading of the carcinoma group in the present study revealed that well differentiated (keratinizing) carcinomas are constituting 10 (15.4%) tissues of NPC group, while 2(3.1%) tissues of NPC have moderately differentiated grade. The poorly differentiated grade was observed in 4(6.2%) tissues, while undifferentiated carcinomas grade was noticed in 49(75.4%) (Table 5 & Figure 5). Well differentiated (keratinizing) carcinomas were not seen in any tissues in SNC group, while 8(44.4%) SNC tissues have moderately differentiated grade, 7(38.9%) tissues have poorly differentiated grade and undifferentiated carcinomas grade were noticed in 3(16.7%) (Table 5 & Figure 5). The statistical analysis of the grading distribution of nasopharyngeal and sinonasal carcinomas revealed highly significant differences (P<0.01).
The undifferentiated carcinoma was the most frequent type in SNC in this study founding (75.4%) of the tissues, while the moderate differentiated carcinoma was the most frequent type in sinonasal cancer tissues group constituting (44.4%) of the cases. The increase rate of undifferentiated NPC and moderately SNC carcinomas may be due to the patients were not aware of their health and did not follow up with their condition as early as possible.
In this respect, Shirazi, et al. revealed that NPC was the most common malignant tumor. Out of the (40.6%) tissues diagnosed as NPC (71.2%) were squamous cell carcinomas (WHO Grade I), (17.3%) were non-keratinizing squamous carcinomas (WHO grade II), and (11.5%) were lymphoepithelioma type carcinomas (WHO grade III). 29.8 [6].
Also, Al-Shemmary found that 37.5% of nasopharyngeal tissues have grade I (squamous cell grade), 15% have grade II (non-keratinizing), and 47.5% have grade III (undifferentiated grade) [38]. However, López-Hernández, et al. found (31.2%) undifferentiated, (57%) with well and moderately differentiated, and (29.8%) associated with poorly differentiated sinonasal carcinomas patients [39]. The present results are incompatible in percentages with Agaoglu, et al. study of NPC tissues where 9.9% was in grade I, followed by 3.7% in grade II, and 86.4% in grade III [40].
Adam, et al. shows that the WHO type III was the most frequent histopathological type in their study population. These results are corresponding with the current study where the WHO type III was the most frequent histopathological type of NPC grades [41]. In contrast to our study, Agaimy results have shown a significant proportion of sinonasal neoplasms displaying undifferentiated carcinoma [42].
However, type III NPC comprises over 95% of NPC in high-incidence areas, and most of the remaining 5% is type II NPC. On the other hand, the most predominant NPC type in low-incidence regions was type I and may have an etiology different from other two histologic types [43, 44]. In areas with low incidence of NPC (such as North America), around 25% of NPC patients are WHO type І, 12% are type П, and 63% are type Ш whereas, in endemic areas such as South China, the histological distribution is approximately 2%, 3%, and 95%, respectively [45].
In endemic areas of NPC, 95% are type III undifferentiated carcinoma, which has Epstein–Barr virus (EBV) infections as the prevalent etiological factor interacting with genetic predisposition as well as consumption of preserved foods [46]. Furthermore, there is a very strong association between nasopharyngeal undifferentiated carcinoma and EBV [47]. Nasopharyngeal carcinoma showed a high incidence rate (0.35) while; accessory sinus was a low incidence in ratio (0.05), according to Iraqi Cancer Registry [48]. The USA, non-keratinizing vs. keratinizing subtypes have significantly shown race-related factors (Asians vs. Hispanic and white vs. black), respectively [49].
References
-
Wu L, Li C, Pan L (2018) Nasopharyngeal carcinoma: A review of current updates. Experimental and therapeutic medicine 15(4): 3687-3692.
-
Dean KE, Shatzkes D, Phillips CD (2019) Imaging Review of new and emerging sinonasal tumors and tumor-like entities from the Fourth Edition of the World Health Organization Classification of Head and Neck Tumors. AJNR Am J Neuroradiol 40(4): 584-590.
-
d’Errico A, Pasian S, Baratti A, Zanelli R, Alfonzo S, et al. (2009) A case-control study on occupational risk factors for sino-nasal cancer. Occup Environ Med 66(7): 448-
-
Chan F, Bray P, McCarron W, Foo A, Lee T, et al. (2005) WHO classification of tumors. Pathology and genetics of Head and Neck tumors. International Agency for Research on Cancer press, Lyon, Chapter 2, pp: 85-113.
-
Lee JW, Hsiao WT, Lee KF, Sheu LF, Hsu HY, et al. (2010) Widespread expression of prostate apoptosis response‐4 in nasopharyngeal carcinoma. Head & neck 32(7): 877- 885.
-
Shirazi N, Bist SS, Selvi TN, Harsh M (2015) Spectrum of sinonasal tumors: a 10-year experience at a tertiary care hospital in North India. Oman medical journal 30(6): 435-440.
-
Stevens WW, Schleimer RP, Kern RC (2016) Chronic Rhinosinusitis with Nasal Polyps. J Allergy Clin Immunol Pract 4(4): 565-572.
-
Sutar HB (2015) Clinic pathological study of nasal polypoidal masses. Annual International Medical Dental Research 1(3): 315-319.
-
Arti K, Kishore K, Manhas P (2018) Neoplastic masses of nasal cavity, paranasal sinuses, and nasopharynx: A clinicopathological study. Asian Pacific Journal of Health Sciences 5(1): 9-12.
-
Kalra VK, Yadav SPS, Vashishth S (2018) Polypoid masses in the nasal cavity. International Journal of Healthcare and Biomedical Research 6(2): 144-148.
-
Parmar NJ, Jethwani DP, Dhruva GA (2018) Histopathological study of nasal lesions: 2 years study. International Journal of Research in Medical Sciences 6(4): 1217-1223.
-
Shah R, Islam MS, Islam MR, Arfin A (2014) Importance of histopathology in diagnosis of unilateral nasal polyps. Clinical Medicine Research 3(4): 87-89.
-
Purkayastha A, Sharma N, Pandya T, Arora C (2016) An extremely rare case report of sinonasal undifferentiated carcinoma of paranasal sinuses. Archives of Medicine and Health Sciences 4(2): 225-265.
-
Franchi A (2017) Sinonasal tumor pathology: what’s new?. Pathologica 109(1): 9-13.
-
Oga EA, Schumaker LM, Alabi BS, Obaseki D, Umana A, et al. (2016) Paucity of HPV-related head and neck cancers (HNC) in Nigeria. PloS One 11(4): e0152828.
-
Bhattacharya J, Goswami BK, Banerjee A, Bhattacharyya R, Chakrabarti I, et al. (2015) A clinic pathological study of masses arising from sinonasal tract and nasopharynx in north Bengal population with special reference to neoplasms. The Egyptian Journal of Otolaryngology 31(2): 98-109.
-
Sivalingam J, Sarawagi R, Raghuwanshi S, Yadav PK (2015) Sinonasal neoplasia–clinicopathological profile and importance of computed tomography. Journal of clinical and diagnostic research 9(6): 1-14.
-
Singh N, Rajesh SL (2016) Histopathological patterns of masses in the nasal cavity, paranasal sinuses and nasopharynx. Journal of Evidence Based Medicine and Healthcare 3(2): 99-101.
-
Dewan K, Ray R, Nag D, Mallick MG, Mukhopadhyay S (2013) Clinic pathological evaluation of sinunasal neoplasm in a tertiary care hospital. IOSR Journal of Dental and Medical Sciences 6(2): 20-26.
-
Gupta S, Singh S, Garewal J, Vijay S, Makhija A, et al. (2016) A clinicomorphological study of Schneiderian Papilloma. Indian Journal of Pathology and Oncology 3(2): 347-350.
-
Burns EA, Leventhal EA (2000) Aging, Immunity, and Cancer. Cancer Control l (7): 513-522.
-
Tang M, Lautenberger JA, Gao X, Sezgin E, Hendrickson SL, et al. (2012) The principal genetic determinants for nasopharyngeal carcinoma in China involve the HLA class I antigen recognition groove. PLoS Genet 8(11): e1003103.
-
Thompson LD (2006) Sinonasal Carcinomas. Current Diagnostic Pathology 12(1): 40-53.
-
Abdulamir AS, Hafidh RR, Abdulmuhaimen N, Abubakar F, Abbas KA (2008) The distinctive profile of risk factors of nasopharyngeal carcinoma in comparison with other head and neck cancer types. BioMed Central public health 5: 8.
-
Bist SS, Varshney S, Baunthiyal V, Bhagat S, Kusum A (2012) Clinico-pathological profile of sinonasal masses: An experience in tertiary care hospital of Uttarakhand. Natl J Maxillofac Surg 3(2): 180-186.
-
Moya-Plana A, Bresson D, Temam S, Kolb F, Janot F, et al. (2016) Development of minimally invasive surgery for sinonasal malignancy. European annals of otorhinolaryngology, head and neck diseases 133(6): 405-411.
-
Pastor M, Pousa AL, Del Barco E, Segura PP, Astorga BG, et al. (2018) SEOM clinical guideline in nasopharynx cancer(2007). Clin Transl Oncol 20(1): 84-88.
-
Charafeddine MA, Olson SH, Mukherji D, Temraz SN, Abou-Alfa GK, et al. (2017) Proportion of cancer in a Middle eastern country attributable to established risk factors. Biomedical Central cancer 17(1): 337-341.
-
Ali SHM, Al Jewari MMM, Saaed NAHAA (2013) Localization of Human Cytomegalovirus-Late Gene DNA, Expression of P53 Gene and CD8-Tumor Infiltrating Lymphocytes in Oral Squamous Cell Carcinoma. Iraqi Academic Scientific Journal 12(2): 296-305.
-
Mumbuc S, Karakok M, Baglam T, Karatas E, Durucu C, et al. (2007) Immunohistochemical analysis of PCNA, Ki67 and p53 in nasal polyposis and sinonasal inverted papillomas. J Int Med Res 35(2): 237-241.
-
Bakari A, Afolabi OA, Adoga AA, Kodiya AM, Ahmad BM (2010) Clinico-pathological profile of sinonasal masses: an experience in national ear care center Kaduna, Nigeria. BMC Res Notes 3(1): 186-191.
-
Parajuli S, Tuladhar A (2013) Histomorphological spectrum of masses of the nasal cavity, paranasal sinuses and nasopharynx. Journal of Pathology of Nepal 3(5): 351-355.
-
Al Doory IAH (2017) Detection of Human Papilloma Viruses and Co-Expression of Tumor Suppressor Genes in Sinonasal and Nasopharyngeal Neoplasms. (Doctoral dissertation, University of Baghdad).
-
Lahma J, Hejjouji R, Gicquel P, Essakalli L (2018) Large cell neuroendocrine carcinoma of the nasal cavity: an extremely rare and new distinct entity. The Pan African medical journal 30 (188): 14992-14997.
-
Khan N, Zafar U, Afroz N, Ahmad SS, Hasan SA (2006) Masses of nasal cavity, paranasal sinuses and nasopharynx: a clinic pathological study. Indian J Otolaryngol Head Neck Surg 58(3) 259-263.
-
Robinson S, Tan LW, James C, Karakousis A, Wormald PJ (2006) Do nasal polyps and inverted papilloma have similar disorders in cell cycle regulation?. Am J Rhinol 20(6): 637-640.
-
Patel VJ, Chen NW, Resto VA (2017) Racial and ethnic disparities in nasopharyngeal cancer survival in the United States: a SEER study. Otolaryngol Head Neck Surg 156(1): 122-131.
-
Al-Shemmary AM (2015) Molecular Study of Epstein Barr Virus, P16 and Bcl2 Gene Expression in Tissues from Nasopharyngeal Carcinoma Patients. MSC thesis, University of Babylon.
-
López-Hernández A, Vivanco B, Franchi A, Bloemena E, Cabal VN, et al. (2018) Genetic profiling of poorly differentiated sinonasal tumours. Scientific reports 8(1): 3998-4003.
-
Agaoglu FY, Dizdar Y, Dogan O, Alatli C, Ayan I, et al. (2004) P53 Overexpression in Nasopharyngeal Carcinoma. In vivo 18(5): 555-560.
-
Adam AA, Abdullah NE, El Hassan LA, Elamin EM, Ibrahim ME, et al. (2014) Detection of Epstein-Barr Virus in Nasopharyngeal Carcinoma in Sudanese by in Situ Hybridization. Journal of Cancer Therapy 5(6): 517- 524.
-
Agaimy A (2016) Poorly differentiated sinonasal tract malignancies: A review focusing on recently described entities. Cesk Patol 52(3): 146-153.
-
Lu S, Chang H, Sun X, Zhen Z, Sun F, et al. (2016) Long- term outcomes of nasopharyngeal carcinoma in 148 children and adolescents. Medicine 95(17): 3445-3451.
-
Long M, Fu Z, Li P, Nie Z (2017) Cigarette smoking and the risk of nasopharyngeal carcinoma: a meta-analysis of epidemiological studies. BMJ Open 7(10): 16582-16588.
-
Sarmiento MP, Mejia MB (2014) Preliminary assessment of nasopharyngeal carcinoma incidence in the Philippines: a second look at published data from four centers. Chin J Cancer 33(3): 159-164.
-
Shah AA, Evans MF, Adamson CC, Peng Z, Rajendran V, et al. (2010) HPV DNA is associated with a subset of Schneiderian papillomas but does not correlate with p16 INK4a immune reactivity. Head Neck Pathol 4(2): 106-112.
-
Wu D, Bleier BS, Wei Y (2018) Progression from nasal polyps to adult-onset asthma: a different process from atopic march?. Rhinology online 1(1): 22-29.
-
(2015) Iraqi Cancer Registry.
-
Fadly F, Farhat F, Asnir RA (2018) Profile of sinonasal malignant tumor patients in Adam Malik General Hospital Medan-Indonesia. Bali Medical Journal 7(1): 137-140.
- Acido Labile or Gastro Irritant Apis and Enteric Release in Galenic Practice: An Overview
- A Study on Knowledge, Attitude and Practice of Hand Hygiene among Healthcare Professionals at a Tertiary Care Hospital, India
- Influence of Inoculum Concentration on In Vivo Incubation Period of Emmia lacerata, Pathogenesis and Management of Wilt in Pepper (Capsicum annuum L.)
- Vanilla’s Chemistry
- Marine Anti-Cancer Compounds and Adverse Effects of Global Warming on Oceans: An Overview
- Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State