Exploring the Interplay of Socio-Demographic Factors, Medication Preferences, and Adherence Behaviors in Candidiasis Treatment Outcomes in Ghanaian Females
Introduction: Candidiasis, a fungal infection caused primarily by Candida species, affects millions of people worldwide, particularly women. Despite the availability of antifungal treatments, treatment failures remain a significant challenge. This study aimed to identify factors contributing to treatment failures in candidiasis among females in the Wa Municipality, Upper West Region of Ghana, to inform targeted interventions and improve patient outcome Methodology: A cross-sectional survey was conducted among 93 females with a history of candidiasis using a structured questionnaire. Descriptive statistics and correlations were used to analyse the data. Results: The majority of participants (92%) were aged between 11-30 years. More than half correctly identified candidiasis as a yeast infection, while others attributed it to poor hygiene and filthy environments. Oral medication was the most preferred treatment. Significant correlations were found between education, age, drug acquisition source, and treatment-related variables. Incomplete dosage intake was common, with reasons including perceived healing and saving medication for future use. Conclusion: The findings highlight the need for targeted interventions to improve candidiasis prevention, diagnosis, and management in the region. Recommendations include strengthening public education, enhancing access to quality-assured antifungal medications, promoting adherence support, and establishing antifungal resistance surveillance
Abbreviations
VVC: Vulvovaginal Candidiasis; UWR: Upper West Region; GSS: Ghana Statistical Service.
Introduction
Candidiasis, an infection caused by the yeast Candida species, is a common health issue with recurrent vaginal candidiasis (vulvovaginal candidiasis) affecting millions of women worldwide [1, 2]. Candida spp. constitute part of the microflora residing alongside bacteria in various parts of the body, including the oropharyngeal cavity, gastrointestinal and vaginal tract, and the skin, without usually posing any threat to the health of a person [3]. However, under certain conditions fungal growth is promoted, resulting in rapid multiplication which in turn cause infection [4]. Vulvovaginal candidiasis (VVC) or vaginal thrush, is a particularly prevalent form of the disease, affecting approximately 75% of women at least once during their reproductive years [5, 6, 7]. While most cases of VVC are mild, some women may experience severe symptoms such as redness, swelling, and fissures in the vaginal wall [8, 9], causing significant discomfort and impacting their quality of life [5].
Candida albicans is the primary culprit responsible for about 90% of VVC cases, with Candida glabrata accounting for the majority of the remaining infections [10]. Common symptoms of vaginal candidiasis include itching, soreness, pain during sexual intercourse or urination, and abnormal vaginal discharge [5, 8, 9]. Although Candida infections rarely lead to serious complications in healthy individuals, invasive candidiasis poses a significant threat in healthcare settings, especially among patients with weakened immune systems [11, 12]. This form of the disease can cause substantial morbidity and mortality, highlighting the importance of effective prevention and treatment strategies [11, 13, 14].
With a limited range of front-line antifungal medications available for treating candida, resistance remains a public health concern [12, 15, 16]. The emergence of drug-resistant Candida strains can complicate treatment and contribute to recurrent infections [17]. Self-diagnosis and improper treatment of VVC can also lead to persistent symptoms and increased risk of complications. Recurrent VVC may be attributed to various factors, including treatment-resistant Candida species, frequent antibiotic use, contraceptives, compromised immune function, sexual activity, and underlying health conditions such as diabetes [18].
Treatment failures in candidiasis can stem from a variety of factors, including patients not adhering to prescribed medication regimens as a result of their beliefs fears and concerns, perceiving symptom improvement after a few days and discontinuing treatment prematurely, and engaging in self-medication [19]. Poor hygiene practices, lack of proper diagnosis, and the development of drug-resistant strains can also contribute to recurrent infections [16, 17, 18]. Furthermore, interactions between certain medications and diets may influence the effectiveness of candidiasis treatment [20, 21].
Additionally, some medical practitioners may fail to perform the necessary laboratory examinations to confirm the infection status of the patient before initiating treatment, which can lead to misdiagnosis and inappropriate therapy, ultimately contributing to the recurrence of the infection. More so, patients’ reluctance to take prescribed medications as directed can further exacerbate the problem of treatment failure [18]. The complex interplay of these factors underscores the need for a comprehensive approach to understanding and addressing the challenges associated with candidiasis treatment. This study therefore focuses on identifying the factors contributing to treatment failures in candidiasis among females in the Wa Municipality of the Upper West Region who have previously been infected with the condition. Given the significance of antifungal resistance in shaping treatment policies and guiding evidence-based healthcare practices, effectively managing surveillance data on this issue is crucial. As the first study of its kind in the region, the findings could provide public health agencies with the evidence needed to develop targeted advocacy programs aimed at educating the public about key aspects of antifungal resistance. More so, the results of this study may serve as a valuable baseline for future surveillance efforts in the region.
Methodology
Study Area
The study was conducted in the Wa Municipality, which is the capital of the Upper West Region (UWR) of Ghana from January 2021-to-June 2021. The municipality has an estimated population of 107,214, representing 15.3% of the region’s total population and 3% of the national population (Ghana Statistical Service (GSS), 2021). Males constitute 49.7%, while females represent 50.3% of the population. The municipality is situated within latitude 1040’N to 2045’N and longitude 90W to 10020’W, sharing boundaries with the Nadowli District to the North, Wa East to the East, and Wa-West District to the West and South. It covers a land area of approximately 579.86 square kilometres, which is about 6.4% of the region [22].
Study Design, Population and Size
This study employed a cross-sectional survey design and a descriptive quantitative approach to provide more information on the causes of treatment failure in candidiasis. A well-structured, closed-ended questionnaire was used to gather data from participants regarding their perception, knowledge, and attitude towards the treatment of candidiasis. The questionnaire was distributed to 93 females with a previous record of candidiasis, comprising 49 tertiary students, 43 senior high school students, and 1 junior high school student from different religious backgrounds selected using purposive sampling of individuals who met the inclusion criteria.
Inclusion and Exclusion Criteria
All females who had a history of candidiasis were included in the study, however, females who met the inclusion criteria but had other underlying health conditions were excluded.
Study Procedures
The study was explained to participants in their most familiar languages to gather information regarding their employment status, educational level, knowledge of candidiasis, experiences during infection, compliance with treatment schedules, and socio-demographic features through a set of questionnaires.
Data Analysis
Data were analysed using SPSS software (version 20). Descriptive statistical analysis was used to explore participants’ responses in percentages. Correlations between the point of drug acquisition, drug intake instructions, treatment duration, participants’ age, educational background, and reasons for not completing medications were examined to determine whether one parameter affected the other. Statistical significance was set at p<0.05.
Results
The majority of participants (92%) were between the ages of 11 and 30 years old. Most participants had attained tertiary-level education, while 46% had completed senior high school. The study included participants from different religious backgrounds, with Christianity being the most prevalent (Table 1).
| Demographic characteristics | Percentage | |
|---|---|---|
| Age category | 11-20 years | 44 |
| 21-30 years | 48 | |
| 31-40 years | 8 | |
| Educational status | Junior High School | 1 |
| Senior High School | 46 | |
| Tertiary | 53 | |
| Religion | Christianity | 61 |
| Islam | 38 | |
| Traditional | 1 |
Table 1: Demographic characteristics of participants.
More than half of the participants correctly identified candidiasis as a yeast infection, while others attributed the cause to factors such as filthy environment and poor hygiene. Proper hygiene was recognized by the majority as a means to control candidiasis, followed by compliance with medication. The most common symptoms reported were vaginal itching, vaginal discharge, and pain or discomfort during urination. Over half of the participants did not complete their prescribed dosage because they felt they had been healed, while others cited reasons such as keeping the medication for future use, or finding the prescribed amount to be excessive, for not completing the prescribed dosage (Table 2).
| Knowledge based questions | Views | Percentage |
|---|---|---|
| Knowledge on causes of candidiasis | Diet | 5 |
| Filthy environment | 21 | |
| Poor hygiene | 19 | |
| Witch craft | 3 | |
| Yeast infection | 52 | |
| Knowledge on the control of candidiasis | Complying with medication | 21.51 |
| Keeping a clean environment | 6.45 | |
| Proper hygiene | 55.91 | |
| Proper hygiene and complying with medication | 12.9 | |
| Proper hygiene and keeping a clean environment | 2.15 | |
| Proper hygiene, keeping a clean environment and complying with medication | 1.08 |
Pain and discomfort during sex 2.2
- Pain and discomfort during sex and vaginal discharge
- 1.1
- Pain and discomfort during urination and vaginal discharge
- 1.1
- Pain and discomfort during urination and vaginal itching
- 6.5
- Pain and discomfort during urination, vaginal itching and vaginal discharge
- 6.5
- Pain, discomfort during urination, vaginal itching, vaginal discharge and fever
- 1.1 knowledge on symptoms of candidiasis
- Pain and discomfort during urination, vaginal itching, vaginal discharge and pain and discomfort during sex
- 3.2
- Pain and discomfort during urination and vomiting
- 1.1
- Pain and discomfort during urination, vaginal itching and vomiting
- 1.1
- Vaginal itching, vaginal discharge, pain and discomfort during sex
- 5.4
- Reasons for not completing their prescribed dosage
Table 3: Responses to knowledge-based question.
Pain and discomfort during urination 8.6
Vaginal discharge 19.4
Vaginal itching 26.9
Vaginal itching and vaginal discharge 12.9
- Pain and discomfort during sex and vaginal discharge
- 1.1
- Pain and discomfort during urination and vaginal discharge
- 1.1
- Pain and discomfort during urination and vaginal itching
- 6.5
- Pain and discomfort during urination, vaginal itching and vaginal discharge
- 6.5
- Pain, discomfort during urination, vaginal itching, vaginal discharge and fever
- 1.1 knowledge on symptoms of candidiasis
- Pain and discomfort during urination, vaginal itching, vaginal discharge and pain and discomfort during sex
- 3.2
- Pain and discomfort during urination and vomiting
- 1.1
- Pain and discomfort during urination, vaginal itching and vomiting
- 1.1
- Vaginal itching, vaginal discharge, pain and discomfort during sex
- 5.4
- Reasons for not completing their prescribed dosage
Table 3: Responses to knowledge-based question.
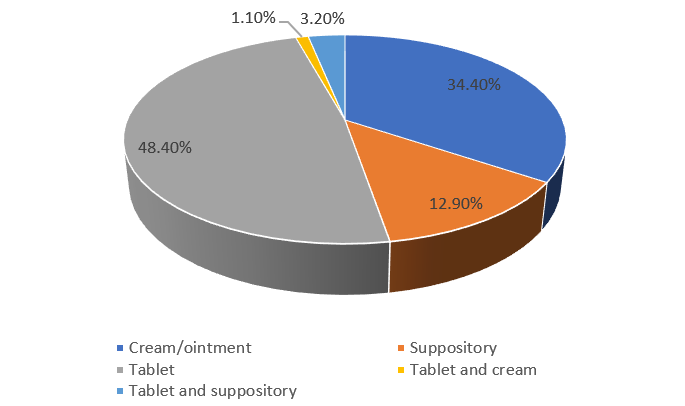
In some cases, the preferred medications type may be inappropriate for the circumstance, however since the participant is not being offered a preferred option, the possibility of not complying with dosage instruction is high. The bar graph Figure 1 illustrates participants’ preferences Vomiting 3.2 Completed dosage 25.8 Got healed 55.9 Kept for future use 8.6 Drugs were too much 9.7 for different types of candidiasis medication. The most preferred medication type was oral medication, followed by topical creams. Suppositories were the least preferred option among the participants.
Several significant relationships between various parameters were observed in the study (Table 3). There was a strong negative correlation between the educational level of participants and the duration of treatment, suggesting that participants with higher education levels tend to have shorter treatment durations. The reason for incomplete dosage intake negatively correlated with the educational level of participants and positively correlated with the duration of treatment. The source of drug acquisition positively correlated with the educational level of participants and negatively correlated with the reason for incomplete dosage intake. Participants’ knowledge of the causes of candidiasis positively correlated with their educational level and negatively correlated with the reason for incomplete dosage intake and the duration of treatment. The age of participants positively correlated with their educational level and negatively correlated with the reason for incomplete dosage intake and the duration of treatment (Table 3).
| Educational level of participant | Reason for incomplete dosage intake | Reason for medication preference | Duration of treatment | ||
|---|---|---|---|---|---|
| Educational level of participant | Pearson Correlation | 1 | -.294** | 0.164 | -.606** |
| Sig. (2-tailed) | 0.004 | 0.116 | 0 | ||
| Reason for incomplete dosage intake | Pearson Correlation | -.294** | 1 | -0.077 | .274** |
| Sig. (2-tailed) | 0.004 | 0.463 | 0.008 | ||
| Reason for medication preference | Pearson Correlation | 0.164 | -0.077 | 1 | -0.058 |
| Sig. (2-tailed) | 0.116 | 0.463 | 0.578 | ||
| Duration of treatment | Pearson Correlation | -.606** | .274** | -0.058 | 1 |
| Sig. (2-tailed) | 0 | 0.008 | 0.578 | ||
| Source of drug acquisition | Pearson Correlation | .303** | -.341** | 0.113 | -0.161 |
| Sig. (2-tailed) | 0.003 | 0.001 | 0.279 | 0.123 | |
| Participant knowledge on causes of candidiasis | Pearson Correlation | .456** | -.211* | 0.196 | -.365** |
| Sig. (2-tailed) | 0 | 0.042 | 0.06 | 0 | |
| Age of participant | Pearson Correlation | .719** | -.325** | 0.142 | -.550** |
| Sig. (2-tailed) | 0 | 0.001 | 0.174 | 0 |
Table 4: Correlations between various parameters. **.Correlation is significant at the 0.01 level (2-tailed). *.Correlation is si
The cross-tabulation between the age of participants and the source of medication shows that the majority of participants in all age groups acquired their medication from hospitals, followed by pharmacies. A small number of participants in the 11-20 and 21-30 age groups obtained their medication from friends and relatives or herbalists (Table 4).
| Source of medication | Total | ||||||
|---|---|---|---|---|---|---|---|
| Friends and relatives | Herbalists | Hospitals | Pharmacy | Pharmacy and hospital | |||
| Age of participant | 11-20 | 7 | 4 | 22 | 8 | 0 | 41 |
| 21-30 | 4 | 0 | 19 | 19 | 3 | 45 | |
| 31-40 | 1 | 0 | 4 | 1 | 1 | 7 | |
| Total | 12 | 4 | 45 | 28 | 4 | 93 |
Table 5: Cross tabulation between age of participants and source of medication.
The majority of participants in the 21-30 and 31-40 age groups correctly identified yeast infection as the cause of candidiasis. However, a significant number of participants in the 11-20 age group attributed the cause to factors such as a filthy environment, poor hygiene, and witchcraft (Table 5).
| Participant knowledge on causes of candidiasis | Total | ||||||
|---|---|---|---|---|---|---|---|
| Diet | Filthy environment | Poor hygiene | Witchcraft | Yeast infection | |||
| Age of participant | 11-20 | 3 | 14 | 10 | 3 | 11 | 41 |
| 21-30 | 2 | 3 | 7 | 0 | 33 | 45 | |
| 31-40 | 0 | 2 | 1 | 0 | 4 | 7 | |
| Total | 5 | 19 | 18 | 3 | 48 | 93 |
Table 6: Linkage between age of participants and their knowledge on causes of candidiasis.
From the table above, majority of participants indicated that yeast infection was the major cause of candidiasis as per scientific literature while a few participants inappropriately chose the cause of the condition to be witchcraft.
The link between the educational level to knowledge of the causes of candidiasis showed that the majority of participants with tertiary education correctly identified yeast infection as the cause. Participants with senior high school education had more varied responses, with some attributing the cause to factors such as a filthy environment, poor hygiene, and witchcraft. The single participant with junior high school education selected a filthy environment as the cause (Table 6).
| Knowledge on causes of candidiasis | ||||||
|---|---|---|---|---|---|---|
| Diet | Filthy environment | Poor hygiene | Witchcraft | Yeast infection | ||
| Educational level of participant | JHS | 0 | 1 | 0 | 0 | 0 |
| SHS | 3 | 14 | 12 | 3 | 11 | |
| Tertiary | 2 | 4 | 6 | 0 | 37 | |
| Total | 5 | 19 | 18 | 3 | 48 |
Table 7: Linkage between knowledge on causes of candidiasis and educational level.
Discussion
This study provides valuable insights into the factors contributing to treatment failures in candidiasis among females in the Upper West Region of Ghana. The results highlight several key issues that are consistent with findings from other studies on Candida infections and antifungal resistance. One notable result is that the majority of participants were between the ages of 11 and 30 years old (Table 1). This is in line with research indicating that vulvovaginal candidiasis (VVC) is particularly prevalent among women of reproductive age [23, 24]. The high incidence of VVC in this age group may be attributed to factors such as hormonal changes, sexual activity, and use of certain contraceptives that can disrupt the vaginal microbiome and facilitate Candida overgrowth [24].
The study also found that more than half of the participants correctly identified candidiasis as a yeast infection, with others attributing the cause to factors such as poor hygiene and filthy environments. This mixture of accurate and inaccurate perceptions about the causes of candidiasis is consistent with findings from other studies in developing countries [18]. Misconceptions about the aetiology of VVC can lead to inappropriate self-treatment, delays in seeking medical care, and non-adherence to prescribed antifungal regimens [18]. Improving public knowledge about the true causes and risk factors for candidiasis could help promote better prevention and treatment-seeking behaviours.
Interestingly, the most preferred medication type among participants was oral medication, followed by topical creams, with suppositories being the least preferred. This contrasts with some studies that have found topical azole antifungals to be the first-line treatment for uncomplicated VVC [11, 19]. The preference for oral medications in this study may reflect cultural attitudes, ease of use, or limited access to or familiarity with other treatment options in the region. Oral fluconazole is effective for VVC treatment, but resistance is a growing concern [17, 25]. More research is needed to understand the factors driving medication preferences and ensure that preferred, effective options are available and properly used.
The study uncovered several significant correlations that shed light on the complex interplay of factors influencing treatment outcomes. Higher educational levels were associated with shorter treatment durations, better knowledge of the causes of candidiasis, and a lower likelihood of incomplete dosage intake. This suggests that education plays a key role in promoting adherence to treatment and reducing the risk of recurrent infections. Health literacy and knowledge have been identified as important determinants of health behaviours and outcomes in various contexts [26, 27].
The source of drug acquisition was another factor that correlated with treatment-related variables. Acquiring drugs from hospitals or pharmacies was associated with higher educational levels and a lower likelihood of incomplete dosage intake compared to obtaining medication from informal sources like friends or herbalists. This highlights the importance of access to quality-assured antifungal medications and proper medical guidance for effective treatment. Self-medication and use of untested alternative remedies have been identified as risk factors for treatment failure and antifungal resistance in other studies [11, 19, 24].
Age also significantly correlated with several key variables. Older age groups had higher educational levels, better knowledge of candidiasis aetiology, and were less likely to have incomplete dosage intake or longer treatment durations. This may reflect greater health literacy, access to care, and treatment adherence among older women compared to adolescents and young adults. Tailoring education and support strategies to different age groups may help optimize treatment outcomes.
The study’s location in the Upper West Region of Ghana, characterized by a tropical savanna climate with distinct wet and dry seasons, raises important considerations about the potential impact of climatic conditions on candidiasis incidence. Hot and humid environments can promote fungal growth and potentially increase the risk of Candida infections. This contrasts with more temperate regions, where seasonal variations in temperature and humidity may lead to different patterns of infection prevalence. Studies in temperate climates have reported seasonal fluctuations in vulvovaginal candidiasis, with some finding higher rates during warmer months [28]. However, the year-round warm and often humid conditions in tropical regions like Ghana may contribute to a more consistent incidence of candidiasis throughout the year. Furthermore, limited access to air conditioning and challenges in maintaining personal hygiene during hot seasons could exacerbate risk factors for infection in this setting. Additionally, the standard of living and access to advanced medical care play crucial roles in the incidence and management of candidiasis. Higher-income regions often have better access to a wider range of antifungal medications, including newer formulations with improved efficacy and reduced side effects. This access, combined with better healthcare infrastructure and education, can lead to more effective prevention, diagnosis, and treatment of candidiasis, potentially reducing its incidence and recurrence rates compared to regions with limited resources. Future research should explore the relationship between local climate patterns, hygiene practices, and candidiasis incidence to inform targeted prevention strategies that account for environmental factors specific to the region.
The findings on the reasons for incomplete dosage intake, such as feeling healed before finishing the prescribed course or saving medication for future use, are consistent with common challenges in antimicrobial adherence. Similar issues have been reported in studies on antibiotic use and the development of antimicrobial resistance [6, 11, 18]. Poor adherence to antifungal therapy can lead to persistent infections, recurrent episodes, and the selection of resistant Candida strains [19, 29]. Emphasizing the importance of completing the full course of antifungal treatment, even after symptoms resolve, is crucial for preventing these negative outcomes.
An important consideration is the potential for antifungal resistance among Candida isolates in this population. This study did not directly assess resistance profiles, but other research has highlighted the global emergence of resistance to commonly used antifungal drugs [30, 31]. Rising rates of non-albicans Candida species with reduced susceptibility to azoles and echinocandins pose additional therapeutic challenges [32]. Surveillance of local resistance patterns and tailoring treatment guidelines accordingly will be essential for optimizing care and preventing the spread of resistant strains.
Conclusion
In conclusion, this study provides valuable insights into the factors contributing to treatment failures in candidiasis among females in the Upper West Region of Ghana. The findings highlight the complex interplay of socio-demographic characteristics, knowledge, medication preferences, and adherence behaviours in shaping treatment outcomes. The high prevalence of candidiasis among women of reproductive age underscores the need for targeted interventions to improve the prevention, diagnosis, and management of this common infection. Misconceptions about the causes of candidiasis, preferences for oral medications, and incomplete dosage intake emerged as key challenges that may hinder effective treatment.
The significant correlations between education, age, source of drug acquisition, and treatment-related variables provide valuable insights for designing strategies to optimize care. Strengthening health literacy, ensuring access to quality-assured medications, and promoting adherence support tailored to different age groups could help reduce the burden of recurrent and refractory infections.
However, the study’s reliance on self-reported data and cross-sectional design limits the ability to draw causal inferences and assess objective measures of infection and resistance. Future research should employ longitudinal designs, triangulate data sources, and incorporate laboratory testing to provide a more comprehensive understanding of the determinants and consequences of treatment failure.
Furthermore, the potential for antifungal resistance in this population warrants close monitoring and consideration in treatment guidelines. Surveillance of local resistance patterns and judicious use of antifungal agents will be critical for preserving the effectiveness of available therapies and preventing the spread of resistant strains. Overall, this study lays the groundwork for further research and action to address the challenges of candidiasis treatment in the Upper West Region of Ghana.
Recommendations
Based on the findings of this study, the following recommendations are proposed to address the challenges of candidiasis treatment failure in the Upper West Region of Ghana:
- Strengthen public education and awareness campaigns to improve knowledge about the causes, risk factors, and proper management of candidiasis. These efforts should target women of reproductive age and be tailored to different educational and age groups to ensure widespread understanding and adoption of preventive and treatment-seeking behaviours. Healthcare providers, community leaders, and media outlets can play key roles in disseminating accurate information and dispelling misconceptions about the infection.
- Enhance access to quality-assured antifungal medications through formal healthcare channels, such as hospitals and pharmacies. Strategies may include increasing the availability and affordability of essential antifungal drugs, training healthcare providers on appropriate prescribing practices, and enforcing regulations to curtail the distribution of counterfeit or substandard medications. Collaborative efforts between public health agencies, healthcare facilities, and pharmaceutical companies can help ensure a reliable supply of effective antifungal agents.
- Develop and implement adherence support interventions to promote the complete and proper use of prescribed antifungal regimens. These may involve patient education on the importance of finishing the full course of treatment, even after symptom resolution, as well as the risks of saving medications for future self-treatment. Simplified dosing schedules, reminder systems, and follow-up care can also help foster adherence. Healthcare providers should be trained to provide clear instructions, assess adherence barriers, and offer ongoing support to patients throughout the treatment process.
- Establish a surveillance system to monitor local trends in antifungal resistance and inform treatment guidelines. This may involve periodic sampling and susceptibility testing of Candida isolates from clinical settings, as well as tracking prescribing patterns and treatment outcomes. The data generated can guide the selection of appropriate antifungal agents, identify emerging resistance threats, and evaluate the impact of interventions to optimize treatment effectiveness. Collaboration between healthcare facilities, public health agencies, and research institutions can facilitate the implementation and sustainability of surveillance efforts.
- By implementing these recommendations, the Upper West Region of Ghana can take important steps towards reducing the burden of candidiasis treatment failure and improving the health outcomes of affected women.
Acknowledgements
The authors of this study are grateful to the participants who granted consent to participate in this study.
Competing Interests
“The authors have no relevant financial or non-financial interests to disclose”.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Consent to Participate
Permission was sought from participants via written informed consent. The purpose and necessity of the research was fully explained to the participants as well as the risks and benefits.
Availability of Data
All data used in this study are available upon reasonable request.
Author Contributions
EUO developed the concept and directed the research as well as participated in the finalizing of the manuscript. JBK, FBB, and DTM carried out sample collection, data analysis and manuscript preparation. REA and EAB coordinated and helped draft the manuscript as well as designed the sampling techniques and performed data analysis. All authors read and approved the final manuscript.
References
-
Denning DW, Kneale M, Sobel JD, Rautemaa-Richardson R (2018) Global burden of recurrent vulvovaginal candidiasis: a systematic review. Lancet Infect Dis 18(11): e339-437.
-
Odds FC (1994) Pathogenesis of Candida infections. J Am Acad Dermatol 31(3): S2-S5.
-
Asif H, Qadir MI (2019) An Overview to Candidiasis-A Candida Infection. International Journal of Advanced Research in Microbiology and Immunology 2(1): 31-33.
-
Talapko J, Juzbašić M, Matijević T, Pustijanac E, Bekić S, et al. (2021) Candida albicans—The Virulence Factors and Clinical Manifestations of Infection. Journal of Fungi 7(2): 79.
-
Blostein F, Levin-Sparenberg E, Wagner J, Foxman B (2017) Recurrent vulvovaginal candidiasis. Ann Epidemiol 27(9): 575-582.
-
Foxman B, Muraglia R, Dietz JP, Sobel JD, Wagner J (2013) Prevalence of Recurrent Vulvovaginal Candidiasis in 5 European Countries and the United States. J Low Genit Tract Dis 17(3): 340-345.
-
Balakrishnan SN, Yamang H, Lorenz MC, Chew SY, Than LTL (2022) Role of Vaginal Mucosa, Host Immunity and Microbiota in Vulvovaginal Candidiasis. Pathogens 11(6): 618.
-
Eckert L, Hawas SE, Stevens CE, Koutsky LA, Eschenbach DA, et al. (1998) Vulvovaginal candidiasis: clinical manifestations, risk factors, management algorithm. Obstetrics & Gynecology 92(5): 757-765.
-
Geiger AM, Foxman B (1996) Risk Factors for Vulvovaginal Candidiasis. a case-control study among university students 7(2):182-187.
-
Jeanmonod R, Chippa V, Jeanmonod D (2024) Vaginal Candidiasis. StatPearls [Internet].
-
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, et al. (2016) Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clinical Infectious Diseases. 62(4): e1-50.
-
Parslow BY, Thornton CR (2022) Continuing Shifts in Epidemiology and Antifungal Susceptibility Highlight the Need for Improved Disease Management of Invasive Candidiasis. Microorganisms 10(6): 1208.
-
Saville SP, Lazzell AL, Monteagudo C, Lopez-Ribot JL (2003) Engineered Control of Cell Morphology In Vivo Reveals Distinct Roles for Yeast and Filamentous Forms of Candida albicans during infection. Eukaryot Cell 2(5): 1053-1060.
-
Toda M, Williams SR, Berkow EL, Farley MM, Harrison LH, et al. (2019) Population-Based Active Surveillance for Culture-Confirmed Candidemia — Four Sites, United States, 2012–2016. MMWR Surveillance Summaries 68(8): 1-15.
-
Ostrosky-Zeichner L, Casadevall A, Galgiani JN, Odds FC, Rex JH (2010) An insight into the antifungal pipeline: selected new molecules and beyond. Nat Rev Drug Discov 9(9): 719-727.
-
Bassetti M, Righi E, Montravers P, Cornely OA (2018) What has changed in the treatment of invasive candidiasis? A look at the past 10 years and ahead. J Antimicrob Chemother 73(S1): i14-i25.
-
Perea S, Patterson TF (2002) Antifungal Resistance in Pathogenic Fungi. Clin Infect Dis 35(9): 1073–1080.
-
M Lema V (2017) Recurrent Vulvo-Vaginal Candidiasis: Diagnostic and Management Challenges in a Developing Country Context. Obstet Gynecol Int J 7(5): 00260.
-
Erfaninejad M, Salahshouri A, Amirrajab N (2022) Barriers and facilitators of adherence to treatment among women with vulvovaginal candidiasis: a qualitative study. Eur J Med Res 27(1): 303.
-
Jeziorek M, Frej-Mądrzak M, Choroszy-Krol I (2019) The influence of diet on gastrointestinal Candida spp. colonization and the susceptibility of Candida spp. to antifungal drugs. Rocz Panstw Zakl Hig 70(2): 195-200.
-
Palmucci JR, Sells BE, Giamberardino CD, Toffaletti DL, Dai B, et al. (2024) A ketogenic diet enhances fluconazole efficacy in murine models of systemic fungal infection. mBio15(5): e0064924.
-
(2021) Ghana Statistical Service (GSS). Ghana 2021 Population and housing census general report. Accra.
-
Rathod SD, Klausner JD, Krupp K, Reingold AL, Madhivanan P (2012) Epidemiologic Features of Vulvovaginal Candidiasis among Reproductive-Age Women in India. Infect Dis Obstet Gynecol 2012: 1-8.
-
Goncalves B, Ferreira C, Alves CT, Henriques M, Azeredo J, et al. (2016) Vulvovaginal candidiasis: Epidemiology, microbiology and risk factors. Crit Rev Microbiol 42(6): 905-927.
-
Zhang J, Liu J, Liu F, Xia Y, Wang J, et al. (2014) Vulvovaginal candidiasis : species distribution, fluconazole resistance and drug efflux pump gene overexpression. Mycoses 57(10): 584-591.
-
Levy H, Janke A (2016) Health Literacy and Access to Care. J Health Commun 21(S1): 43-50.
-
Kinoshita S, Hirooka N, Kusano T, Saito K, Aoyagi R (2024) Does health literacy influence health-related lifestyle behaviors among specialists of health management? A cross-sectional study. BMC Prim Care 25(1): 29.
-
Spence D (2010) Candidiasis (vulvovaginal). BMJ Clin Evid 2010: 0815.
-
Mathema B, Cross E, Dun E, Park S, Bedell J, et al. (2001) Prevalence of Vaginal Colonization by Drug‐Resistant Candida Species in College‐Age Women with Previous Exposure to Over‐the‐Counter Azole Antifungals. Clin Infect Dis 33(5): e23-e27.
-
Fisher MC, Hawkins NJ, Sanglard D, Gurr SJ (2018) Worldwide emergence of resistance to antifungal drugs challenges human health and food security. Science 360(6390): 739-742.
-
Perlin DS (2015) Mechanisms of echinocandin antifungal drug resistance. Ann N Y Acad Sci 1354(1): 1-11.
-
Wiederhold N (2017) Antifungal resistance: current trends and future strategies to combat. Infect Drug Resist 10: 249-259.
- Acido Labile or Gastro Irritant Apis and Enteric Release in Galenic Practice: An Overview
- A Study on Knowledge, Attitude and Practice of Hand Hygiene among Healthcare Professionals at a Tertiary Care Hospital, India
- Influence of Inoculum Concentration on In Vivo Incubation Period of Emmia lacerata, Pathogenesis and Management of Wilt in Pepper (Capsicum annuum L.)
- Vanilla’s Chemistry
- Marine Anti-Cancer Compounds and Adverse Effects of Global Warming on Oceans: An Overview
- Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State