Kaposiform Hemangioendothelioma Complicated by a Kasabach-Merritt Syndrome: Report of a Case
Kaposiform hemangioendothelioma (KHE) is a very rare form of vascular tumor, which is complicated by intra-tumor coagulopathy and requiring urgent management. Objective: we report a case of a KHE, complicated by a kasabach merrit syndrome compiled in the neonatology department of Mohamed VI university hospital, Marrakech and we discuss the different therapeutic modalities. Observation: a newborn was admitted, on the third day of life, for jaundice associated with a purplish red swelling of the left hemi face. He had anemia and thrombocytopenia requiring repeated transfusions. In view of the instrumental delivery, a hematoma was initially evoked. But in the absence of improvement, the eventuality of a hemangioma or complicated tumor became more likely. The patient was treated by propranolol in addition to high dose of oral corticosteroids and a skin biopsy was realized. Despite treatment, the patient died 10 days later due to a disseminated intravascular coagulation. A posteriori the histological study confirmed the KHE. Conclusion: a codified and early therapeutic protocol is necessary to improve the prognosis of patients with KEH, especially since other therapeutics has proved their effectiveness in the literature.
Baddouh N¹*, Bennaoui F¹, El idrissi Slitine N¹, Berrada S², Hazmiri
FZ², Rais H², Maja N3, Hocar O3, Amal S3 and Maoulainine FMR¹
¹Neonatal Intensive Care Unit, Mohammed VI University Hospital, Marrakesh, Morocco
²Department of pathology, Mohammed VI University Hospital, Marrakesh, Morocco
Tel: 212672050984; Email: naima_102@hotmail.com
coagulopathy and requiring urgent management.
intravascular coagulation. A posteriori the histological study confirmed the KHE.
especially since other therapeutics has proved their effectiveness in the literature.
Introduction
Soft tissue tumors account for approximately 25% of neonatal tumors and are most often benign (more than 2/3 of cases). Vascular tumors are the most frequent benign tumors. Infantile hemangioma accounts for 32% of these tumors, affecting 1 out of 200 children at birth [1]. The international society of vascular disorders classifies vascular tumors as: the kaposiform hemangioendothelioma (KHE), the tufted angiomas (tTA), infantile hemangiomas, congenital hemangiomas and other rarer forms of tumors [2]. Kaposiform hemangioendothelioma is a very rare form of vascular tumor with locally aggressive behavior. More than 50% of the KHE are complicated by an intra-tumor coagulopathy responsible for Kasabach-Merritt phenomenon (KMP) [3]. Clinically, KMP is defined by the association between a rapidly extensive violet red vascular tumor and thrombocytopenia, which can be complicated by hemorrhage and coagulation disorders [4]. We report a case of a newborn with a KHE complicated by a KMP treated inefficiently by corticosteroid in addition to propranolol and we discuss the different therapeutic options.
Case Report
We report the case of a male newborn, who was admitted to neonatal intensive care unit on the third day of life for jaundice associated with a large cutaneous lesion in the left hemi face. The mother was 24 years old, primi gravida, primi para, without any particular antecedent. The pregnancy was followed up. He was delivered vaginally with forceps. The apgar was normal at 5 min. The clinical examination at admission had found a newborn reactive icteric, pale, hemodynamically stable. The birth weight was at 3800 g; the height at 57 cm and the cranial perimeter at 36 cm. The skin of the left hemiface was indurated, with violet-red lesion, which extended to the neck. The left eyelid was also edematous (Figure 1 (A)). Malformative assessment was negative. Initially the most likely diagnosis was subcutaneous hematoma or subcutaneous fat necrosis due to the instrumental extraction.

Figure 1: Clinical case of kaposiform hemangioendothelioma with kasabach-Merritt phenomenon diagnosed in a 3-days-old patient. Photos taken at the department level. Extension of cutaneous lesion: A violet-red lesion in the left hemiface with irregular margins and edema of the left eyelid (A). Laboratory tests showed normocytic normochromic anemia: hemoglobin at 8.1 g / dl and deep thrombocytopenia: platelet at 6000 /mm3. The workup of jaundice revealed that the grouping of the baby and her mother was: O+. Total bilirubin was at 150.46 mg / l; direct bilirubin at 11.22 mg / l and indirect bilirubin at 139.2 mg / l. C reactive protein test was normal.
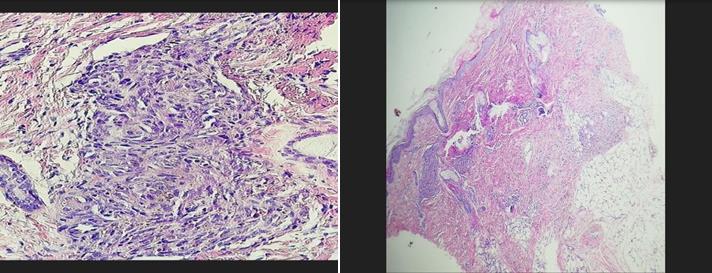
The newborn was transfused packed red blood cells, and treated by intensive phototherapy. The evolution was marked by the extension of swelling to the thorax, with the reappearance of pallor and the persistence of jaundice (Figure 1B & 1C). The hemogram confirmed anemia with deep thrombocytopenia: hemoglobin at 8.3 g/d; the platelets at 5000/mm3. An assessment of hemostasis was requested: Prothrombin time at 100% ; activated partial thromboplastin time at 30.6 seconds; fibrinogen at 0.21 g / l (decreased rate) and D dimmers> 4 μg / ml: (high level). The newborn had required several transfusions of red blood cells and platelets. The diagnosis of a hemangioma or extensive tumor complicated by disseminated intravascular coagulation became more likely. The ultrasound was inconclusive. Due to the unfavorable outcome, a skin biopsy was realized. Then the patient was treated by 2 mg / kg / day of propranolol and oral high dose of corticosteroid. The evolution has not changed with this therapy and the patient died by disseminated intravascular coagulation. A posteriori the anatomopathological study of the skin biopsy confirmed that the morphological and immuno- histochemical form of the tumor was a kaposiform hemangioendothelioma (Figure 2).
Discussion
Kaposiform hemangioendothelioma is a rare vascular tumors that occurs predominantly in infancy or early childhood. It was described for the first time in 1993 by Zukerberg, et al. and since this date less than 200 cases have been reported in the literature [5]. The incidence of KHE has been estimated at 0.071 per 100,000 children [4]. KHE presents with intermediate- malignant and locally aggressive characteristics but without distant metastases. More than 70% of KHE patients develop a life-threatening thrombocytopenia and coagulopathy, known as Kasabach-Merritt phenomenon. Additionally, KHE may be complicated by severe anemia due to blood sequestration and intra-lesional hemorrhage. KHE has high morbidity and mortality rates, resulting from the rapid growth of the tumor, compression or destruction of vital structures, and hemodynamic instability. [6]
Kaposiform hemangioendothelioma most commonly appears as an enlarging, firm, solitary, purpuric cutaneous or soft tissue lesion [4]. Often, several tissue planes are involved and the boundaries of the tumor are poorly defined. Kaposiform hemangioendothelioma typically involves the extremities, trunk, and retroperitoneum. The risk of KMP is greater with increased depth and infiltration of the vascular tumor and with retroperitoneal or intrathoracic involvement [7]. Kasabach-Merritt phenomenon is specific to KHE occurring in 70% of cases [4]. Clinically, KMP is often marked by a rapidly enlarging tumor, which may be painful. A profound thrombocytopenia and coagulopathy, including hypofibrinogenemia, characterizes KMP, and therefore, laboratory evaluation is essential for the diagnosis. This includes a complete blood count, fibrinogen, d-dimmer, prothrombin time (PT), and activated partial thromboplastin time (aPTT). Kasabach-Merritt phenomenon is characterized by very low platelet levels, commonly ranging from 3000 to 60 000 per micro liter [8]. Fibrinogen levels are significantly decreased and d- dimer and fibrin degradation products are elevated. The PT and the aPTT are typically normal to slightly elevated. Significant anemia can occur due to intra lesional bleeding, coagulopathy, sequestration of blood within the tumor, and/or hemolytic anemia secondary to the sheering of red blood cells in the abnormal vasculature of the tumor. Evoking the diagnosis of KHE should not lead to a biopsy without a hemostasis test [8]. In histological study, KHE is marked by irregular sheets of spindle-shaped endothelial cells and characteristic slit- like vascular channels, [9]. With positive immunohistochemical staining for lymphatic markers, D2-40, LYVE1, and Prox-1 [10], and negative for GLUT-1, the marker for infantile hemangioma. Immuno- histochemical stains are also positive for vascular markers CD31 and CD34 [7]. The rare superficial and limited forms of KHE can benefit from complete excision. Conversely, deep forms, especially when they are complicated by coagulation disorders, have an unfavorable prognosis. The largest published series of KHE (33 children) reports a mortality rate of 15% [7]. To distinguish KHE from infantile hemangioma is sometimes difficult. The two main elements that distinguish them are the absence of spontaneous regression of KEH lesions and the high incidence of intra tumor coagulopathy complicating KEH. Sometimes, only the immuno-histochemical study of GLUT-1 allows differentiating them. KMP is most likely whenever the vascular tumor has a purplish-red tint or is suddenly increased in volume [1]. The traumatic context of delivery in our case has delayed evoking the diagnosis of vascular tumor but the extension of the lesion and the unfavorable improvement of the patient led to reconsider the diagnosis. We associated the propranolol, a nonselective β- adrenergic antagonist, to high dose of corticosteroid in our case since numerous studies had demonstrated the success of propranolol for shrinking hemangiomas [11], the time to have the results of the skin biopsy to adjust the treatment, but this dual therapy was not enough in our patient.
Optimal treatment of Kaposiform hemangioendothelioma is not well established and depends on the extent of the tumor and on the clinical condition of the patient. Given the various therapies available to manage KMP, common decision by the physician and the family should be established regarding the best approach. Complete surgical resection offers the most definitive cure for small, localized tumors; for tumors that have decreased in size with medical therapy; or for life- threatening tumors [12]. However, surgical intervention at initial presentation with KHE is rarely feasible, given the infiltrative nature of the associated tumor and existing coagulopathy. Use of radiation therapy has been reported in KMP [13]. A response rate of 75% has been described with the use of radiation in conjunction with steroids [14]; however, radiation may have long-term complications, including growth arrest, developmental delay, and secondary malignancies, and therefore should be used with caution in younger patients. Successful use of embolization has also been described in patients with KMP [15]; Potential side effects include the risk of skin necrosis secondary to infarction of surrounding tissue and the risk of fatal bleeding with the use of heparin with catheter placement. Invasive interventions within the context of coagulopathy are associated with high-risk complications; therefore, pharmacologic management is often first line and can achieve hemostatic stability in KMP. Various small case series using monotherapy or multimodal therapies have been described involving steroids, vincristine [16], interferon- alfa [17], ant platelet agents, propranolol [18], and sirolimus with variable outcomes [19] and long-term side effects. Due to the large variability in management protocols, consensus- derived practice standards have been developed in 2013 by a multidisciplinary expert panel in North America from various institutions to provide a uniform approach to treat KHE with KMP and therefore allow for a cohesive comparison of responses and long-term outcomes [3]. The group recommends a regimen of systemic corticosteroids and weekly vincristine as standard of care for KHE associated with KMP [20]. During the same time, a phase II study [21] evaluating the safety and efficacy of sirolimus, an inhibitor of mammalian target for rapamycin, for the treatment of complicated vascular anomalies included 10 patients with KHE and KMP, and the response rate was impressive: 100% partial response of KHE, but with complete and quick resolution of KMP in all patients. The number of cases was small (as the incidence of the vascular tumors is low). However, considering the potential side effects of the 2 regimens (vincristine + steroids vs sirolimus + steroids) and mode of administration (intravenous for vincristine vs oral for sirolimus), many centers have adopted sirolimus + steroids as a first- line pharmacologic therapy. A multi- institutional study is underway to randomly assign patients to the 2 arms described above and evaluate treatment response. European groups have described successful outcomes with vincristine, aspirin, and ticlopidine in the treatment of vascular tumors with KMP [22]. Both aspirin and ticlopidine potentiate the inhibition of platelet aggregation. Successful use of aspirin and ticlopidine [23], vincristine and ticlopidine [24] in KMP has also been described. Vincristine is a cytotoxic drug with potential side effects, which include peripheral neuropathy, constipation, and syndrome of inappropriate ant diuretic hormone secretion. Steroids also have side effects, which include hypertension, hyperglycemia, adrenal insufficiency, and gastritis. The vincristine, aspirin, and ticlopidine regimen avoids use of steroids; however, aspirin use in children is associated with the potential risk of Reye syndrome, which is characterized by encephalopathy and liver failure, and therefore should be used with caution in children. Sirolimus with or without steroids is a therapeutic option that does not require a central line placement as both medical treatments are oral. Blood draws are necessary to assess the sirolimus level and adjust the dose based on the targeted value. These regimens have the potential side effects of steroids, as described above, in addition to the side effects of sirolimus, which include decreased immunity, mucositis, and dyslipidemia. The length of therapy is determined by resolution of KMP. Improvement in thrombocytopenia can be noted in days after initiation of pharmacologic therapy with significant improvement in coagulopathy in a few weeks [8]. A global consensus on the best first-line therapy is needed.
Conclusion
The management of HEK is based on a multidisciplinary approach (pediatrician, hematologist, dermatologist, radiologist and surgeon). Deep or complicated forms of kasabach-merritt syndrome are associated with an unfavorable prognosis. Propranolol and oral high-dose of corticosteroids were not useful for our patient. The absence of a codified therapeutic protocol makes the management of this tumor a real challenge.
Conflicts of interest
The authors have declared no competing interest.
Funding
Auto financing by the authors
Acknowledgements
The authors acknowledge all the members of the neonatal Intensive care unit and the department of pathology, Mohammed VI University Hospital of Marrakesh, where teamwork and expertise together benefit our patient. And the parents of the patient for their cooperation.
References
-
Minard-Colin V, Orbach D, Martelli H, Bodemer C, Oberlin O (2009) Les tumeurs mésenchymateuses du nouveau-né Soft tissue tumors in neonates. Archives de Pédiatrie 16(7): 1039-1048.
-
Duclaux-Loras R, Lachauxa A, Guibaudb L, Bertrand Y (2015) L’interferon alfa a-t-il encore des indications dans la prise en charge du syndrome de Kasabach- Merrit ?. Archives de Pédiatrie 22(5): 523-527.
-
Drolet BA, Trenor 3rd. CC, Brandao LR, Chiu YE, Chun RH, et al. (2013) Consensus-derived practice standards plan for complicated Kaposiform hemangi.oendothelioma. J Pediatr 163(1): 285-291.
-
Croteau SE, Liang MG, Kozakewich HP, Alomari AI, Fishman SJ, et al. (2013) Kaposiform- hemangioendothelioma: atypical features and risks of Kasabach- Merritt phenomenon in 107 referrals. J Pediatr 162(1): 142-147.
-
Odgaard HS, Christensen MK, Gade J (2012) [Kaposiform haemangioendothelioma in the small intestine of a three year-old boy]. Ugeskrift Laeger 174(24): 1679-1680.
-
Enjolras O, Wassef M, Mazoyer E, Frieden IJ, Rieu PN, et al. (1997) Infants with Kasabach-Merritt syndrome do not have "true" hemangiomas. J Pediatr 130(4): 631-640.
-
Lyons LL, North PE, Lai FM-M, Stoler MH, Folpe AL, et al. (2004) Kaposiform hemangioendothelioma: a study of 33 cases emphasizing its pathologic, immunophenotypic, and biologic uniqueness from juvenile hemangioma. Am J Surg Pathol 28(5): 559- 568.
-
Mahajan P, Margolin J, Iacobas L (2017) Kasabach- Merritt Phenomenon: Classic Presentation and Management Options. Clin Med Insights Blood Disorders 10: 1-5.
-
Zukerberg LR, Nickoloff BJ, Weiss SW (1993) Kaposiform hemangioendothelioma of infancy and childhood. An aggressive neoplasm associated with Kasabach-Merritt syndrome and lymphangiomatosis. Am J Surg Pathol 17(4): 321-328.
-
Le Huu AR, Jokinen CH, Ruben BP, Mihm MC, Weiss SW, et al. (2010) Expression of prox1, lymphatic endothelial nuclear transcription factor, in Kaposiform hemangioendothelioma and tufted angioma. Am J Surg Pathol 34(11): 1563-1573.
-
Richter GT, Friedman AB (2012) Hemangiomas and vascular malformations: current theory and management. Int J Pediatr Pp: 10.
-
Drolet BA, Scott LA, Esterly NB, Gosain AK (2001) Early surgical intervention in a patient with Kasabach-Merritt phenomenon. J Pediatr 138(5): 756-758.
-
Mitsuhashi N, Furuta M, Sakurai H, Takahashi T, Kato S, et al. (1997) Outcome of radiation therapy for patients with Kasabach-Merritt syndrome. Int J Radiat Oncol Biol Phys 39(2): 467-473.
-
Shin HY, Ryu KH, Ahn HS (2000) Stepwise multimodal approach in the treatment of Kasabach- Merritt syndrome. Pediatr Int 42(6): 620-624.
-
Garcia-Monaco R, Giachetti A, Peralta O, Napoli N, Lobos P, et al. (2012) Kaposiform hemangioendothelioma with Kasabach-Merritt phenomenon: successful treatment with embolization and vincristine in two newborns. J Vasc Interv Radiol 23(3): 417-422.
-
Haisley-Royster C, Enjolras O, Frieden IJ, Garzon M, Lee M, et al. (2002) Kasabach- Merritt phenomenon: a retrospective study of treatment with vincristine. J Pediatr Hematol Oncol 24(6): 459-462.
-
Deb G, Jenkner A, De Sio L, Boldrini R, Bosman C, et al. (1997) Spindle cell (Kaposiform) hemangioendothelioma with Kasabach-Merritt syndrome in an infant: successful treatment with alpha-2A interferon. Med Pediatr Oncol 28(5): 358- 361.
-
Chiu YE, Drolet BA, Blei F, Fangusaro J, Kelly ME, et al. (2012) Variable response to propranolol treatment of kaposiform hemangioendothelioma, tufted angioma, and Kasabach- Merritt phenomenon. Pediatr Blood Cancer 59(5): 934-938.
-
Ryan C, Price V, John P, Mahant S, Baruchel S, et al. (2010) Kasabach-Merritt phenomenon: a single centre experience. Eur J Haematol 84(2): 97-104.
-
Tlougan BE, Lee MT, Drolet BA, Frieden IJ, Adams DM, et al. (2013) Medical management of tumors associated with Kasabach-Merritt phenomenon: an expert survey. J Pediatr Hematol Oncol 35(8): 618- 622.
-
Adams DM, Trenor CC, Hammill AM, Vinks AA, Patel MN, et al. (2016) Efficacy and safety of sirolimus in the treatment of complicated vascular anomalies. Pediatrics 137(2): 147.
-
Fernandez-Pineda I, Lopez-Gutierrez JC, Ramirez G, Marquez C (2010) Vincristineticlopidine- aspirin: an effective therapy in children with Kasabach-Merritt phenomenon associated with vascular tumors. Pediatr Hematol Oncol 27(8): 641-645.
-
Moimeaux V, Taieb A, Legrain V, Meraud JP, Jimenez M, et al. (1992) Aspirin-ticlopidin in Kasabach-Merritt syndrome. Lancet 340(8810): 55.
-
Lopez V, Marti N, Pereda C, Martín JM, Ramón D, et al. (2009) Successful management of Kaposiform hemangioendothelioma with Kasabach-Merritt phenomenon using vincristine and ticlopidine. Pediatr Dermatol 26(3): 365-366.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?