Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?
Background: The osteopathological etiology of shock in newborn neonates is distinct and necessitates meticulous evaluation to guide targeted therapies. Timely diagnosis is essential for effective management. The prevalence of newborn septic shock in low-income nations is 26.8%, accompanied by a fatality rate of 35.4%. The research regarding the hemodynamic effects of noradrenaline in newborns is limited. Objective: This study aims to evaluate the effectiveness of noradrenaline on ventricular parameters and Vital parameters and blood gases in neonatal septic shock patients admitted to the neonatal critical care unit at Al-Azhar University hospitals. Methods: This prospective cohort study performed on 200 neonates with septic shock born in the delivery room of the Gynecology and Obstetrics Department admitted to the NICU at Al Azhar University Hospitals from September 2023 to June 2024. Parents and caregivers of neonates signed an informed consent form after explaining the advantages and possible risks of the study. The ethical committee of Al-Azhar University Hospitals approved the study protocol. Results: Neonatal characteristics distribution there were 71% patients had SGA (<10th centile), mean of birth weight ranged from 1230-3800 kg with mean of 2100.80±1740.11 kg, duration of shocked ranged from 4-12 days, with mean 7.96±6.13 days, NICU stay was ranged from 4-9 days with mean 6.82±3.10 days. Regarding the intraventricular hemorrhage among the studied neonates, most of patients had grade 1 by 20%, followed 9% had grades 3 and 7.5% had grades 2, then 2.5% only had grade 4. The mortality rate in neonates with septic shock under study was 26.5%. Regarding echocardiographic parameters, VO and FS were significantly higher at 1 hour of noradrenaline (288.30±163.9, 47.32±19.12) compared to an initiation (212.4±79.18, 29.50±14.01), (p˂0.05). MBP significantly improved after noradrenaline (37.82 ±8.22) compared to before noradrenaline (30.65 ±6.11). Conclusion: The death rate among infants with septic shock in this study was 26.5%. The administration of noradrenaline in addressing hemodynamic instability during neonatal septic shock plays a critical yet complex role in the neonatal intensive care environment. Noradrenaline significantly increases systemic vascular resistance and elevates mean arterial pressure, which is essential for preserving organ perfusion in at-risk newborns.
Mohammed Maged HEH¹, Khalifa SSM², Said Abdelfattah WAM³, Hafez MZ⁴*, Amin RH⁵, Hassan MF⁶ and El-Sayad Abd El-Hamid M²
¹Pediatric and Neonatal Department, Fujariah Hospital, UAE ²Pediatrics Department, Menoufia University, Egypt ³Pediatric Department, HMS-Algarhoud Private Hospital, UAE ⁴Physiology department, Al-Azhar University, Egypt ⁵Pediatrician Specialist, Ain Shams University, Egypt ⁶Epidemiology and preventive medicine department, Menoufia University, Egypt
Abbreviations
NICU: Newborn Intensive Care Unit; BP: Blood Pressure; EOS: Early-Onset Sepsis; LOS: Late-Onset Sepsis; MAP: Mean Arterial Pressure; PVR: Pulmonary Vascular Resistance; MBP: Mean Blood Pressure; LVO: Left Ventricular Output; RVO: Right Ventricular Output; FS: Fractional Shortening; TAPSE: Tricuspid Annular Plane Systolic Excursion; CRP: C-Reactive Protein; CBC: Complete Blood Count; ALT: Alanine Transaminase; AST: Aspartate Transaminase; BUN: Blood Urea Nitrogen; SD: Standard Deviation; IQR: Interquartile Range; UTIs: Urinary Tract Infections; PROM: Premature Rupture of Membranes.
Key massage
Neonatal sepsis is a major factor in neonatal mortality. The death rate for newborns with septic shock is 35.4% in low- and middle-income countries. The knowledge regarding the hemodynamic effects of noradrenaline in neonates is scarce.
This study intends to assess the effectiveness of noradrenaline in managing hemodynamic instability in neonatal septic shock patients admitted to the neonatal critical care unit at Al-Azhar University hospitals.
The mortality rate among infants with septic shock under examination was 26.5%.
We conclude that noradrenaline is a relatively safe and effective treatment for managing septic shock in newborns. However, further multicenter studies with larger sample sizes are necessary to corroborate our findings before it can be recommended as the primary treatment for neonatal septic shock.
Introduction
Shock is a pathophysiological condition marked by a disparity between oxygen delivery and oxygen demand in tissues, resulting in tissue hypoxia [1]. The early compensated phase is marked by neuroendocrine compensation mechanisms that enhance tissue oxygen extraction, hence sustaining blood pressure (BP) within normal ranges. Vital organs are given precedence for perfusion and oxygenation compared to non-vital organs [2].
The etiopathological etiology of shock in neonates is distinct and necessitate thorough evaluation to guide targeted interventions. Timely diagnosis is essential for effective management. Myocardial failure, aberrant peripheral vasoregulation and hypovolemia result in diminished supply of oxygen and nutrients to tissues, thereby serving as the primary causes of neonatal shock. This is typically intensified by relative adrenal insufficiency commonly observed in premature infants [3, 4].
Sepsis is a critical organ dysfunction resulting from an aberrant host reaction to infection. Neonatal sepsis is classified into early-onset sepsis (EOS) and late-onset sepsis (LOS), determined by a positive blood or cerebrospinal fluid culture collected within or beyond 3 days of age, respectively [5]. Neonates delivered before to 28 weeks before gestation or with a birth weight below 1500g have increased vulnerability to sepsis. Sepsis-related mortality rates fluctuate according to the severity of clinical symptoms, risk factors, and geographic location [6].
Newborn sepsis ranks as the third leading cause of neonatal mortality, responsible for nearly 15% of all neonatal fatalities worldwide. Sepsis is a prevalent etiology of multifactorial shock in newborns. The global incidence of baby sepsis with shock is around 1.3% of all NICU hospitalizations, along with elevated fatality rates [4, 7]. The prevalence is elevated in low-income nations, with an incidence rate of 26.8% and a death rate of 35.4%. Hypotensive preterm infants exhibit a heightened risk of morbidity, mortality, and worse neurodevelopmental outcomes [8]. Vasopressors function through several receptors to augment intracellular calcium in vascular myocytes, resulting in peripheral vasoconstriction, elevated systemic vascular resistance, and an ensuing increase in mean arterial pressure (MAP). The commonly utilized catecholamine vasopressors include norepinephrine, epinephrine, dopamine, and phenylephrine. Vasopressors operate via several receptors to elevate cytosolic calcium concentrations in vascular myocytes, resulting in vasoconstriction that enhances systemic vascular resistance and mean arterial pressure [9].
The primary care of septic shock entails swift diagnosis, hemodynamic evaluation, initiation of empirical antibiotics, fluid resuscitation, vasopressor delivery if shock continues, and hydrocortisone for refractory instances [10]. Dopamine and adrenaline have historically served as the primary vasopressor agents for managing newborn shock, with similar efficacy and safety profiles [11, 12]. Mainstay therapy for septic shock includes prompt diagnosis, hemodynamic assessment, administration of empiric antibiotics, fluid resuscitation, vasopressor support if shock persists, and hydrocortisone for refractory shock. Traditionally, dopamine and adrenaline have been used as the initial vasopressor agent for the management of neonatal shock, with comparable efficacy and safety [11, 13].
Noradrenaline activates beta 1-adrenergic and alpha- adrenergic receptors, resulting in enhanced contractility and heart rate, which subsequently elevates systemic blood pressure and coronary blood flow [14, 15, 16]. In clinical practice, alpha effects (vasoconstriction) surpass beta effects (inotropic and chronotropic effects), particularly at elevated doses [17]. Additionally, noradrenaline has a pulmonary vasodilation impact in newborns with high pulmonary vascular resistance (PVR) [7, 18]. Noradrenaline has been shown to be beneficial in the treatment of juvenile septic shock [19, 20]. The hemodynamic effects of noradrenaline in the pediatric population are well-documented, although research in newborns is limited. Enhancements in blood pressure, urine production, reduced oxygen demand following the introduction of noradrenaline, and resolution of shock in term neonates unresponsive to dopamine and dobutamine have been documented [18, 21]. The objective of our study is to evaluate the effectiveness of noradrenaline on ventricular parameters and vital parameters and blood gases in neonatal septic shock patients admitted to the neonatal critical care unit at Al-Azhar University hospitals.
Patients and Methods
Study Design and Ethics Approval
Prospective cohort research performed on 200 neonates with septic shock borned in the delivery room of the Gynecology and Obstetrics Department admitted to the NICU at Al Azhar University Hospitals from September 2023 to June 2024. Parents and caregivers of neonates signed an informed consent form after explaining the advantages and possible risks of the study. All operations were conducted in compliance with the 1964 Declaration of Helsinki and its subsequent revisions, adhering to the ethical principles established by national and institutional research committees and analogous standards. The ethical committee of Al Azhar University Hospitals approved the study protocol (IRB: RESEARCH/AZ.AST /AIP029/11/218/2/2024).
Criteria for Patient Selection
The study included both sexes septic neonates (preterm and full-term) diagnosed according to Tollner’s criteria, exhibiting clinical signs of shock, and receiving noradrenaline infusion as the initial vasoactive treatment [22]. However, we eliminated neonates with significant congenital abnormalities, those experiencing hypovolemic shock (due to blood loss or other fluid loss), hemodynamically significant patent ductus arteriosus (hsPDA), and moderate to severe hypoxia ischemic encephalopathy [23].
Diagnosis of Septic Neonates
Septic shocks are defined by systemic hypotension, indicated by a Mean Blood Pressure (MBP) falling below the 10th percentile of the normative range for birth weight and postnatal age, alongside at least three of the following criteria reflecting diminished perfusion: Tachycardia (heart rate surpassing 20 beats per minute above baseline), feeble peripheral pulses, extended capillary refill time exceeding 3 seconds, and urine output below 1 mL/kg/h.
All neonates incorporated in this study were subjected to the following: • Full History taking and Clinical Examination as: Assessment of gestational age/weeks, Assessment of birth weight utilizing electronic scale EB522, LOT. NO.CR2021/07. Cuff sizes 1 to 3 were utilized, with cuff 1 designated for arm circumferences of 1-4 cm, cuff 2 for 4-6 cm, and cuff 3 for 6-11 cm, ensuring coverage of at least two-thirds of the right upper arm length and the complete arm circumference. Maternal history (age, parity, consanguinity, birth method, maternal risk factors). Documentation of maternal and neonatal risk factors and comprehensive systematic evaluation of enrolled infants, encompassing anthropometric measurements, neurological assessment, and examinations of the chest, cardiovascular system, belly, extremities, integumentary system, and genitalia. • Echocardiographic studies were performed by cardiologist pysiation included Left ventricular systolic functions left ventricular output (LVO) and fractional shortening (FS) both in parasternal long and short axis views. • Right ventricular systolic: Right ventricular output (RVO) and tricuspid annular plane systolic excursion (TAPSE) will be assessed twice using echocardiography: once post-fluid bolus and again sixty minutes following the initiation of noradrenaline infusion. All infants were delivered a fluid bolus of 10 mL/kg of crystalloids, followed by the administration of noradrenaline at a rate of 0.2–0.5 mcg/kg/min via central or midline venous catheters. • Laboratory Investigations were done at admission and followed up: Complete blood count (CBC) with differential leukocyte count, utilizing an automated cell counter from Beckman Coulter, Inc. C-reactive protein (CRP) is deemed positive if it exceeds 6 mg/dl (utilizing CRP cobas 8000). Liver function tests were conducted using an automatic chemistry analyzer from Beckman Coulter, Inc., which comprised measurements of serum total and direct bilirubin (mg/dl), serum albumin (gm/dl), alanine transaminase (ALT), and aspartate transaminase (AST) (U/L). Kidney function assessments: (utilizing an automatic chemistry analyzer, Beckman Coulter, Inc.) comprised Blood Urea Nitrogen (BUN) (mg/dl) and Serum Creatinine concentration (mg/dl). Serum electrolytes comprised Na+, K+, and total Ca++ levels, analyzed using an automatic chemical analyzer from Beckman Coulter, Inc. Blood cultures were performed as specified.
Technique of Collection of Blood Samples
A sterile venipuncture needle was employed under stringent aseptic conditions. A tourniquet was utilized to identify a stationary vein. The skin was prepped by applying 2% tincture of iodine in expanding circles, starting from the designated puncture location. Iodine was subsequently eliminated using 70% alcohol. A vein puncture was performed, and 1-2 ml of blood was then extracted. Blood was introduced into a flask containing 50ml of nutrient-rich media to facilitate the proliferation of organisms via diphasic blood culture bottles, which must be maintained at a temperature of 8-25°C. The specimens were subsequently transferred to the laboratory, where blood culture bottles were incubated at 37°C for up to two weeks [24], and the identification of isolated organisms was conducted as follows: Microscopic analysis of a Gram-stained smear. For gram-positive bacteria: standard biochemical assays (catalase assay, cultivation on mannitol salt agar, slide coagulase assay, DNase assay, Novobiocin susceptibility assay, and CAMP assay). For gram- negative bacteria: standard biochemical assays (triple sugar iron agar, lysine iron agar, citrate utilization test, urease test, indole test, and oxidase test) and the API 20E identification system. Infants with positive culture findings were diagnosed with proven sepsis [25].
Venous blood gases (pH-PCO2-HCO3-BE) using ABL 800 and Medica easy stat devices.
Outcomes of the study
- The primary outcomes included the evaluation of shock resolution after one hour of noradrenaline infusion, the need for dose escalation, and the mortality rate, which was also assessed as a primary outcome.
- Secondary outcomes encompass the assessment of ventricular systolic function through echocardiography, the requirement for additional vasopressors, vital signs (heart rate, blood pressure), and acid-base parameters at 0 and 60 minutes, duration of ventilation, and neonatal morbidities during hospitalization, including intraventricular hemorrhage, acute kidney injury, and necrotizing enterocolitis.
Estimation of Sample Size
Sample sizes were estimated according to the cluster sample of preterm and full-term neonates with septic shock who born in the delivery room of the Gynecology and Obstetrics Department who admitted to the NICU at Al Azhar University Hospitals from September 2023 to June 2024 which were 200 neonates (128 preterm and 72 full-term).
Statistical Analysis
Statistical analysis was done by SPSS v27 (IBM©, Armonk, NY, USA). The Shapiro-Wilks test and histograms were used to evaluate the normality of the distribution of data. Quantitative parametric data were presented as mean and standard deviation (SD) and were analyzed by unpaired student t-test. Quantitative non-parametric data were presented as the median and interquartile range (IQR) and were analyzed by Mann Whitney-test. Qualitative variables were presented as frequency and percentage (%) and analyzed using the Chi-square test or Fisher’s exact test when appropriate. Kaplan–Meier survival analysis used to estimate Means and Medians for Survival Time based on duration of shock. A two-tailed P value<0.05 was considered statistically significant.
Results
A CONSORT of the study population is shown in Figure 1. 213 neonates admitted after birth to the NICU. 13 patients were excluded from the study (5 patients declined consent and 8 patients did not meet the inclusion criteria), 200 neonates with septic shock were willing to participate in the study (128 preterm and 72 full-term). In our study, the mean age of our patients was 35.65±4.69 years old, males were the most commonly frequently found in 139 (69.50%), most of them had primigravida found in 110 patients (55%), also, 137 patients (68.5%) were delivered by CS and 64 patients only by NVD (31.5%), regarding maternal risks, PROM found in 45 mother (22.5%), hypertension found in 15 patients (7.5%), DM found in 8 patients (4%), and UTI in 24 mother (12.5%) (Table 1).
The total population examined
(n=213) Excluded (n=13)
Enrolment
- Didn’t meet inclusion criteria (n=8)
- Declined to participate (n=5)
- Other reasons (n=0) Allocated (n=200) $$ \therefore \mathrm {当} x = 1 \mathrm {时} x ^ {2} + 2 x + 1 = 0 $$ Examined v Full-term received noradrenaline Allocated to intervention (n=72) Received allocated intervention (n=72) Didn’t receive allocated intervention (n=0) Preterm received noradrenaline Allocated to intervention (n=128) Received allocated intervention (n=128) Didn’t receive allocated intervention (n=0) Follow-Up Lost to follow up (n=0) Discontinued intervention Unexpected delay in diagnosis (n=0) Lost to follow up (n=0) Discontinued intervention Unexpected delay in diagnosis (n=0) $$ - 1 $$ Analysis Analyzed (n=72) Excluded from analysis (n=0) Analyzed (n=128) Excluded from analysis (n=0) Figure 1: Flowchart of the studied preterm and full-term neonates.
| Mean±SD | Range | |
|---|---|---|
| Age/year | 35.65±4.69 | 26-41 |
| No | Percentage % | |
| Primigravida | 110 | 55.00% |
| Mode of delivery | ||
| NVD | 63 | 31.50% |
| CS | 137 | 68.5 |
| Maternal risk factors | ||
| Hypertension | 15 | 7.50% |
| DM | 8 | 4.00% |
| PROM | 45 | 22.50% |
| UTI | 24 | 12% |
Table 1: Maternal characteristics distribution (n=200).
In our study, there were 71% patients had SGA (<10th centile), mean of birth weight ranged from 1230-3800 kg with mean of 2100.80±1740.11 kg, duration of shocked ranged from 4-12 days, with mean 7.96±6.13 days, NICU stay was ranged from 4-9 days with mean 6.82±3.10 days, blood culture found in 48 patients (24%). Additionally, a total of 200 cases included in this study, 152 patients (76%) had no blood culture and 48 (24%) had positive blood culture. 17 patients had positive gram, and 31 patients had negative gram, 54.84% of them had Klebsiella, and 32.26% had G+Cocci followed by 12.9% had E coli. Also, 153 patients 76.5% under mechanical ventilations, on other side, 12.5%, 4%, and 26.5% had AKI, necrotizing enterocolitis, and mortality rate, respectively (Table 2). Regarding the intraventricular hemorrhage among the studied neonates, most of patients had grade 1 by 20%, followed 9% had grades 3 and 7.5% had grades 2, then 2.5% only had grade 4 (Figure 2).
| Mean±SD | Range | |
|---|---|---|
| GA/weeks | 35.98±4.17 | 32-41 |
| SGA (<10th centile) | 142 | 71.00% |
| Gender | ||
| Male | 139 | 69.50% |
| Female | 61 | 30.50% |
| BW/kg | 2100.80±1740.11 | 1230-3800 |
| APGAR at 1 min | 5.69±1.68 | 4.54-7.81 |
| APGAR at 5 min | 7.10±2.13 | 6.10-9.03 |
| Preterm (<37 weeks) | 128 | 64.00% |
| Full-term (≥37 weeks) | 72 | 36.00% |
| Blood culture | ||
| No-growth | 152 | 76.00% |
| Growth | 48 | 24.00% |
| Gram +ve (n=17) | ||
| Staph aureus | 9 | 52.94% |
| Strep pneumonia | 5 | 29.41% |
| MRSA | 3 | 17.65% |
| Gram -ve (n=31) | ||
| G+cocci | 10 | 32.26% |
| Klebsiella | 17 | 54.84% |
| E. coli | 4 | 12.90% |
| Duration of shocked/day | 7.96±6.13 | 12-Apr |
| MV | 153 | 76.50% |
| Acute kidney injury | 25 | 12.50% |
| Necrotizing enterocolitis | 8 | 4.00% |
| NICU stay (days) | 6.82±3.10 | 4-9 |
| Hospital stays (days) | 14.22±5.14 | 17-Aug |
| Mortality rate | 53 | 26.50% |
Table 2: Neonatal characteristics distribution (n=200).
Gestational age (GA), small gestational age (SGA), birth weight (BW), mechanical ventilation (MV), neonatal intensive care (NICU).
Intraventricular hemorrhage
0.00 Grade 1 Grade 2 Grade 3 Grade 4
9.00
2.50 Figure 2: Intraventricular hemorrhage among the studied neonates.
Regarding echocardiographic parameters, VO and FS were significantly higher at 1 hour of Noradrenaline (288.30±163.9, 47.32±19.12) compared to an initiation (212.4±79.18, 29.50±14.01), (p˂0.05). While other left ventricular parameters were not significant differences between initiation and 1 hour of Noradrenaline among the studied neonates (Table 3). In this concern, VTI and VO were significantly higher at 1 hour of Noradrenaline (11.325±1.99, 329.500±145.30) compared to an initiation (9.45±3.07, 237±134.1), (p˂0.05). While other right ventricular parameters were not significant differences between initiation and 1 hour of Noradrenaline among the studied neonates (Table 4).
| Left ventricular parameters | Noradrenaline | Mean dif. | P value | |
|---|---|---|---|---|
| At initiation | 1hrs | |||
| HR | 149.3±13.8 | 153.5±20.39 | 4.19±6.59 | 0.99 |
| VTI | 9.20±1.97 | 11.0 ±2.10 | 1.8±0.13 | 0.072 |
| OCSA | 6.10±1.30 | 6.50±1.50 | 0.40±0.20 | 0.1 |
| VO | 212.4±79.18 | 288.30±163.9 | 75.90±84.72 | 0.004* |
| FS | 29.50±14.01 | 47.32±19.12 | 17.82±5.11 | 0.031* |
| Right ventricular parameters | Noradrenaline | Mean dif. | P value | |
| At initiation | 1hrs | |||
| HR | 148.30±15.41 | 152.90±18.98 | 4.60±3.57 | 0.067 |
| VTI | 9.45±3.07 | 11.325±1.99 | 1.87±1.08 | 0.047* |
| OCSA | 6.20±1.15 | 6.27±1.6 | 0.069±0.45 | 0.19 |
| VO | 237±134.1 | 329.500±145.30 | 92.50±11.20 | 0.043* |
| TAPSE | 9.09±3.08 | 9.60±1.98 | 0.51±1.10 | 0.088 |
Table 3: Left ventricular parameters among the studied neonates.
HR-Heart Rate, VO-Ventricular output, FS-Fractional Shortening, VTI-Velocity Time Integral, OCSA-Outflow cross-sectional area, *Significant Table 3: Left ventricular parameters among the studied neonates.
HR-Heart Rate, VO-Ventricular output, FS-Fractional Shortening, VTI-Velocity Time Integral, TAPSE-Tricuspid annular plane systolic excursion, OCSA-Outflow cross-sectional area. Table 4: Right ventricular parameters among the studied neonates.
As for, vital parameters and blood gases at one hour of starting noradrenaline, MBP, was significantly improved after noradrenaline (37.82±8.22) compared to before noradrenaline (30.65±6.11), by mean changes of 7.17±2.11 (23.39%), (p=0.004). However, CFT was significantly lower after noradrenaline (1.78±0.73) compared to before noradrenaline (2.22±0.42), by mean changes of 0.44±0.31 (19.82%), (p=0.012). While other parameters were not significant differences between before and after noradrenaline among the studied neonates (Table 5, Figure 3).
| Noradrenaline | P value | |||
|---|---|---|---|---|
| Before | After | Mean dif. | ||
| HR | 154.13 ±13.88 | 151.98 ±21.78 | 2.15±7.90 | 0.13 |
| MBP (mm of HG) | 30.65 ± 6.11 | 37.82 ± 8.22 | 7.17±2.11 | 0.004* |
| CFT (sec) | 2.22 ± 0.42 | 1.78 ± 0.73 | 0.44±0.31 | 0.012* |
| PH | 7.50 ± 0.09 | 7.32 ± 0.13 | 0.18±0.04 | 0.115 |
| pCO2 (mm Hg) | 37.35 ± 6.13 | 37.50 ± 4.93 | 0.15±1.20 | 0.13 |
| pO2 (mm Hg) | 69.43±5.88 | 70.14± 3.91 | 0.71±1.97 | 0.569 |
| HCO3 (mmol/L) | 18.80 ± 3.55 | 17.90 ± 3.39 | 0.90±0.16 | 0.15 |
| Base deficit (mmol/L) | -7.12±2.13 | -5.00±3.67 | 2.12±1.54 | 0.077 |
| Lactate level | 3.29±1.76 | 2.32±2.07 | 0.97±0.31 | 0.064 |
Table 4: Vital parameters and blood gases at one hour of starting noradrenaline.
Heart rate (HR), mean blood pressure (MBP), Capillary Filling Time (CFT), *significant Table 5: Vital parameters and blood gases at one hour of starting noradrenaline.
% Changes after Vs before noradrenaline Lactate level Base deficit (mmol/L) HCO3 (mmol/L)
Additionally, left ventricular parameters as VO and FS were significantly lower among preterm neonates (246.2±61.80, 36.27±17.21) more than full-term neonates (283.60±170.4, 45.32±19.12), (p˂0.05). In this concern, right ventricular parameters as VO were significantly lower among preterm neonates (254.60±147.8) more than full- term neonates (319.50±150.11), (p=0.002). While other right ventricular parameters were not significant differences between preterm and full-term neonates (Table 6).
| Studied neonates (n=200) | P value | |||
|---|---|---|---|---|
| Preterm (n=128) | Full-term (n=72) | Mean dif. | ||
| Left ventricular parameters | ||||
| HR | 150.7±12.54 | 152.8±15.33 | 2.10±0.79 | 0.753 |
| VTI | 10.65±0.99 | 11.10 ±1.149 | 0.45±0.15 | 0.085 |
| OCSA | 6.13±1.10 | 6.48±1.62 | 0.35±0.52 | 0.32 |
| VO | 246.2±61.80 | 283.60±170.4 | 37.4±8.60 | 0.013* |
| FS | 36.27±17.21 | 45.32±19.12 | 9.05±0.91 | 0.028* |
| Right ventricular parameters | ||||
| HR | 150.7±11.90 | 151.96±16.80 | 1.26±0.49 | 0.76 |
| VTI | 9.94±3.12 | 11.79±1.53 | 1.85±1.50 | 0.054 |
| OCSA | 6.15±1.30 | 6.24±1.70 | 0.09±0.04 | 0.985 |
| VO | 254.60±147.8 | 319.50±150.11 | 64.9±2.31 | 0.002* |
| TAPSE | 9.10±3.14 | 9.50±1.94 | 0.40±0.12 | 0.93 |
Table 5: Ventricular parameters among preterm and full-term neonates.
HR-Heart Rate, VO-Ventricular output, FS-Fractional Shortening, VTI-Velocity Time Integral, TAPSE-Tricuspid annular plane systolic excursion, OCSA-Outflow cross-sectional area. *significant Table 6: Ventricular parameters among preterm and full-term neonates.
Regarding the ventricular parameters in relation to mortality, left ventricular parameters as VO and FS were significantly decreased among death neonates (210.23±70.43, 26.28±10.67) more than survivor neonates (279.12±175.40, 49.55±19.88), (p˂0.05). In this trend, right ventricular parameters as VO were significantly lower among death neonates (228±133.6) more than survivor neonates (340.90±139.21), (p=0.001). While other right ventricular parameters were not significant relation with mortality among the studied neonates (Table 7).
| Studied neonates (n=200) | P value | |||
|---|---|---|---|---|
| Death (n=53) | Survivor (n=147) | Mean dif. | ||
| Left ventricular parameters | ||||
| HR | 143.65±10.51 | 148.78±21.43 | 5.13±1.92 | 0.567 |
| VTI | 10.11±0.83 | 11.4 ±3.12 | 1.29±0.29 | 0.064 |
| OCSA | 6.02±0.76 | 6.57±1.60 | 0.55±0.40 | 0.82 |
| VO | 210.23±70.43 | 279.12±175.40 | 68.89±4.97 | 0.004* |
| FS | 26.28±10.67 | 49.55±19.88 | 23.27±9.21 | 0.001* |
| Right ventricular parameters | ||||
| HR | 145.80±13.65 | 154.18±19.70 | 8.38±6.05 | 0.053 |
| VTI | 9.96±1.66 | 11.96±1.85 | 2.00±0.19 | 0.068 |
| OCSA | 6.03±1.01 | 6.50±1.80 | 0.47±0.19 | 0.499 |
| VO | 228±133.6 | 340.90±139.21 | 112.90±5.61 | 0.001* |
| TAPSE | 9.02±2.10 | 9.85±1.96 | 0.83±0.14 | 0.057 |
Table 6: Ventricular parameters in relation to mortality among the studied neonates.
HR-Heart Rate, VO-Ventricular output, FS-Fractional Shortening, VTI-Velocity Time Integral, TAPSE-Tricuspid annular plane systolic excursion, OCSA-Outflow cross-sectional area. *significant. Table 7: Ventricular parameters in relation to mortality among the studied neonates.
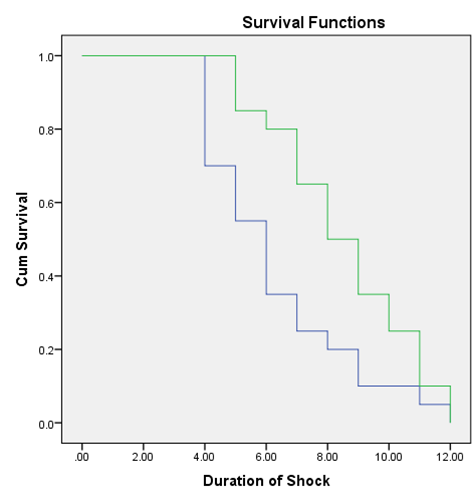
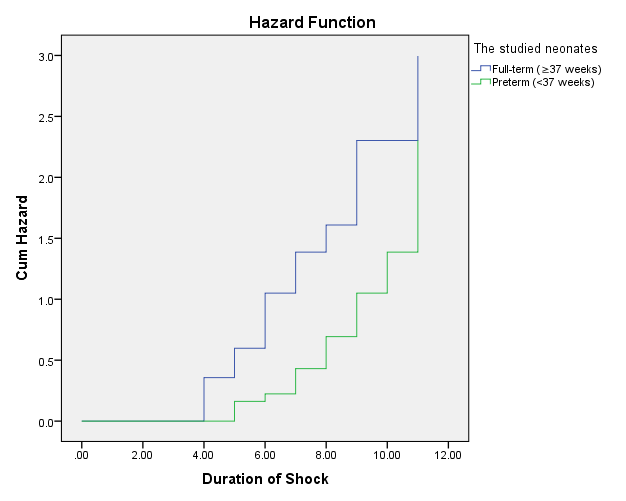
According to Kaplan–Meier survival curves, estimated median survival time was significantly higher full-term neonates with lower duration of shock (6.00, 95% CI: 4.955-7.045) as compared to preterm neonates with higher duration of shock (8.00, 95%CI: 6.539-9.461) with a significant different between them (log-rank test=5.385, P=0.02) (Table 8, Figure 4).
| Mean | Median | |||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | Std. Error | 95% CI | Estimate | Std. Error | 95% CI | |||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||||
| Full-term (≥37 weeks) | 6.3 | 0.539 | 5.245 | 7.355 | 6 | 0.533 | 4.955 | 7.045 |
| Preterm (˂37 weeks) | 8.5 | 0.51 | 7.5 | 9.5 | 8 | 0.745 | 6.539 | 9.461 |
| Overall | 7.4 | 0.406 | 6.604 | 8.196 | 7 | 0.629 | 5.767 | 8.233 |
| Chi-Square (X2) | P value | |||||||
| Log Rank (Mantel-Cox) | 5.385 | .020* | ||||||
| Breslow (Generalized Wilcoxon) | 8.289 | .004* | ||||||
| Tarone-Ware | 7.241 | .007* |
Table 7: Means and medians for survival time based on duration of shock using Kaplan–Meier survival analysis among the studied pa
Confidence Interval (CI), *Significant Table 8: Means and medians for survival time based on duration of shock using Kaplan–Meier survival analysis among the studied patients.
Discussion
Sepsis is prevalent in the newborn intensive care unit (NICU) and is linked to considerable morbidity and mortality [26]. Numerous infants with sepsis demonstrate cardiovascular instability; preterm neonates are especially susceptible due to the distinctive characteristics of their circulatory function and reserve. Cardiovascular impairment frequently results from sepsis [27]. In newborns, various hemodynamic symptoms result from unique inflammation pathways, cardiac underdevelopment, and hormonal responses. Shock is a significant syndrome marked by compromised circulation and inadequate oxygen supply to essential tissues, frequently observed in neonates within neonatal intensive care units (NICUs) [28]. Noradrenaline has been shown to be beneficial in the treatment of juvenile septic shock [19, 20]. A prospective cohort research was performed on 200 neonates with septic shock born in the delivery room of the Gynecology and Obstetrics Department admitted to the NICU at Al Azhar University Hospitals from September 2023 to June 2024, to evaluate the effectiveness of noradrenaline on ventricular parameters and vital parameters and blood gases in neonatal septic shock patients.
In this study, hypertension and diabetes mellitus emerged as the predominant maternal risk factors, with hypertension identified in 15 patients (7.5%) and diabetes mellitus in 8 patients (4%). Dirirsa, et al. reported that the incidence of premature rupture of membranes (PROM) among cases was 30.8%. In the control group, the proportion of those at significantly higher risk of developing neonatal sepsis was 3.8% (odds ratio (OR) = 7.43, 95% CI). Hamed AM, et al. identified that PROM, intrapartum fever, UTI, CS, CVL, and mechanical ventilation significantly elevated the incidence of sepsis [29]. Hornik, et al. reported that the use of mechanical ventilation on the first day was a risk factor for early sepsis, but not for late sepsis. The study identified gestational week, male gender, Apgar score at the 5th minute, and the use of prenatal steroids and antibiotics as risk factors for both early and late sepsis. Dirirsa, et al. found that neonates born to mothers with a history of urinary tract infections had a 4.7-fold increased risk of developing neonatal sepsis. The findings align with the research by Woldu, et al. in Bishoftu, Ethiopia, indicating that neonates born to mothers with a history of UTI had a threefold increased risk of developing sepsis compared to those born to mothers without such a history. Microorganisms responsible for urinary tract infections (UTIs) may be transmitted to the fetus in utero or during delivery via the birth canal, often resulting in early- onset sepsis (EOS). Bacteria such as Escherichia coli are known to cause UTIs and should be prevented.
In this study, a total of 200 cases were analyzed, of which 152 patients (76%) had no blood culture, while 48 patients (24%) had a positive blood culture. Seventeen patients tested positive for Gram staining, while thirty-one tested negatives. Among the positive cases, 54.84% were identified as Klebsiella, 32.26% as Gram-positive cocci, and 12.9% as EL- Ashry MA, et al. reported that Gram-negative cases constituted 61.1% of the total, with 54 cases confirmed by positive blood culture and 54 controls confirmed by negative blood culture [30]. Msanga DR, et al. reported that approximately 28.5% of neonates with positive blood cultures succumbed [31], in contrast to 8.6% of those with negative blood cultures. Gram-negative sepsis is associated with higher mortality rates compared to gram-positive sepsis. Increased mortality was observed in cases of sepsis caused by ESBL and MRSA isolates. A subsequent study conducted by O’Connor C, et al. analyzed 11,471 bloodstream samples revealed that Gram- negative rods were isolated from over 60% of positive blood cultures across all developing regions globally [32]. A study by Hamed AM, et al. identified gram-negative bacteria as the predominant cause of neonatal sepsis [29].
Hemodynamics dysfunction improved with elevated blood pressure, reduced heart rate, and enhanced arterial blood gas values. Preterm neonates with septic shock revealed a diminished response to norepinephrine, whereas those with prolonged pulmonary hypertension of the newborn displayed an augmented response. The current investigation demonstrated a significant rise in ventricular measures, including VO, FS, VTI, and VO, one-hour post- Noradrenaline injection compared to baseline tests. In this context, vital indicators and blood gases examined one hour after the commencement of noradrenaline demonstrated a considerable increase in mean blood pressure, with an average change of 7.17±2.11 (23.39%) compared to pre- noradrenaline values. The CFT demonstrated a significant decrease after noradrenaline injection, with a mean change of 0.44±0.31 (19.82%). A study conducted by Lu, et al. analyzed ninety-two newborns, of which 76% were premature, who received NE infusion. Norepinephrine infusion commenced after a median duration of 7 hours (IQR 2-19 hours) from the beginning of shock. The maximal norepinephrine infusion dosage in preterm infants was 0.5 (IQR 0.3-1.0) µg/kg/min, with a median duration of 45 (IQR 24.0-84.5) hours.
Hemodynamics dysfunction was mitigated by elevated blood pressure, reduced heart rate, and enhanced arterial blood gas parameters. Preterm neonates with septic shock revealed a diminished response to norepinephrine, whereas those with prolonged pulmonary hypertension of the newborn displayed an augmented response. Thirty-four neonates, or 37% of our cohort, succumbed. The timing, dosage, and duration of NE administration showed no association with infant mortality. Rizk MY, et al. discovered that initiating norepinephrine infusion enhanced hemodynamics in all preterm infants experiencing shock due to necrotizing enterocolitis or sepsis [7]. Eight hours post-NE infusion, 24 patients (80%) demonstrated normal mean blood pressure, while 27 patients (90%) showed normal urine output. No impairment of respiratory function was noted following the initiation of NE infusion, which correlated with an increase in urine output and a reduction in FiO2 requirements. The findings align with those of the prospective study conducted by Tourneux P, et al., which involved full-term infants experiencing refractory septic shock. The study indicated that norepinephrine enhanced heart performance and tissue perfusion [18]. Kallimath A, et al. demonstrates that noradrenaline enhances heart function and is a safe intervention for neonatal septic shock [33]. Nonetheless, this requires validation with a more extensive sample size. This research illustrates the efficacy of noradrenaline as a primary inotropic drug in neonatal septic shock. Since 2017, the ACCM standards advocate for dopamine or adrenaline as the primary pharmacological treatments for managing baby septic shock [34].
Conversely, accumulating evidence indicates that noradrenaline may function as an optimal inotrope in the treatment of septic shock, acting both as an inotropic drug and reducing pulmonary vascular resistance as necessary in warm shock. Tournex P, et al. conducted a prospective observational study including 22 neonates [18], revealing that noradrenaline significantly elevated systolic blood pressure, enhanced urine output, and reduced blood lactate levels. Gupta S, et al. documented similar results in a retrospective cohort study of 53 newborns [21]. Furthermore, animal investigations have shown that noradrenaline elicits a pulmonary vasodilatory response [35, 36]. It has demonstrated a pulmonary vasodilatory impact, enhanced oxygenation and decreasing the fractional inspired oxygen (FIO2) requirement in newborns [7, 18].
Noradrenaline’s pharmacological properties render it an optimal inotropic drug for neonatal shock, particularly in infants exhibiting vasodilation, elevated pulmonary vascular resistance (PVR), or pulmonary hypertension [37]. Noradrenaline elevates systemic blood pressure, enhances cardiac output, optimizes oxygen supply and use, and augments regional blood flow, particularly in the mesenteric and renal circulations, thereby enhancing survival [38]. Our results align with existing research regarding the impact of noradrenaline in newborns. Consistent with the research conducted by Tourneux P, et al. and Gupta S, et al. on neonatal shock, a retrospective investigation by Rizk MY, et al. involving preterm neonates with refractory septic shock demonstrated a significant elevation in MBP [7, 18, 21]. The data support our analysis, demonstrating a favorable response to noradrenaline in elevating mean blood pressure and decreasing the need for additional inotropes. Neonates in our study had a fast elevation in blood pressure, signifying a robust reaction within one hour of commencing noradrenaline treatment. The reaction transpired more swiftly than in the studies conducted by Torunex P, et al., Rizk MY, et al., and Gupta S, et al., which documented reactions at 3 hours, 8 hours, and 6 hours following noradrenaline injection, respectively [7, 18, 21].
The Kaplan–Meier survival curves indicate that the expected median survival time was considerably greater for full-term babies with shorter shock durations compared to preterm neonates with longer shock durations, underscoring a substantial difference between the two groups. The mortality rate in this trial was 26.5%, consistent with the range described by Kallimath et al. six neonates (28.6%) succumbed. This exceeded the mortality rates of 18% and 16% reported by Torunex P, et al. and Gupta S, et al., respectively [18, 21]. The findings exceed the percentage indicated by Rizk MY, et al., who observed that two (7%) individuals succumbed to septic shock, in contrast to the previously recorded 10.3% mortality rate in neonates with sepsis and organ failure [7]. The effectiveness of norepinephrine in enhancing survival rates in newborns with refractory septic shock remains uncertain. They conclude that NE may be advantageous in mitigating stress during the newborn period. The medication seems to be well tolerated; nevertheless, additional prospective studies with sufficient hemodynamic evaluation are required to ascertain the safety of NE in the preterm demographic. Lu, et al. demonstrated that NE significantly enhances clinical indices in both preterm and full-term neonates. It must be determined whether norepinephrine therapy can enhance survival rates compared to other vasoactive agents in preterm neonates. Previous research indicated that the mortality rate of premature newborns treated with NE was elevated (33%- 48%), which is lower than the 41% mortality reported by Lu, et al. The increased mortality noted in these studies is attributable to the selection of subjects exhibiting greater disease severity (ineffectiveness of standard treatment) and various confounding factors, including indicators of inadequate prenatal care (reduced prenatal steroid administration) and a higher incidence of morbidities (IVH and NEC) relative to the general preterm neonate population in China [39]. While NE shown comparable efficacy in enhancing clinical parameters in both preterm and full- term newborns, the tendency suggested that NE may be less beneficial in premature infants with septic shock, but it appears more helpful in those with PPHN. This trend indicates that etiology-specific interventions for preterm neonates in shock are likely crucial; however, further validation is necessary, as prior studies have demonstrated inconsistent effects of NE on ventilation parameters in preterm neonates with septic shock [18, 21].
Limitation of the Study
The current study had several limitations, including its conduct at a single center with a small patient sample size. Additionally, it relied on non-invasive blood pressure recordings, using a threshold of less than the 10th percentile for the definition of shock. Therefore, multicenter studies involving a substantial number of patients across diverse geographic regions are necessary [40, 41, 42, 43].
Conclusion
Neonatal sepsis is a significant cause of neonatal mortality. The mortality rate for neonates experiencing septic shock in this study was 26.5%. The administration of noradrenaline for managing hemodynamic instability in neonatal septic shock is essential but intricate within the neonatal intensive care setting. Noradrenaline markedly enhances systemic vascular resistance and raises mean arterial pressure, which is crucial for maintaining organ perfusion in vulnerable neonates. However, its use requires careful monitoring due to potential adverse effects, including altered heart rate and peripheral perfusion.
Declarations
Consent for publication: all authors have read and revised well for the manuscript and agree to publish.
Availability of data and material: Not applicable Competing interests: There is no conflict of interest.
Funding: The author received no financial support for this article’s research, authorship, and publication.
Authors’ contributions: Conceptualization: MZ Hafez, WA Abdelfattah, HE Maged, RH Amin; Methodology: SS Khalifa, MF Hassan; Software: MZ Hafez, RH Amin, MA Abd El- Hamid; Data curation: MZ Hafez, SS Khalifa, Validation: MZ Hafez, WA Abdelfattah, HE Maged, MF Hassan; Supervision: MZ Hafez, WA Abdelfattah, HE Maged; Visualization: RH Amin, MF Hassan, MA Abd El-Hamid; Writing- Original draft preparation: MZ Hafez, WA Abdelfattah, HE Maged, RH Amin, MF Hassan, SS Khalifa; Reviewing and Editing: MZ Hafez, WA Abdelfattah, HE Maged, RH Amin, MA Abd El- Hamid, SS Khalifa, MF Hassan. All authors read and approved the final manuscript.
Acknowledgments: Not applicable
Authors’ information (optional): Not applicable.
References
-
Blumlein D, Griffiths I (2022) Shock: aetiology, pathophysiology and management. Br J Nurs 31(8): 422- 438.
-
Elsayed Y, Abdul Wahab MG (2022) A new physiologic- based integrated algorithm in the management of neonatal hemodynamic instability. Eur J Pediatr 181(3): 1277-1291.
-
Nagpal R, Suryawanshi P (2020) Role of Point-of- care Ultrasound Imaging in Neonatal Sepsis. Pediatric Infectious Disease 2(3): 89-98.
-
Nates JL, Pene F, Darmon M, Mokart D, Castro P, et al. (2024) Septic shock in the immunocompromised cancer patient: a narrative review. Crit Care 28(1): 285.
-
Gopal N, Chauhan N, Jain U, Dass SK, Sharma HS, et al. (2023) Advancement in biomarker based effective diagnosis of neonatal sepsis. Artificial Cells, Nanomedicine, and Biotechnology 51(1): 476-490.
-
Spaggiari V, Passini E, Crestani S, Roversi MF, Bedetti L, et al. (2022) Neonatal septic shock, a focus on first line interventions. Acta Biomed 93(3): e2022141.
-
Rizk MY, Lapointe A, Lefebvre F, Barrington KJ (2018) Norepinephrine infusion improves haemodynamics in preterm infants during septic shock. Acta Paediatr 107(3): 408-413.
-
Mannan MA, Jahan MA, Hossain MA, Shuma AI, Moni SC, et al. (2022) Septic Shock in Neonate: Clinical Profile and its Outcome. Journal of Pediatrics, Perinatology and Child Health 6(1): 171-187.
-
Shankar A, Gurumurthy G, Sridharan L, Gupta D, Nicholson WJ, et al. (2022) A clinical update on vasoactive medication in the management of cardiogenic shock. Clin Med Insights Cardiol 2022 16: 11795468221075064.
-
Ahlstedt C, Sivapalan P, Kriz M, Jacobson G, Meyhoff TS, et al. (2024) Effects of restrictive fluid therapy on the time to resolution of hyperlactatemia in ICU patients with septic shock. A secondary post hoc analysis of the CLASSIC randomized trial. Intensive Care Med 50(5): 678-686.
-
Baske K, Saini SS, Dutta S, Sundaram V (2018) Epinephrine versus dopamine in neonatal septic shock: a double-blind randomized controlled trial. Eur J Pediatr 177(9): 1335-1342.
-
Coloretti I, Genovese A, Teixeira JP, Cherian A, Ferrer RR, et al. (2024) Angiotensin ii therapy in refractory septic shock: which patient can benefit most? A narrative review. J Anesth Analg Crit Care 4(1): 13.
-
Valverde E, Pellicer A, Madero R, Elorza D, Quero J, et al. (2006) Dopamine versus epinephrine for cardiovascular support in low-birth-weight infants: analysis of systemic effects and neonatal clinical outcomes. Pediatrics 117(6): e1213-e1222.
-
Gorain B, Dutta S, Nandy U, Sengupta P, Choudhury H (2020) Pharmacology of Adrenaline, Noradrenaline, and Their Receptors. Frontiers in Pharmacology of Neurotransmitters, Springer, Singapore, pp: 107-142.
-
Lechsner P, Ban EG (2022) Alpha adrenergic receptors in clinical practice–Present and future. Acta Marisiensis- Seria Medica 68(4): 145-149.
-
Trivino CAS, Clavijo AH, Velandia KYG, Pifferi S, Menini A (2024) Noradrenaline modulates sensory information in mouse vomeronasal sensory neurons. IScience 27(10): 110872.
-
Seri I (2001) Circulatory support of sick preterm infants. Semin Neonatol 6(1): 85-95.
-
Tourneux P, Rakza T, Abazine A, Krim G, Strome L (2008) Noradrenaline for management of septic shock refractory to fluid loading and dopamine or dobutamine in full-term newborn infants. Acta Paediatr 97(2):177- 180.
-
Lampin ME, Rousseaux J, Botte A, Sadik A, Cremer R, et al. (2012) Noradrenaline use for septic shock in children: doses, routes of administration and complications. Acta Paediatr 101(9): e426-e430.
-
Deep A, Goonasekera CD, Wang Y, Brierley J (2013) Evolution of haemodynamics and outcome of fluid- refractory septic shock in children. Intensive Care Med 39(9): 1602-1609.
-
Gupta S, Agrawal G, Thakur S, Gupta A, Wazir S (2022) The effect of norepinephrine on clinical and hemodynamic parameters in neonates with shock: a retrospective cohort study. European Journal of Pediatrics 181(6): 2379-2387.
-
Tollner U (1982) Early diagnosis of septicemia in the newborn: clinical studies and sepsis score. Eur J Pediatr 138(4): 331-337.
-
Jain A, Shah PS (2015) Diagnosis, evaluation, and management of patent ductus arteriosus in preterm neonates. JAMA Pediatrics 169(9): 863-872.
-
Kwon-Chung KJ, Boekhout T, Fell JW, Diaz M (2002) (1557) Proposal to conserve the name Cryptococcus gattii against C. hondurianus and C. bacillisporus (Basidiomycota, Hymenomycetes, Tremellomycetidae). Taxon 51(4): 804-806.
-
El Awady MY, Abd El Rahman AT, Al Bagoury LS, Mossad IM (2014) Air quality in Ain shams university surgery hospital. J Egypt Soc Parasitol 44(3): 749-759.
-
Shane AL, Sanchez PJ, Stoll BJ (2017) Neonatal sepsis. Lancet 390(10104): 1770-1780.
-
Kharrat A, Jain A (2022) Hemodynamic dysfunction in neonatal sepsis. Pediatr Res 91: 413-424.
-
Schwarz CE, Dempsey EM (2020) Management of neonatal hypotension and shock. Semin Fetal Neonatal Med 25(5): 101121.
-
Hamed AM, Ibrahim MF, Abdel-Alim MA (2020) Evaluation of various risk factors in neonatal sepsis. The Egyptian Journal of Hospital Medicine 81(2): 1449-1456.
-
EL-Ashry MA, Saleh GA, Hosny YR, Mohammed N (2022) Mean platelet volume (MPV) and plasma lactate level in the diagnosis and prognosis of neonatal bacteremia. Microbes and Infectious Diseases 3(1): 92-100.
-
Msanga DR, Parpia F, Konje ET, Hokororo A, Mshana SE (2021) High Mortality among Premature Neonates with Positive Blood Culture Neonatal Sepsis in a Tertiary Hospital, Tanzania: A Call for Action. Children 8(11): 1037.
-
O’Connor C, Joffe H (2020) Intercoder reliability in qualitative research: debates and practical guidelines. International journal of qualitative methods 19: 2020.
-
Kallimath A, Garegrat R, Patnaik S, Singh Y, Soni NB, et al. (2024) Hemodynamic effects of noradrenaline in neonatal septic shock: a prospective cohort study. Journal of Tropical Pediatrics 70(2): fmae001.
-
Davis AL, Carcillo JA, Aneja RK, Deymann AJ, Lin JC, et al. (2017) American College of Critical Care Medicine Clinical Practice Parameters for Hemodynamic Support of Pediatric and Neonatal Septic Shock. Crit Care Med 45(6): 1061-1093.
-
Tulloh RM, Dyamenahalli U, Smith KS, Haworth SG (1994) Adrenoceptor-stimulated endothelium- dependent relaxation in porcine intrapulmonary arteries. Pulm Pharmacol 7(5): 299-303.
-
Jaillard S, Elbaz F, Bresson-Just S, Riou Y, Houin- Debarge V, et al. (2004) Pulmonary vasodilator effects of norepinephrine during the development of chronic pulmonary hypertension in neonatal lambs. Br J Anaesth 93(6): 818-824.
-
Beale RJ, Hollenberg SM, Vincent JL, Parrillo JE (2004) Vasopressor and inotropic support in septic shock: an evidence-based review. Crit Care Med 32: S455-S465.
-
Giantomasso DD, Morimatsu H, May CN, Bellomo R (2003) Intrarenal blood flow distribution in hyperdynamic septic shock: Effect of norepinephrine. Crit Care Med 31(10): 2509-2513.
-
Cao Y, Jiang S, Sun J, Hei M, Wang L, et al. (2021) Assessment of neonatal intensive care unit practices, morbidity, and mortality among very preterm infants in China. JAMA Netw Open 4(8): e2118904.
-
Aneja R, Carcillo J (2011) Differences between adult and pediatric septic shock. Minerva Anestesiol 77(10): 986- 992.
-
Brierley J, Carcillo JA, Choong K, Cornell T, Decaen A, et al. (2009) Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine. Crit Care Med 37(2): 666-688.
-
De Backer D, Biston P, Devriendt J, Madl C, Chochrad D, et al. (2010) Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med 362(9): 779-789.
-
Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, et al. (2008) Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med 2008; 34(1): 17-60.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Occurrence of Third root (supernumerary / Radix Entomolaris / Radix Paramolaris) in the Primary Mandibular Molars - A Systematic Review