Anaesthetic Concerns of an Anterior Mediastinal Mass
Managing a child with anterior mediastinal mass is considered as one of the most challenging cases ever encountered by an anesthetist. The main concerns are not only related to managing the airway and maintaining ventilation with the most suitable mode, but also the associated cardiovascular complications, where the patient is at risk of cardiorespiratory embarrassment before, during and after induction of anaesthesia. Furthermore, managing children during anaesthesia produces an array of implications, hence thorough preoperative assessment is essential to ensure that the children are safely induced with the general anesthetic drugs, the airway is securely protected and the anxious parents are given ample explanations and are comforted. A case report of an unfortunate boy who required an elective intubation prior to investigations to establish his diagnosis is presented. The aim emphasizes on highlighting our main concerns and strategies pre, during & post induction of anaesthesia from an anaesthetist’s point of view.
Zainal Abidin H*, Ali S, Hassan MH, Chong SE and Mazlan MZ
Malaysia
9398443; Email: hudaz82@gmail.com
strategies pre, during & post induction of anaesthesia from an anaesthetist’s point of view.
Keywords: Anterior mediastinal mass; General anaesthesia; Paediatric
Case Report
A five-year-old boy, the second child raised by a single parent was presented for the first time to our hospital with complaints of on and off low grade fever, cough and neck swelling for one week duration. His mother described the cough as non-productive but worsening over the period of 1 week associated with shortness of breath. Besides this, the neck swelling progressed rapidly causing dysphagia.
On physical examination, vital signs were stable, he was able to complete sentences with hoarseness of voice however there was no stridor heard. There was also facial congestion with dilated veins over the anterior chest area suggesting superior vena cava compression. Variable sizes of cervical lymph nodes palpated. The abdomen was soft with hepatosplenomegaly. The impression made by the primary team was possible lymphoma with evidence of superior vena cava obstruction. The boy was advised to be admitted to the paediatric oncology ward ensuring his condition did not deteriorate further; meanwhile a thorough checkup was performed to ascertain the diagnosis and the most suitable treatment to be administered.
Chest X-ray revealed obvious huge anterior mediastinal mass and left pleural effusion. Bone marrow aspiration showed an increase in eosinophilic precursors and monocytosis. Definitive diagnosis could not be made at that particular time possibly due to inadequate samples (Figure 1).
(CXR film attached)
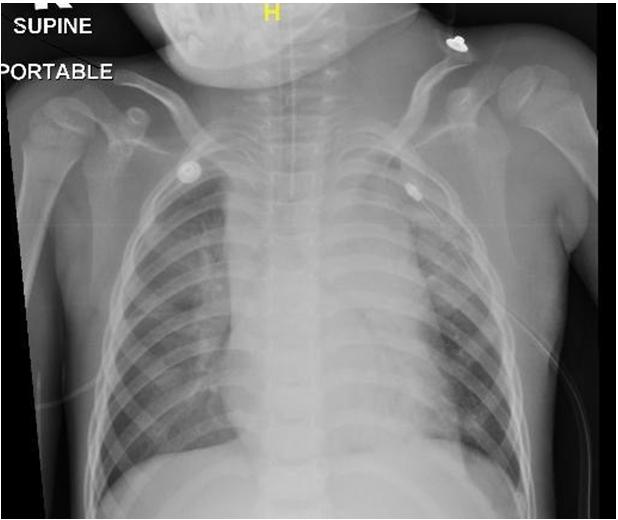
Figure 1: CXR taken on the day of admission. Two days after admission, the patient was referred for an elective intubation to enable the child to proceed with the CT scan and lymph nodes biopsy. After a multidisciplinary discussion, agreed consensus was made that the child should be intubated and ventilated in a controlled environment where difficult airway adjuncts are easily available and varying modes of ventilator settings could be offered.
Explanation and reassurance was given to the accompanying mother, the child was put under general anaesthesia whereby gas induction which consisted of 100% oxygen and titrated 8% Sevoflurane delivered vigilantly. Intravenous fentanyl 20mcg was given to the readily inserted intravenous cannula at the right foot.
Spontaneous breathing was maintained soon after the child was deeply anaesthetized and neither induction agent nor muscle relaxant was given during that time. The child was then intubated with size 5.0 endotracheal tube anchored at 15cm. A few seconds after intubation, the SpO2 reading dropped significantly to 84% but picked up slowly with positive pressure ventilation using t-piece, with application of positive end expiratory pressure (PEEP). On auscultation, there was reduced in air entry on the left lung and occasional rhonchi detected. Thick copious mucoid secretion was noted upon suctioning through the endotracheal tube. A conventional ventilator was connected with the setting of FiO2: 1.0, PI: 24, Psupp: 10, PEEP: 4, and generated tidal volume was around 200- 250mls. The child was then sedated with intravenous propofol running at 50mg/hr and intravenous fentanyl 10mcg/hr.
Subsequently, a lung scan was conducted at the bedside which revealed massive pleural effusion on the left lung and minimal pleural effusion on the right lung. A chest drain was inserted at the left safety triangle draining about 450 mls serous fluid followed by 20mls per kg ringer’s lactate and 250mls of 5% albumin as replacement. The child was then transported safely and stabilized at the pediatric oncology ward. After discussions between pediatric oncologists and based on investigations done, the patient was treated as non- Hodgkin lymphoma & CHOPP protocol was initiated.
Discussion
For this particular patient, our anaesthetic concerns are mainly on the airway management and subsequent ventilation strategies, bearing in mind the possible complications that might arise as a result of an anterior mediastinal mass. On top of that, the presence of significant bilateral pleural effusion which required chest drainage upon induction of general anaesthesia possesses a significant risk. Approaching paediatric patients will never be the same as managing adult patients going for general anaesthesia. Various imperative points need to be stressed on not only pertaining to the child but also to the anxiously accompanied parents. As a rule of thumb, before subjecting patients to general anaesthesia, they should be thoroughly evaluated and investigated.
The mediastinum is described as an area between two pleural cavities where the superior border consists of the thoracic inlet and the diaphragm as the inferior border. By imagining the sagital cross sectional area of the thorax, the inferior border is further divided by three other compartments namely; anterior compartment which is the space between the sternum and the anterior border of the pericardium, the middle mediastinum which contains the heart, its pericardium, and other vital structures such as the trachea, carina and the two main bronchi. Where else, the posterior mediastinum is the area between the posterior border of the heart and the vertebrae [1].
Among the causative diseases contributing to an anterior mediastinal mass includes lymphoma, thymoma, germ cell tumors, metastatic lesion, bronchogenic tumors and thyroid, in descending frequency order [2].
Despite all currently available investigations, getting to know the classical symptoms and signs upon presentation is crucial to give us a general idea of the current condition of the patient. However, there were cases reported of a few patients presented with a large anterior mediastinal mass with apparently no obvious signs and symptoms. These kinds of patients will usually develop catastrophic events intraoperatively with an obstructed airway. This is possibly due to aggressiveness and a slow growing tumor. In our patient, the airway compression symptoms appeared early because of the relatively smaller airway caliber compared to an adult.
The symptoms may vary depending on the severity of intrathoracic compression. From the acute presentation and evidence of compression of vital structures such as superior vena cava syndrome, dyspnoea and hoarseness of voice, we would say that this patient easily fell under the high risk group for general anesthesia. The presence of pleural effusions from the CXR may further predispose the patient to perioperative complications. In our patient, we could not ascertain the degree of airway obstruction since there was no CT scan or lung function test done. We presumed that this might be due to concerns of the child’s cooperation during the procedure.
It is vital to determine the best or optimal position where the symptoms are minimized. This is correlated well with the size and the exact position of the mass. As this will later contribute to what is described as the ‘rescue position’ upon failure of ventilation under general anaesthesia. The rescue positions may vary from lateral, upright seated and even prone position [3]. This is related to the anatomic variation of the mass and the airway. This is again best determined by a CT scan report of individual patients.
As a measure to reduce the unwanted complications of an anterior mediastinal mass upon delivering general anaesthetics, preoperative radio or chemotherapy and even corticosteroid therapy have been advocated. This is believed to reduce the tumor size and thus encroachment of the airway [3] however this may give an impact on diagnostic histological accuracy.
Numerous strategies described on anaesthetic management of patients presented with an anterior mediastinal mass. Ideally, where general anaesthesia can be avoided, for instance for the purpose of lymph nodes biopsy, the local anaesthetic or regional anaesthesia technique is preferred [4]. The use of ketamine as a sedative agent added with antisialogogue drug to decrease salivation has been described. Among the favoured advantages include maintenance of spontaneous ventilation and preservation of airway reflexes. Besides, ketamine can help ameliorate the signs and maintain haemodynamic stability in patients with evidence of cardiovascular compression with its sympathomimetic properties [5].
Other alternative includes the use of dexmedetomidine as a sedative agent. Although it is an agent which is seldomly used for paediatric population, it contributes to only modest cardio respiratory compromise in patients with an anterior mediastinal mass in both adult and a paediatric group of age. A case series reported of successful use of bolus of dexmedetomidine up to 0.5mcg/kg over 5 minutes or an infusion of up to 0.7mcg/kg/hr in conjunction with other sedative agents to the paediatric population. The fact that it is a selective alpha 2 agonist with combination of sedation and analgesic properties makes the wide usefulness of the agent to many anaesthetic procedures [6].
One of the methods suggested on approaching the airway is with awake fibre optic intubation followed by appropriately sized reinforced endotracheal tube. The use of rigid bronchoscope may be life saving especially in the situation where the distal carina or bronchi are compressed and it is not possible to advance the endotracheal tube beyond the site of obstruction. With application of this method, the use of jet ventilation would be beneficial.
Most literature emphasises on the maintenance of spontaneous ventilation to preserve normal transpulmonary pressure gradient and improves flow to the conducting airway. This can either be via inhalational induction or titrated doses of intravenous induction agents. The use of muscle relaxants is not recommended as it can cause hazardous airway obstruction.
Nevertheless, even by using what is described as the most preferable and safest techniques, there were still adverse events reported especially with patients with >50% compression of cross sectional areas of the trachea (TCA). Other than CT scan findings, peak expiratory flow rate (PEFR) value of less than 50% may also indicate significant airway compression [7].
Interestingly, the use of helium-oxygen mixture has been described for symptomatic relief, facilitates induction and weaning from mechanical ventilation. It is basically used to decrease airway resistance and promotes laminar flow [8].
For high risk patients, it is advisable to have a cardiopulmonary bypass machine available beforehand, for instance in an unexpected airway collapse during general anaesthesia, the use of extracorporeal membrane oxygenation (ECMO) and emergency percutaneous cardiopulmonary bypass support can be applied. Although there were several cases reported of successful use of CBP on managing cardiorespiratory embarrassment, there was also conflicting opinion where the time taken for preparations including cannulation and institution of CPB was argued and believed that it may have cause considerable neurological damage to the patients [9].
General anesthesia induction for a restless child is prone to complications like bronchospasm, airway collapse, and cardiovascular compromise thus careful assessment and anaesthetic plans should be individualized for each patient requiring general anaesthesia.
References
-
Soliman LM, Mossad EB (2006) Thoracic epidural catheter in the management of a child with an anterior mediastinal mass: a case report and literature review. Pediatr Anesth 16(2): 200-205.
-
Gardner JC, Royster RL (2011) Airway collapse with an anterior mediastinal mass despite spontaneous ventilation in an adult. Anesth Analg 113(2): 239-242.
-
Ricketts RR (2001) Clinical management of anterior mediastinal tumors in children. Paper presented at the Seminars in pediatric surgery.
-
Gothard JW (2008) Anesthetic considerations for patients with anterior mediastinal masses. Anesthesiol clin 26(2): 305-314.
-
Frawley G, Low J, Brown T (1995) Anaesthesia for an anterior mediastinal mass with ketamine and midazolam infusion. Anaesth Intensive Care 23(5): 610-612.
-
Carollo DS, Pestieau S, Bosco R (2013) Dexmedetomidine for anterior mediastinal mass computed tomography-guided biopsy: a case series. Ochsner J 13(4): 541-543.
-
Perger L, Lee EY, Shamberger RC (2008) Management of children and adolescents with a critical airway due to compression by an anterior mediastinal mass. J Pediatr Surg 43(11): 1990-1997.
-
Galway U, Doyle DJ, Gildea T (2009) Anesthesia for endoscopic palliative management of a patient with a large anterior mediastinal mass. J Clin Anesth 21(2): 150-151.
-
Hammer GB (2004) Anaesthetic management for the child with a mediastinal mass. Pediatr Anesth 14(1): 95-97. `
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?