Use of Intraventricular Vancomycin in Neonatal Meningitis Dueto Elizabethkingilla Meningoseptica
Elizabethkingia meningoseptica is a non-motile, catalase positive, oxidase positive, non-glucose fermenting, gram negative bacilli which is resistant to common drugs active against gram negative organism. It presents as neonatal meningitis mostly in preterms as they have low immunity. Antibiotics which have shown effectiveness against this organism includes cefepime, tazobactam, piperacillin, cotrimoxazole, tigecycline, minocycline, quinolones and drugs active against gram positive bacteria such as vancomycin and rifampicin. Intraventricular therapy use has been limited owing to drug toxic effect. Seizures, hearing loss and chemical ventriculitis had been reported mostly as short term side effect. Long term side effect needs more follow up studies. Here we report a preterm newborn having E.meningoseptica ventriculitis showing improvement with intraventricular vancomycin without any short term adverse effect in first 6 months of life.
Introduction
Elizabethkingia meningoseptica is non-motile, catalase positive, oxidase positive, non-glucose fermenting, gram negative bacilli which formerly has been known by name of Chryseobacterium meningosepticum until 2005 and Flavobacterium meningosepticum until 1994 [1, 2]. As per Centers for Disease Control and Prevention (CDC) classification, it has been categorized into group II an unclassified bacteria. It has been name after, Elizabeth O King an American bacteriologist, who isolated it in 1959 in an infant suffering from meningitis [3]. Elizabethkingia meningoseptica is an ubiquitous Gram negative bacillus which colonizes the hospital environment including sinks, water tanks, incubators, beds, saline solutions, syringes, feeding tubes, ventilator tubings, humidifiers among many other sites [3]. It presents as meningitis in neonates specially preterms who are immunocompromised [4]. It is resistant to most antimicrobials used for empirical therapy in neonatal sepsis/meningitis including beta lactams, carbapenems and aminoglycosides [5]. Neonatal mortality has been reported in nearly one third of patients and nearly one third of survivors had sequelae and deficits [4].
Here we report a case of Elizabeth kingella meningoseptica causing neonatal meningitis in preterm neonate not responding to intravenous drugs as per blood culture and sensitivity, but responded well to intraventricular vancomycin.
Preterm 30 weeks 5 days gestation male baby was born to a gravida 2 para 1 mother with 1 live child, with birth weight of 1.266 Kg. Baby was delivered by LSCS, done in view of uncontrolled PIH with non-progression of labour. Baby cried soon after birth. As oxygen saturation was between 84-90% so baby was put on nasal CPAP ventilation in NICU. Chest X Ray done was suggestive of RDS, surfactant was administered. CPAP was weaned off by day 7 of life. Initially baby was kept NPO and IV fluid was started. Minimal OG feed and TPN was started on day 2 of life but baby could not tolerated OG feed, so pediatric surgeon opinion was taken and advised to do XRay abdomen erect and gastrographin study, which was suggestive of malrotation of intestine. Hence baby was operated for same on day 5 of life. Sepsis screen done on day 2 of life was positive, so inj cefotaxime and inj amikacin were started. Inj Metronidazole was added post- surgery for malrotation on day 6 of life. On repeated sepsis screens CRP was increasing so on day 9 of life cefotaxime was stopped and inj Piperacillin Tazobactam added which was further upgraded next day due to continuous increase in sickness. So baby was started on Meropenem and Amikacin in anti meningitic dose. Blood culture and ET culture showed growth of Elizabethkingia meningoseptica which was sensitive to vancomycin, so vancomycin was added on day 12 of life. Repeat Blood culture was also sent and again the same organism grown so meropenem was stopped as was resistant. Rifampicin and cefepime+tazobactum (antimeningitic dose) was added as per senstivity. LP was done which was suggestive of meningitis and culture also showed the growth of the same organism, which was resistant to vancomycin and rifampicin. So vancomycin and Rifampicin were stopped and linezolid was added. After that, repeated lumber punctures showed meningitis and culture also showed same organism sensitive to cefepime+tazobactam, linezolid. CSF culture on 19th day was also sensitive to Rifampicin so Rifampicin was again added on day 32 of life. As CSF was continuously growing same organism despite 18 days of sensitive antibiotics in adequate doses so 10 mg vancomycin was added intraventricularly although was not sensitive but was used in literature with similar setting. After 18 days of vancomycin intraventricularly, CSF culture was negative and grams stain became negative for organism. Thereafter intraventricular vancomycin was stopped after 21 days.
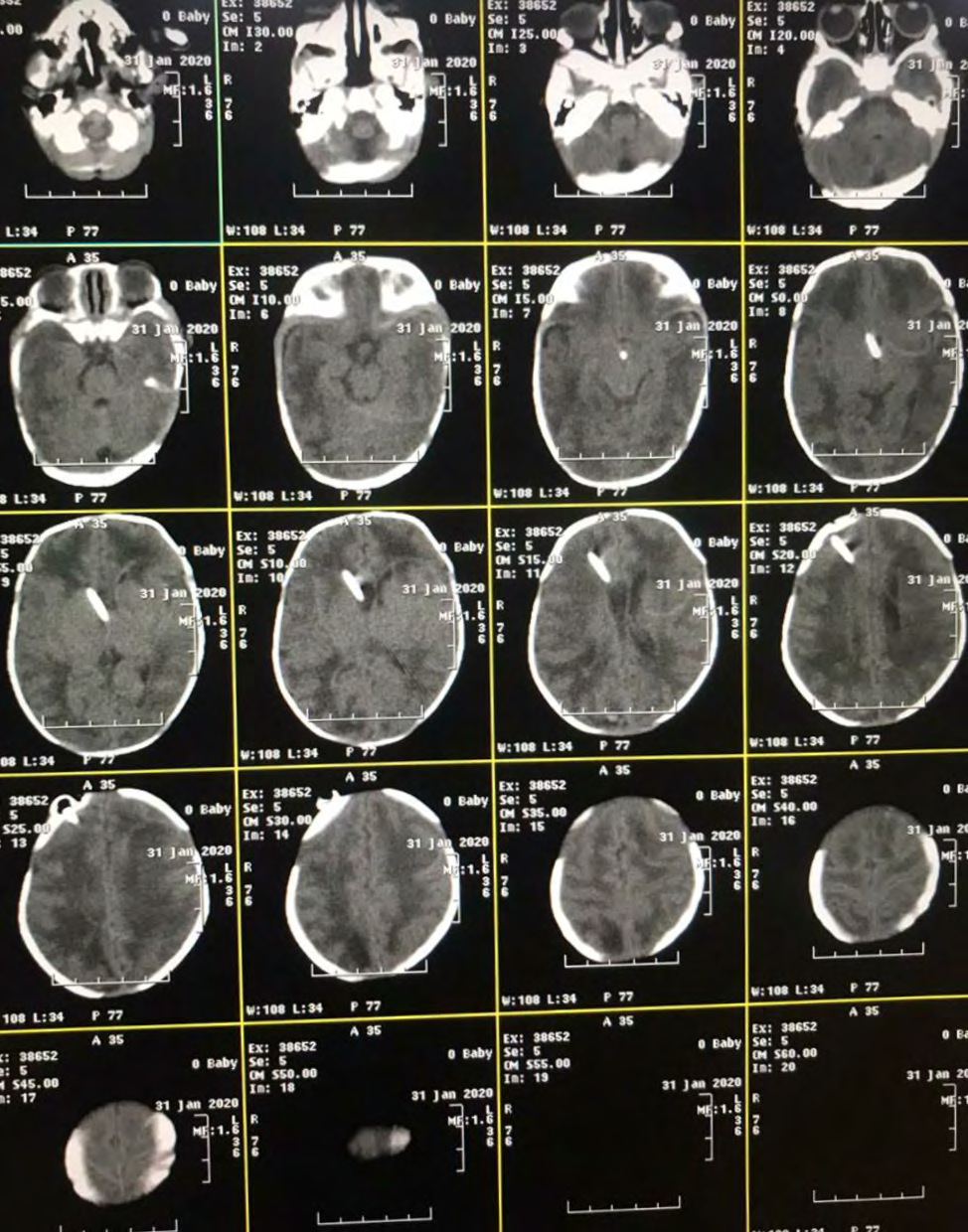
USG cranium after diagnosis of meningitis showed ventriculomegaly. MRI was done which showed ventricular enlargement with leptomeningeal enhancement suggestive of meningitis. Neurosurgery opinion was taken and advised to continue conservative treatment initially but in view of increasing ventricular size right sided external ventricular drainage was done on day 38 of life which was replaced with omaya reservoir (left sided) after 5 days .Ventriculoperitoneal shunt was put on day 75 of life once CSF culture became sterile and biochemistry was within normal limits. Figure 1 attached below showing ventriculomegaly and shunts in situ.
On day 10 of life, baby had apnea and repeated desaturation, so was intubated and put on mechanical ventilator. Repeated chest x ray showed right upper zone opacity. After apnea baby also had poor perfusion so received normal saline boluses and started on dopamine which was gradually tapered and stopped after 3 days. After that baby was weaned off from ventilator on day 23 of life and shifted on oxygen by HHHFNC. Gradually settings of HHHFNC was decreased and baby weaned off from it on day 27 of life. Baby maintained saturation on room air without distress thereafter.
TPN was stopped on day 10 of life. OG feed was again started after 6th day of surgery and gradually progressed. IV fluid was stopped on day 23 of life and was on full OG feed. Oral feed was tried on day 29 of life and fully established by day 73 of life. At discharge baby was on full oral feeds and gaining weight.
Neurological behavior of the baby remained appropriate for gestational age at discharge. Occupational therapy was given during hospital stay and plan to continue during follow up too. Baby needs long-term neurodevelopmental follow- up.
Discussion
E. meningoseptica cause meningitis mostly in immunocompromised individuals. India got its first reported case of Elizabethkingia meiningitis in 1988. Many case reports of this organism causing septicemia, meningitis, endocarditis has been published since then [6, 7, 8, 9, 10]. Elizabethkingia meningoseptica is uncommon organism which shows resistance too many antibiotics. It is gram negative organism which responds well to drugs active against gram positive organism [11]. Although few publication show resistance to vancomycin [12]. We too started treatment with these drugs as per blood culture sensitivity but despite 8 weeks of drug treatment Csf clearance of Elizabethkingia meningoseptica was not seen, so gave trial for intraventricular vancomycin.
The CSF concentration of intraventricular administration of vancomycin of10 mg and 20 mg in previous clinical trials showed that the concentration in the CSF is prolonged at a high level of 20 mg. But the results showed no difference in efficacy with dosage difference although the organism was staphylococcus [13, 14]. No conclusive study was found for dosage levels against Elizabethkingilla.
Intraventricular therapy has been in limited use owing to its reported toxic effects in various studies. These includes seizures, transient hearing loss and chemical ventriculitis [15, 16]. Seizures, transient hearing loss had been reported with gentamicin and vancomycin. Less side effects reported with newer drugs like polymyxin B, colistin [17]. Meropenem and netilmicin also showed no adverse effects in one case report [17]. In our study, we did not encounter any patient with any serious adverse effects which supports the safety of intraventricular therapy, if used in the correct dosage.
High drug level definitely could have causing auditory disorders and central nervous system disorders. High dose effect on brain and long term sequelae are less known [18, 19, 20]. One study showed decline in brain and ear involvement at CSF concentration of vancomycin ≤20 mg/L [21]. So we decided to give vancomycin 10 mg intraventricularly in our patient. Regarding the interval of intraventricular vancomycin, administration in 12-24 hourly interval is the current regime. We decided to give 24 hourly. Intraventricular vancomycin was administered for 21 days. Csf culture done after 18 days course of intraventricular vancomycin was sterile.
Conclusion
Use of intraventricular vancomycin in neonates especially preterm neonates needs more validation as data available is not enough and needs time test trial. Long term neurological follow up needed to look for adverse effect of vancomycin over neurological behavior of infant over a period of time. Dose and duration of vancomycin needs clinical trial as per CSF concentration and time kill curve test .We got quick response to vancomycin given intraventricularly, so will look for more detailed study in future if encountered with such resistant Elizabetkingia meningoseptica again.
References
-
Kim KK, Kim MK, Lim JH, Park HY, Lee ST (2005) Transfer of Chryseobacterium meningosepticum and Chryseobacterium miricola to Elizabethkingia gen. nov. as Elizabethkingia meningoseptica comb. nov. and Elizabethkingia miricola comb. nov. Int J Syst Evol Microbiol 55: 1287-1293.
-
King EO (1959) Studies on a group of previously unclassified bacteria associated with meningitis in infants. Am J Clin Pathol 31(3): 241-247.
-
Jean SS, Lee WS, Chen FL, Ou TY, Hsueh PR (2014) Elizabethkingia meningoseptica: an important emerging pathogen causing healthcare-associated infections. J Hosp Infect 86(4): 244-249.
-
Dziuban EJ, Franks JL, So M, Peacock G, Blaney DD (2018) Elizabethkingia in children: a comprehensive review of symptomatic cases reported from 1944 to 2017. Clin Infect Dis 67(1): 144-149.
-
Kirby JT, Sader HS, Walsh TR, Jones RN (2014) Antimicrobial susceptibility and epidemiology of a worldwide collection of Chryseobacterium spp.: report from the SENTRY antimicrobial surveillance program (1997-2001). J Clin Microbiol 42(1): 445-448.
-
Bomb K, Arora A, Trehan N (2007) Endocarditis due to Chryseobacterium meningosepticum. Indian J Med Microbiol 25(2): 161-162.
-
Sarma S, Kumar N, Jha A, Baveja U, Sharma S (2011) Elizabethkingia meningosepticum: An emerging cause of septicemia in critically III patients. J Lab Physicians 3(1): 62-63.
-
Dias M, Fernandes A, Furtado Z (2012) Case series: Elizabethkingia meningosepticum. J Clin Diagn Res 6(9):1550-1551.
-
Gokul BN, Chandramukhi A, Ravikumar R, Aroor S (1989) Flavobacterium meningosepticum meningitis in a neonate. Indian J Pediatr 56(4): 524-527.
-
Padmaja P, Verghese S, Bhirmanandham CV, Ajith, Thirugnanasambandham S, et al. (2006) Chryseobacterium meningosepticum: An uncommon pathogen causing adult bacterial meningitis. Indian J Pathol Microbiol 49(2): 293-295.
-
Soman R, Agrawal U, Suthar M, Desai K, Shetty A (2017) Successful management of Elizabethkingia meningoseptica meningitis with intraventricular vancomycin. J Assoc Physicians India 65(10): 98-99.
-
Jean SS, Hsieh TC, Ning YZ, Hsueh PR (2017) Role of vancomycin in the treatment of bacteraemia and meningitis caused by Elizabethkingia meningoseptica. Int J Antimicrob Agents 50(4): 507-511.
-
Rodvold KA, Everett JA, Pryka RD, Kraus D (1997) Pharmacokinetics and administration regimens of vancomycin in neonates, infants and children. Clin Pharmacokinet 33(1): 32-51.
-
Nagl M, Neher C, Hager J, Pfausler B, Schmutzhard E, et al. (1999) Bactericidal activity of vancomycin in cerebrospinal fluid. Antimicrob Agents Chemother 43(8): 1932-1934.
-
Khawcharoenporn T, Apisarnthanarak A, Mundy LM (2010) Intrathecal colistin for drug-resistant Acinetobacter baumannii central nervous system infection: A case series and systematic review. Clin Microbiol Infect 16(7): 888-894.
-
Ng J, Gosbell IB, Kelly JA, Boyle MJ, Ferguson JK (2006) Cure of multiresistant Acinetobacter baumannii central nervous system infections with intraventricular or intrathecal colistin: Case series and literature review. J Antimicrob Chemother 58(5): 1078-1081.
-
Remes F, Tomas R, Jindrak V, Vanis V, Setlik M (2013) Intraventricular and lumbar intrathecal administration of antibiotics in postneurosurgical patients with meningitis and/or ventriculitis in a serious clinical state. J Neurosurg 119(6): 1596-1602.
-
LeRoux P, Howard MA, Winn HR (1990) Vancomycin pharmacokinetics in hydrocephalic shunt prophylaxis and relationship to ventricular volume. Surg Neurol 34(6): 366-372.
-
Thilmann AF, Möbius E, Pondoll K (1992) Intraventricular antibiotic therapy. Nervenazt 63(2): 108-112.
-
Wilson HD, Bean JR, James HE, Pendley MM (1978) Cerebro spinal fluid antibiotic concentrations in ventricular shunt infections. Childs Brain 4(2): 74-82.
-
Luer MS, Hatton J (1993) Vancomycin administration into the cerebrospinal fluid: a review. Ann Pharmacother 27(7-8): 912-921.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?