A Case Report of Osteoblastoma of Distal Femur: A Diagnostic Challenge
Osteoblastoma is uncommon benign bone tumour, representing approximately 1% of all primary bone tumour. The nidus of osteoblastoma is similar to that of osteoid osteoma on histopathology and imaging, but it is larger in size. Osteoblastomas have a variable imaging appearance ranging from indolent to very aggressive, and many times difficult to differentiate from osteoid osteoma only based on imaging. A combination of thorough medical history, radiographic examination and clinical suspicion is at most important for differentiating osteoblastoma from osteoid osteoma. We present a case report of benign osteoblastoma of meta-diaphysis of distal femur in 15-year-old male child and histopathological confirmation
Summary
Key Points
Keywords: Osteoblastoma; Osteoid Osteoma; Benign Tumour; Bone Tumour
Introduction
Osteoblastoma is uncommon benign bone tumor, representing approximately 1% of all primary bone tumor and 3% of all benign bone tumor [1]. The nidus of osteoblastoma is simulating to that of osteoid osteoma on histopathology and imaging, but it is larger in size [2]. Osteoblastoma is usually diagnosed in the second decade of life and have a 2:1 male predominance [3, 4]. It occurs, in order of frequency, in the spine, femur, foot and ankle [4]. The basis for diagnosis in most of cases is from clinical, radiological, and mainly histopathological examination. Osteoblastomas have a variable imaging appearance ranging from indolent to very aggressive, and many times difficult to differentiate from osteoid osteoma only based on imaging [5].
Case Report
Case History
15-year-old male patient was admitted in our hospital with history of right knee pain for the past 4 months. There was no history of injury. The pain was progressive and worse at night. The pain was initially relieved by Non-Steroidal Anti- Inflammatory Drugs (NSAIDs) but in the last few weeks only partially relieved and the patient was forced to limit activities due to the pain. There were no constitutional symptoms such as fever, weight loss or malaise.
Physical Examination and Laboratory Investigations
Involved knee was not swollen but tender on palpation, with no obvious erythema or increase in temperature. The patient was otherwise fit and well. Blood analysis was unremarkable.
Radiological Investigations
Right knee radiographs (Antero posterior and lateral views) were obtained (Figure 1), which revealed a well- defined, eccentrically located lytic lesion in the lateral cortical and subcortical region of meta-diaphysis of distal femur. It showed central ossifications and significant surrounding sclerosis with ill-defined overlying cortex at places.
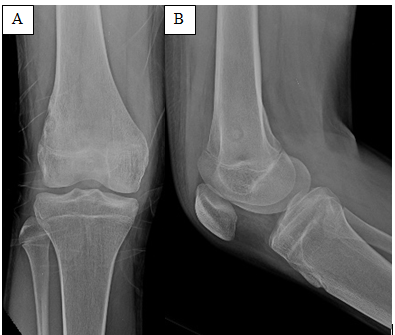
However, no significant surrounding soft tissue was noted. On Computed Tomography (CT) scan (Figure 2), the lytic lesion was located in the cortical and subcortical region of meta-diaphysis of distal femur along its lateral cortex, causing focal cortical bulge and expansion with thinned out overlying cortex and cortical disruption at places. It confirmed the central ossification and significant thickening and sclerosis of adjacent cortex and medullary cavity with mild benign looking periosteal reaction. No significant soft tissue component was noted. The lesion measured 1.8 cm in maximum length. Based on the imaging morphology and size of the lytic lesion, benign lesion such as osteoid osteoma was considered as a primary diagnosis and osteoblastoma was close differential diagnosis.
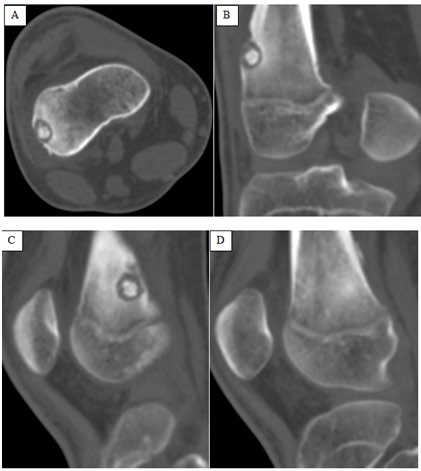
Figure 2: Axial (A), Coronal (B) and Sagittal (C,D) images of CT scan confirmed the mildly expansile lytic lesion with central matrix ossifications located in the cortical and subcortical region of meta-diaphysis of distal femur along its lateral cortex, causing focal cortical bulge and expansion with thinned out overlying cortex and cortical disruption at places (A,B). Note, the central ossification with significant thickening and sclerosis of adjacent cortex & medullary cavity (C) and benign looking periosteal reaction (D).
Therapeutic Intervention
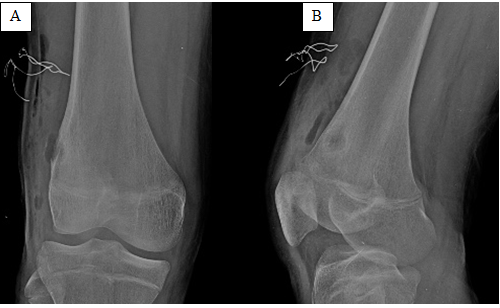
In view of significant progressive pain and only partially relieved by NSAIDS, the patient underwent excision and curettage of the lesion through an antero-lateral incision. Curettage of the nidus and cauterization of the wall was performed (Figure 3).
Final Diagnosis
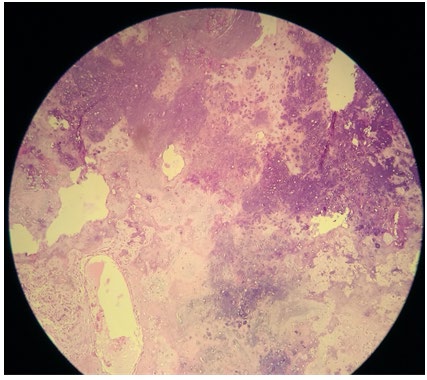
Microscopic examination (Figure 4) showed anastomosing trabeculae of osteoid and woven bone, rimmed by single layer of benign activated osteoblasts and numerous osteoclasts, loose fibrovascular stroma between bone trabeculae with cartilaginous component, confirming the diagnosis of osteoblastoma over osteoid osteoma.
Outcome
The patient was immediately relieved from nocturnal pains and progressively completely relieved from knee pain.
He was discharged on next day with stable condition.
Discussion
Osteoblastoma is a rare benign bone-forming neoplasm, accounting for ~1% of all primary bone tumors and affects mainly adolescents and young adults with a male predominance [1, 2, 3, 4]. It can involve any bone, commonly arises in the posterior elements of the spine and the sacrum followed by the proximal femur, distal femur, and proximal tibia [6]. It is also called giant osteoid osteoma, can occur in an intramedullary, cortical, or periosteal location [7]. It has no pathognomonic clinical or radiological features that could allow for a positive diagnosis of osteoblastoma [8]. Severe pain that is worse at night and relief from NSAIDS are not typically seen as with osteoid osteoma.
Osteoblastomas can have a wide range of radiographic patterns, however the lesions are typically larger than 1.5-2 cm in size although smaller lesions may occur [9, 10]. Radiographs usually show an expansile, well- circumscribed, lytic lesion with matrix ossification and mild surrounding sclerosis with cortical expansion in 75-94%, and cortical destruction in 20-22% [4, 7, 11]. Other imaging methods such as bone scintigraphy, CT and MRI may provide information about the extent of the lesion [11]. CT scan reveals similar findings as radiograph; however, the internal matrix mineralization is better appreciated on CT. Magnetic Resonance Imaging tend to be non-specific and often overestimate the lesion [12].
The radiological differential diagnosis may include osteoid osteoma, bone abscess, chondromyxoid fibroma, enchondroma and osteosarcoma [3, 4]. Chondroid like matrix calcifications may be present in the center of the nidus, at times resembling the dense osteoid matrix of osteosarcoma The lesion may mimic an osteoid osteoma when surrounded by a sclerotic rim and located intracortically or periosteally; however, osteoblastoma are typically larger than 2 cm at presentation and exhibit growth on serial examinations, while the osteoid osteomas tend towards regression [3, 7] because of absence of limited growth potential. Another important distinctive feature to differentiate it from osteoid osteoma is characteristic of pain, which is dull, localized and insidious onset in osteoblastoma with less severity than that of osteoid osteoma. It is not classically nocturnal and responds to NSAIDS only in 7% of the cases. While in osteoid osteoma, pain is classical and more severe at night but is dramatically relieved by NSAIDS, serves as an important clue to the diagnosis [13]. The lesion can be removed with intralesional curettage or marginal en block excision, depending on the clinical situation, and location within the bone [14].
Conclusion
A combination of thorough medical history, radiographic examination and clinical suspicion is at most important for differentiating osteoblastoma from osteoid osteoma. In our case, total resection of the lesion resulted in complete remission of the patient’s symptoms.
References
-
Unni KK (1996) Benign osteoblastoma (giant osteoid osteoma). In: Unni KK, (Eds.), Dahlin’s Bone Tumors, General Aspects and Data on 11087 Cases, 5th (Edn.), Lippincot Raven, Philadelphia.
-
Mortazavi SM, Wenger D, Asadollahi S, Shariat Torbaghan S, Unni KK, et al. (2007) Periosteal osteoblastoma: report of a case with a rare histopathologic presentation and review of the literature. Skeletal Radiol 36(3): 259-264.
-
Greenspan A (2004) Orthopedic imaging: a practical approach. 4th (Edn.), Lippincott Williams and Wilkins, pp: 573-594.
-
Yochum TR, Rowe LJ (2005) Essentials of Skeletal Radiology. 3rd (Edn.), Lippincott Williams and Wilkins 2: 1262-1267.
-
Sharma V, Chew FS, Hoch B (2015) Periosteal osteoblastoma: Multimodal imaging of a rare neoplasm. Radiol Case Rep 4(4): 329.
-
Lucas DR (2010) Osteoblastoma. Arch Pathol Lab Med 134(10): 1460-1466.
-
Kroon HM, Schurrnans J (1990) Osteoblastoma: clinical and radiologic findings in 98 new cases. Radiology 75: 783-790.
-
Manaster BJ (1994) Musculoskeletal tumor imaging. In: Putman CE & Ravin CE (Eds.), Textbook of Diagnostic Imaging, 2nd (Edn.), W.B. Saunders, Philadelphia.
-
Eisenberg RL (2009) Bubbly lesions of bone. AJR Am J Roentgenol 193 (2): 79-94.
-
Rodriguez DP, Poussaint TY (2010) Imaging of back pain in children. AJNR Am J Neuroradiol 31 (5): 787-802.
-
Stoller DW, Tirman PFJ, Bredella MA (2004) Diagnostic imaging, orthopaedics, 1st (Edn.), Amirsys Inc, pp: 8-13.
-
Shaikh MI, Saifuddin A, Pringle J, Natali C, Sherazi Z (1999) Spinal osteoblastoma: CT and MR imaging with pathological correlation. Skeletal Radiol 28(1): 33-40.
-
Atesok KI, Alman BA, Schemitsch EH, Peyser A, Mankin H (2011) Osteoid osteoma and osteoblastoma. J Am Acad Orthop Surg 19(11): 678-689.
-
Frassica FJ, Waltrip RL, Sponseller PD, Ma LD, McCarthy EF (1996) Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 27(3): 559-74.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?