Congenital Giant Melanocytic Nevus with Meningeal Melanocytosis in a Term Neonate- A Case Report
Congenital giant melanocytic nevus presenting in the neonatal period is a clinical diagnosis, but the extra dermatology manifestations require early recognition. Meningeal melanocytosis is one such association which increases the risk of epilepsy. We report a neonate with large congenital melanocytic nevus over the torso with satellite lesions presenting with meningeal melanocytotic in the right parietal and cerebellar region. We discuss the clinical course, management and review the literature on this condition.
Introduction
Congenital Giant melanocytic nevus presenting in the neonatal period is a rare entity with a reported incidence of 1 in 20000 live births [1]. Even though the clinical diagnosis is straightforward, the timely recognition of non-dermatological manifestations, predicting the risk of epilepsy, multidisciplinary management and counselling of family members is challenging. We report a case of congenital giant melanocytic nevus with meningeal melanocytosis in a term baby.
Case Report
A male baby born with birth weight of 1860gram via vaginal delivery to a 24-year old primigravida mother at 35+ 2 weeks of gestation had a huge hyperpigmented skin lesion of ≥ 20 cm diameter covering the posterior scalp, neck, chest wall, shoulder and upper back. It contained irregularly shaped macules, papules, patches, and plaques of variegated colours (greyish, blackish and light-to-dark brown). Other smaller pigmented nevi were scattered across the thigh, and measured 0.5-1 cm in diameter. There were no hairs noted over the lesions. On systemic examination, there were no signs of neurological abnormality. In view of the extensive involvement of the nevus, magnetic resonance imaging of the brain and spine was done which showed flair hyperintensities in the right parietal region and bilateral cerebellar hemisphere. Bedside amplitude-integrated electroencephalogram showed a normal continuous pattern with no evidence of seizures. A paediatric dermatology and plastic surgery consult was done and they advised follow up visits with close monitoring of the lesion for any changes in its pattern and if required, excision-grafting at a later stage. Ophthalmological evaluation was normal. Neonate remained hemodynamically stable on exclusive breastfeeding and continued on multidisciplinary care. Family members were counselled by a neonatologist and is on regular follow-up.
Discussion
Congenital Melanocytic nevus (CMN) is a benign proliferation of naevomelanocytes with larger lesions being rarer and having higher malignant potential [1]. The size of small CMNs is <1.5cm in diameter, medium size is of 1.5 to 19.9cm, and large or giant nevus measures >20cm in diameter [2]. CMN if presents on the torso as in the index neonate are predicted to grow by a factor of 2.8 by adulthood [1]. These lesions are due to over-proliferation of melanocytes and can start developing in utero as early as 5th week of gestation. A common CMN mutation is the N-Ras pathway implicated in the regulation of melanocyte migration and proliferation, with other genes such as BRAF, KRAS, APC, and MET variants are also being reported [3].
In the neonatal period, the giant nevus is associated with satellite nevus in up to 80% of cases and evolves over time and develops changes in pigmentation, dermal nodules and hypertrichosis [4]. Diagnosis is often clinical as in our case, examination with dermatoscopy or biopsy is used only in patients with diagnostic dilemmas. MRI brain is useful in diagnosing meningeal melanocytosis, which is reported in up to 17%-41% of such high risk infants and distribution of the same has been predictive of risk of subsequent epilepsy [5]. Those with bilateral amygdala involvement have the highest frequency of seizure-free patients on antiepileptic drugs whereas those with lesions in multiple locations might develop drug-resistant epilepsy [6]. The mean age of seizures is 5 months in these patients and are asymptomatic in neonatal period [7]. The chances for malignant transformation including both cutaneous and extracutaneous malignant melanoma are upto10% in these cases.
The role of excision procedures such as surgery or the use of laser, or dermal ablation for the purpose of reducing the malignant change and aesthetic appearance remains controversial [8] and affection of quality of life is an additional concern in the long term [9] Figures 1 & 2.
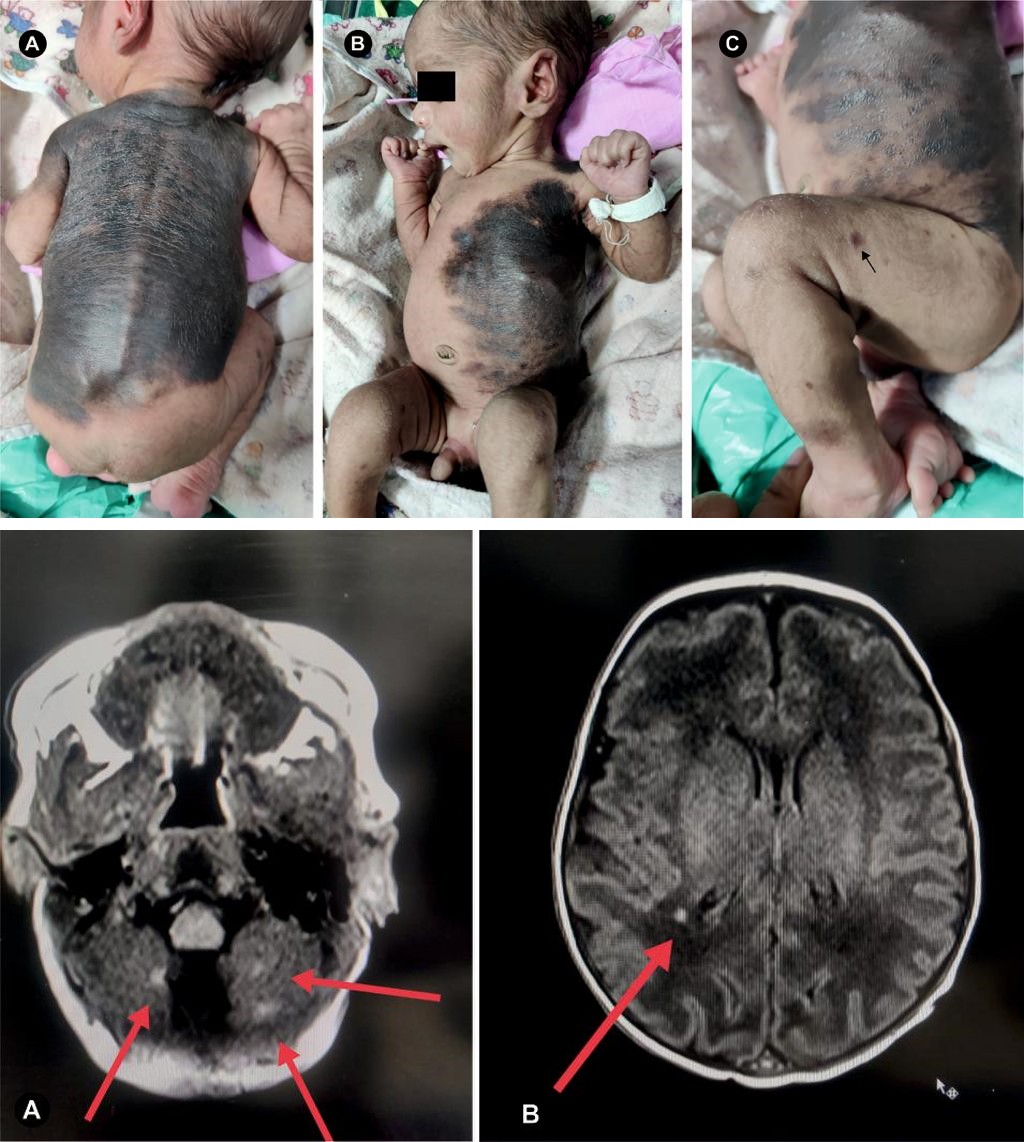
Figure 1A-C: Giant melanocytic nevi on posterior aspect of neck, shoulder and upper back, B: Giant Nevus extending from right upper chest to abdomen, C: Satellite Lesions over thigh(black arrow).
Figure 2A,B: MRI Flair images showing hyperintensities in the right parietal and cerebellar region as indicated by red arrows.
Acknowledgement: The authors thank Dr. Sangeeta Ravat, Dean, Seth GS Medical College and KEM Hospital, Mumbai for granting permission for publication.
• Patient consent for publication: Patient consent for publication was obtained.
References
-
Kovalyshyn I, Braun R, Marghoob A (2009) Congenital melanocytic naevi. Australas J Dermatol 50(4): 231-240.
-
Ibrahimi OA, Alikhan A, Eisen DB (2012) Congenital melanocytic nevi: where are we now? Part II. Treatment options and approach to treatment. J Am Acad Dermatol 67(4): 515,e1-13.
-
Martins da Silva V, Martinez-Barrios E, Tell-Mart TG, Dabad M, Carrera C, et al. (2019) Genetic abnormalities. in large to giant congenital nevi: beyond NRAS mutations. J Invest Dermatol 139(4): 900-908.
-
Arneja JS, Gosain AK (2009) Giant congenital melanocytic nevi. Plast Reconstr Surg 124(1S): 1e-13e.
-
Jakchairoongruang K, Khakoo Y, Beckwith M, Barkovich AJ (2018) New insights into neurocutaneous melanosis. Pediatr Radiol 48(12): 1786-1796.
-
Pellino G, Gencarelli J, Bertelli S, Russo A, Fiumana E, et al. (2020). Epilepsy in isolated parenchymal neurocutaneous melanosis: A systematic review. Epilepsy Behav 107: 107061.
-
Eggen CAM, Lommerts JE, van Zuuren EJ, Limpens J, Pasmans SGMA, et al. (2018) Laser treatment of congenital melanocytic naevi: a systematic review. Br J Dermatol 178(2): 369-383.
-
Polubothu S, Kinsler VA (2020) Final congenital melanocytic naevi colour is determined by normal skin colour and unaltered by superficial removal techniques: a longitudinal study. Br J Dermatol 182(3): 721-728.
-
Neuhaus K, Landolt MA, Theiler M, Schiestl C, Masnari O (2020) Skin-related quality of life in children and adolescents with congenital melanocytic naevi - an analysis of self and parent reports. J Eur Acad Dermatol Venereol 34(5): 1105-1111.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?