Bed Wetter: An Upset 9 Y Old Boy with Primary Mono symptomatic Nocturnal Enuresis
Background: Bed wetting or nocturnal enuresis is seen in 15% of children over 5 Yr. it is primary in 75-90% of cases and the monosymptomatic enuresis is more common and should be estimated after ruling out other symptoms. In here we report a case of a 9-year-old boy who referred with a permanent primary monosymptomatic nocturnal enuresis and he was quite upset and had a tired and unhappy family. Case Presentation: This is a clinical combined therapy case study. A 9-year-old boy was referred with a chief complaint of bed wetting, which was primary and monosymptomatic, but because of experiencing of wrong incomplete period of treatments, they were disappointed. He had tried one or two drugs each time. In this approach I put him under simultaneous given multifaceted treatment, include education and advises, motivational therapies, conditional therapy, and pharmacotherapies. And this situation revealed a faster and also more persistent result and this motivated the child and his family to complete the treatment course (for 4 months) without any relapse after completion this period. Conclusion: Our study shows that nocturnal enuresis, even primary monosymptomatic types, which are most common types of enuresis may need multi-faceted treatment to make child calm and his family comfort.
Background
By 5 years of age, 90- 95% of children are nearly completely continent during the day and 80 – 85% are continent at night. Nocturnal enuresis refers the occurrence of involuntary voiding at night after 5 yr old. Overall, 75% of children with enuresis are wet only at night, and 25% are incontinent day and night and monosymptomatic enuresis is more common than poly-symptomatic enuresis [1]. In here we report a case of a 9-year-old boy who was referred because he was quite upset because his parents blamed him, frequently.
A 9-year-old boy was referred to the Pediatric Nephrology clinics because of bed wetting. He was quite upset about his bedwetting, particularly because he had recently wet the bed when he stayed at his cousin’s house and has been teased about this between his cousins. Both parents were Army employees and accompanied him. He was the only child in his family and his parents were non-consanguineous, without any positive childhood history of bedwetting. He was born term and without any significant medical history. He had never got urinary control at night, while he has been able to control his urine during the day since he was 30 months old. He had nocturnal enuresis 5-6 /weeks, didn’t wake up when it happened and with a large pool of urine.
He was given Oxybutynin (5 mg one hour before sleeping) at 7 years old for 2 months and due to failure to respond, Imipramine (5 mg every night) was added. Although there was no response after 4 months. So, the parents gave up drugs and bought an enuresis alarm. The alarm woke him up but he was already wet so again they gave up after 2 weeks. In my first visit, he hadn’t taken medicine in the last 8 months, but his mother woke him up twice at night, which was affecting her ability to work and parents believe he is lazy and should be able to control his bladder at this age. This issue had caused serious confrontations and corporal punishments by parents.
He has a normal weight, height and all physical examinations include Blood pressure, genitalia, spine and lower limb neurologic exams were normal. He had more than 5 normal urine analysis, urine cultures and also normal kidneys in ultrasonography which had been done 2 months ago. Fast blood sugar and electrolytes were done 2 months ago, and all were normal. So, we were facing a 9 years old boy with primary nocturnal enuresis and lack of arousal from sleep. Unfortunately, his parents weren’t sympathetic and didn’t agree to start medicine or the commitment to make an enuresis alarm. It was very important to emphasize, his enuresis is out of his control.
In this setting, we preferred to start widespread fast acting pharmacotherapy along with psychosocial consults and educations at the same time. First educations and advises include regular daytime fluid intake, not punishing the child, prohibition of eating caffeinated drinks and fatty dinners, consume whole grains bread in the diet to prevent constipation, and making the existing condition more bearable by using washable/disposable sheets and adding winger for washing the child’s cloths to get rid of urine odor.
For motivational therapy, we used a minor behavioural intervention such as star charts award and positive parent’s reinforcement. Because the child was highly motivated and we found lack of arousal, we used enuresis alarm, but we made the child himself responsible for setting his alarm, such as connecting it, changing his cloths if it wasn’t worked and again starting it (may be 1-2 times each night at the beginning of treatment).
In this setting, we prescribed short term Desmopressin to provide some respite to his family. We hoped it could be withdrawn in a structured fashion, assisted by the use of our other methods such as enuresis alarm, when the family were become ready to support him.
In this case we didn’t have any futures due to bladder instability and we didn’t use anticholinergics, although we worked on his bladder retaining forces by adding biofeedback therapies for first 2 weeks of our treatment. At least as we found that it may take a long time to achieve consistent night time dryness, so we referred them for psychological consult. The therapeutic response started after 2 weeks and at the first month of treatment, the child experienced completely dry nights (about 5-6 days/ week). He was excited and his parents became happy and satisfied. His treatment continued up to 3 months and then tapered his drug in 3 months. Now he is 10 years old boy, who has never been a bed wetter after ending his treatment and he can participate in school camps or stay with his friends with ease.
Discussion
Enuresis refers to discrete episodes of urinary incontinence during sleep in child ≥5 years of age [1]. It may be primary (75-90%) with nocturnal urinary control that never achieved, or may be secondary (10-25%), in which the child was dry at night for at least a few months [2]. Monosymptomatic enuresis is defined as enuresis without any other lower urinary tract symptoms or bladder dysfunction, although the pathogenesis and evaluation of the two forms overlap [3]. In almost all cases, monosymptomatic nocturnal enuresis resolves spontaneously and this suggests that delayed maturation of a normal developmental process plays a role in nocturnal enuresis. Although there is also a genetic tendency (approximately 50%) toward nocturnal enuresis. Other related factors, including nocturnal polyuria, disturbed sleep, small bladder capacity, and detrusor over activity [4].
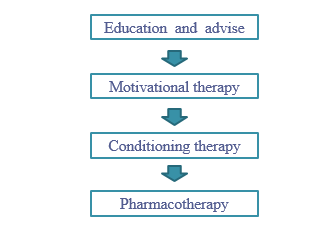
The evaluation of monosymptomatic nocturnal enuresis includes a careful fluid intake history, the pattern of nocturnal enuresis. Physical examination includes abdominal palpation, rectal examination after voiding (to ruled out distended bladder) and also neurologic examinations. Finally, if everything is normal, we just need an overnight fast urinalysis (to evaluate for specific gravity, glycosuria or any other abnormalities) [5]. At first all coexisting conditions such as constipation, sleep disordered breathing or attention deficit hyperactivity disorder should be treated [6]. Then we start our treatment in 4 steps (Figure 1) and in each of them, several methods are being used (Table 1).
Emphasize that enuresis isn’t a disease and parents should avoid express anger, negativity, or blame toward the child, which can affect the child’s psychological development adversely and causing delay in getting better over time [6].
| Type of Treatment | Strategies |
|---|---|
| Education and advise | avoid punishment |
| Washable/ disposable sheets | |
| Voiding just before going to bed | |
| Restrict fluid intake after 7pm | |
| Prevent constipation | |
| Keep lower limb warm in bed | |
| Avoid high fat meals, specific drinks after 5 pm | |
| Bladder training | |
| Wake for urination 1-2/night | |
| Motivational therapy | Chart dry and wet nights in the presence of the child |
| Minor behavioral interventions such as charts award and positive reinforcement | |
| Conditioning therapy | Enuresis alarms |
| Carrying out all the tasks of the device by the child | |
| Biofeedback therapy | |
| Pharmacotherapy | Desmopressin |
| Anti-depressant drugs (Imipramine) | |
| Anticholinergic drugs (Oxybutynin, Tolterodine) | |
| Complementary medicine | |
| Acupuncture therapy |
Table1: Treatment’s Strategies for Mono Symptomatic- Enuresis.
Practical advices include bed protection with disposable products, using room deodorizers, adding 0.5 cup of vinegar for washing under wears, restricting fluid intake to 2 to 6 oz. after 6 PM, prohibiting specific drinks such as cola or tea or bubbles, citrus juices & sports drinks particularly after 5 PM , consuming whole grains bread, fresh fruits and vegetables ( to prevent constipation), prohibiting fast foods and high-fat meat for dinner and keeping their lower limbs warm during sleeping time [7].
Motivational therapy (star charts after dry nights) is used to give he/she responsibility and keeping a record of progress, especially for who wets only 1-2/ week between 5 to 7 years old [6].
The most effective long-term therapy is conditioning therapy with using enuresis alarm [7]. Pharmacotherapy, as the second line therapy should be avoided for child < 6 years of age [1]. Desmopressin (a synthetic analogue of the natural ADH), is FDA-approved in children, reduces urine production overnight and available as tablet or nasal spray. Treatment duration is at least 3 months with 40% effectiveness, and hyponatremia may occur if parents don’t restrict fluid intake in nights [8]. Anti-cholinergic drugs such as Oxybutynin or Tolterodine is indicated in overactive bladders, and constipation is the potential side effect [4].
Tricyclic Antidepressants (TCAs) such as Imipramine, stimulate vasopressin secretion and relax the detrusor muscle with 30-60% effectiveness and dry mouth, anxiety and insomnia are the potential complications. It must be avoided in child with long OT syndrome [6]. Complementary approaches include hypnosis, psychotherapy, and traditional medicine (using herbal drugs such as sweetbread, olive oil, cinnamon). In addition, modern traditional therapies such as acupuncture and biofeedback therapy (a noninvasive stimulation of pelvic muscles and detrusor contractions) are effective in refractory enuresis [9]. Refractory enuresis needs multi-faceted treatment and sometimes other specialists such as psychologists, nutritionists or neurologists [1].
Conclusion
Our study shows that inappropriate treatment of a common complaint in a child can disturb and affect quality of his family life and sometimes both physicians and a hasty family, who are in hurry to stop treatment and imposed restrictions, backfired and get stuck in a vicious cycle.
References
-
Jack S, Kliegman RM, ST Geme J, Blum N, Shah S, et al. (2020) Elder in Enuresis and Voiding Dysfunction. Nelson textbook of Pediatrics 21th edition Canada, pp: 2820-2822.
-
Austin PF, Bauer SB, Bower W, Chase J, Franco I, et al. (2016) The standardization of terminology of lower urinary tract function in children and adolescents Update report from the standardization committee of the International Children’s Continence Society. Neurourol Urodyn 35(4): 471-481.
-
Nevéus T, Fonseca E, Franco I, Kawauchi A, Kovacevic L, et al. (2020) Management and treatment of nocturnal enuresis-an updated standardization document from the International Children’s Continence Society. J Pediatr Urol 16(1): 10-19.
-
Naiwen D Tu, Laurence S Baskin, Anne M Arnhym (2022) Nocturnal enuresis in children etiology and evaluation.
-
Neveus T, Eggert P, Evans J, Macedo A, Rittig S, et al. (2010) Evaluation and treatment for monosymptomatic enuresis a standardization document from the International Children’s Continence Society. J Urol 183(2): 441-447.
-
National Clinical Guideline Centre (2010) Nocturnal Enuresis The Management of Bedwetting in Children and Young People. London.
-
Dormanesh B (2021) non-medical treatment for children nocturnal enuresis. Presented in the Webinar of Iranian Society of Pediatric Nephrology- Tehran.
-
Dormanesh B (2021) Enuresis in children, Presented in 32 nd International Congress on Pediatrics, Tehran- Iran.
-
Dormanesh B, Bayhaghi MH, Salehi E (2016) Sweetbread consumption in the treatment of Enuresis in children from the viewpoint of Islam Presented in the Second International Congress of Nephrology & Urology, Terhran –Iran.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?