Prevalence of Corona Virus in Khaipure Medical College Hospital Pakistan
Corona virus disease (COVID-19) is an infectious disease is contagious, lethal and endemic caused by a newly discovered corona virus. Most people infected with the COVID-19 virus will experience mild to moderate respiratory illness and recover without requiring special treatment. Older people and those with underlying medical problems like cardiovascular disease, diabetes, chronic respiratory disease, and cancer are more likely to develop serious illness. The COVID-19 virus spreads primarily through droplets of saliva or discharge from the nose when an infected person coughs or sneezes, so it’s important that you also practice respiratory etiquette (for example, by coughing into a flexed elbow). At this time, there are no specific vaccines or treatments for COVID-19. However, there are many ongoing clinical trials evaluating potential treatments. WHO will continue to provide updated information as soon as clinical findings become available?
Introduction
Corona viruses are enveloped single-stranded RNA viruses that are zoonotic in nature and cause symptoms ranging from those similar to the common cold to more severe respiratory, enteric, hepatic, and neurological symptoms. Coronavirus has caused two large-scale pandemics in the last two decades: [1, 2]. Reported symptoms include fever, cough, fatigue, pneumonia, headache, diarrhea, hemoptysis, and dyspnea. Preventive measures such as masks, hand hygiene practices, avoidance of public contact, case detection, contact tracing, and quarantines have been discussed as ways to reduce transmission. To date, no specific antiviral treatment has proven effective; hence, infected people primarily rely on symptomatic treatment and supportive care. The corona virus belongs to a family of viruses that may cause various symptoms such as pneumonia, fever, breathing difficulty, and lung infection [3]. These viruses are common in animals worldwide, but very few cases have been known to affect humans. The World Health Organization (WHO) used the term 2019 novel coronavirus to refer to a corona virus that affected the lower respiratory tract of patients with pneumonia in Wuhan, China on 29 December 2019 [2, 3, 4]. The WHO announced that the official name of the 2019 novel corona virus is corona virus disease (COVID-19) [4]. And the current reference name for the virus is severe acute respiratory syndrome corona virus 2 (SARS- CoV-2). It was reported that a cluster of patients with pneumonia of unknown cause was linked to a local Huainan South China Seafood Market in Wuhan, Hubei Province, China in December 2019 [5]. In response to the outbreak, the Chinese Center for Disease Control and Prevention (China CDC) dispatched a rapid response team to accompany health authorities of Hubei province and Wuhan city conduct epidemiological and etiological investigations. The WHO confirmed that the outbreak of the corona virus epidemic was associated with the Huanan South China Seafood Marketplace, but no specific animal association was identified [6]. Scientists immediately started to research the source of the new corona virus, and the first genome of COVID-19 was published by the research team led by Prof. Yong-Zhen Zhang, on 10 January 2020 [7]. Susceptibility seems to be associated with age, biological sex, and other health conditions [8]. COVID-19 has now been declared as a Public Health Emergency of International Concern by the WHO [9]. On 29 December 2019, the first four cases of an acute respiratory syndrome of unknown etiology were reported in Wuhan City, Hubei Province, China among people linked to a local seafood market (“wet market”) [2]. It appears that most of the early cases had some sort of contact history with the original seafood market [2, 10, 11, 12, 13]. Soon, a secondary source of infection was found to be human-to-human transmission via close contact. There was an increase of infected people with no history of exposure to wildlife or visiting Wuhan, and multiple cases of infection were detected among medical professionals [2, 13, 14, 15, 16]. It became clear that the COVID-19 infection occurs through exposure to the virus, and both the immunosuppressed and normal population appear susceptible. Some studies have reported an age distribution of adult patients between 25 and 89 years old. Most adult patients were between 35 and 55 years old [13], and there were fewer identified cases among children and infants [17]. A study on early transmission dynamics of the virus reported the median age of patients to be 59 years, ranging from 15 to 89 years, with the majority (59%) being male It was suggested that the population most at risk may be people with poor immune function such as older people and those with renal and hepatic dysfunction [2]. The COVID-19 has been found to have higher levels of transmissibility and pandemic risk than the SARS-CoV, as the effective reproductive number (R) of COVID-19 (2.9) is estimated to be higher than the reported effective reproduction number (R) of SARS (1.) at this early stage [14]. Different studies of COVID-19 have estimated the basic reproduction (R0) range to be from 2.6 to 4.71. The average incubation duration of COVID-19 was estimated to be 4.8 ± 2.6, ranging from 2 to 11 days [14] and 5.2 days (95% confidence interval, 4.1 to 7) [2]. The latest guidelines from Chinese health authorities stated an average incubation duration of 7 days, ranging from 2 to 14 days [18]. Coronaviruses comprise a large and diverse family of enveloped, positive-stranded RNA viruses. The Corona viridae exhibit broad host range, infecting many mammalian and avian species and causing upper respiratory, gastrointestinal, hepatic, and central nervous system diseases. In humans and fowl, coronaviruses primarily cause upper respiratory tract infections, while porcine and bovine coronaviruses establish enteric infections that result in severe economic loss. Coronaviruses of laboratory mice are, for historical reasons, designated as mouse hepatitis viruses (MHVs), but among these only a subset are strictly hepatotoxic. Enteric strains are commonly found in rodent colonies and neurotropic strains are exploited to study central nervous system infection and demyelinating disease the extraordinary variations in host range and tissue tropism among coronaviruses are in large part attributable to variations in the spike glycoprotein. The S protein is a large, type I membrane glycoprotein that contains distinct functional domains near the amino (S1) and carboxyl (S2) termini. These spikes function to define viral tropism by their receptor specificity and perhaps also by their membrane fusion activity during virus entry into cells. Recently their natural variation has attracted the attention of researchers interested in determinants of viral host range, virus entry, and virus–receptor interactions and their relationship to tropism [19]. Evidence supporting a role for spike protein projections as agents of organ tropism and pathogenesis began with comparative studies of different naturally occurring MHV strains. In essence, nucleotide sequencing revealed that alterations in virus virulence were most closely associated with differences in the spike gene. These correlative findings were recently reinforced using the new technology of targeted RNA recombination, a strategy that can introduce site-specific mutations into the 27- to 32-kb RNA genome via recombination with defined in vitro transcripts. With a collection of carefully constructed recombinant coronaviruses differing only in the spike gene, the relationship between spike variation and in vivo pathogenesis has been unequivocally established The challenge now is to understand, in mechanistic terms, how mutations in spike proteins alter in vivo virulence. This challenge is difficult in the absence of structural data for any S protein. What is known is that the peripheral S1 portion can independently bind cellular receptors while the integral membrane S2 portion is required to mediate fusion of viral and cellular membrane. While natural genetic variability is most extreme in the S1 fragment, S2 changes are also found in mutants with novel in vivo infection characteristics. Thus, it is likely that both the receptor recognition and membrane fusion properties must be investigated for a complete view of coronavirus pathogenesis. The distribution of coronavirus receptors is critical to the pathogenic outcome. In this regard, it is notable that coronavirus spikes exhibit a range of receptor specificities; MHVs enter after binding members of a pleiotropic family of carcinoembryonic antigen–cell adhesion molecules (CEACAMs); feline and porcine coronaviruses bind metalloproteases; and bovine coronaviruses recognize 9-O-acetylated silica acids [20, 21, 22, 23, 24]. This underscores the importance of describing the fusion reaction in terms of the protein conformational changes within spike–receptor complexes. Descriptions of this sort are emerging for spikes complexes with soluble CEACAM 1a receptors, which develop instability at 37°C that is recognized by the separation of the peripheral, receptor-binding S1 fragment from the integral membrane S2 fragment (Figure 1). The S2 fragment contains a putative internal fusion peptide whose precise location is not yet defined pendent membrane fusion in the process. When the unstable JHM virus is propagated extensively in tissue culture, many of the progeny viruses harbor mutations in the spike gene. Sequencing efforts in a number of laboratories have now revealed a pattern of mutations that become fixed into the JHM genome after in vitro passage. There are two fundamental changes: (1) S1 deletions that remove sequences between the receptor-binding region and the fusion-inducing fragment and (2) S2 substitution mutations that alter heptad- repeat sequences. Notably, particular S2 codon changes have been independently observed-for example, L1114 within the middle heptad is a hotspot for mutation [25, 26]. Spikes with S1 deletions or S2 substitutions are unable to mediate murine CEACAM-independent fusion, and relative to JHM, they exhibit enhanced S1-S2 stability Thus, we suggest that fusion activation is related in part to the stability of S1-S2 heteromers and that mutations fixed into JHM spike genes during growth in tissue culture (Figure 1) Schematic depiction of the murine coronavirus (strain JHM) spike protein. Spikes are synthesized in the endoplasmic reticulum and posttranslational cleaved into peripheral S1 (upper bar, aa 15-769) and integral membrane S2 (lower bar, aa 770-
1376) upon transport to the cell surface. The durability of non-covalent S1-S2 interaction is altered by mutations in different regions of the spike gene; this suggests multiple S1- S2 interacting sites (dotted lines). Binding of CEACAM receptors to S1 disrupts some or all of these non-covalent interactions. This is hypothesized to expose an internal membrane fusion peptide within S2 for insertion into target cell membranes. Target cell and virion membranes may then pinch together (fuse) by the collapse of the three predicted S2 helical regions (hatched bars) into coiled-coil structures. 372 MINIREVIEW give rise to stabilized proteins that cannot straddle the energy barrier between “native” and “fusion- active” conformations without prior murine CEACAM binding. The unstable JHM virus is set apart from its tissue culture-adapted variants in its ability to cause a rapid, disseminated, and lethal panencephalitit [27, 28]. Rapid coronavirus spread in the CNS may depend on spikes that can convert into the fusion-active conformation even without induction by receptor binding. After all, the prototype receptor CEACAM 1a is barely detectable in the murine CNS, On the other hand, spike protein instability is a disadvantage in tissue culture, and stabilized variant spikes are selected. Attenuation of these variants in the mouse might be explained by failure of the in vivo CNS environment to support their conversion into fusion-active forms. These investigations relating the function of “JHM-type” spikes to CNS infection provide but one example of how diversity among coronaviruses and their receptors provides models for understanding early events in viral pathogenesis [29].
Material and Methods
This research paper is based on the information supplied by District health officer Khairpure, as the emergency going on the district. As this is the largest district in province, with
15910squrekm, having 2.4 million populations. District further divided in 8 taulkas. In the east border with India, due to diverse religion group there is marked moment of people to covid 19 countries particularly Iran, Saudi Arabia, it is also the center of tableeghi jamat preachers.
Discussion
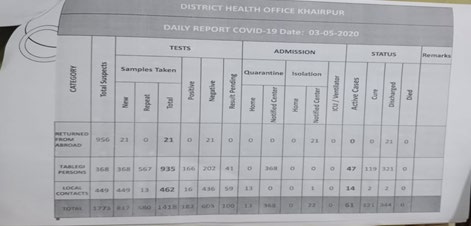
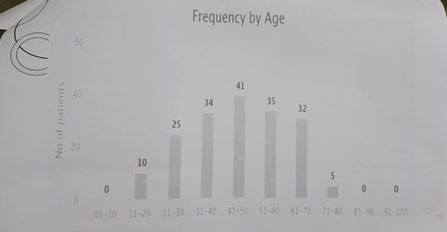
Total sample taken 1418 from which 0 died, returned from abroad 21,Tablighi persons, 935,local contacts 462. From which182 possitive,603 negative,100 pending result, 368 Figure 2, were notified, in this way positive were 11.42% this shows rate of positive cases. Corona occurs frequently 41% at the age of 41-50 years, 35% at the age 51-60 year’s age, and 34% at the age of 31-40 years of age Figure 3, shows the trend of disease pattern, this is situation where test performed cases are11.42% while we are lack of testing due to lack kits, while there is no vaccine, no specific treatment, no clinical diagnosis ,only we have an option only laboratory diagnosis which is very costly in this poor country like Pakistan.
References
-
Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020) A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 382: 727-733.
-
WHO (2020) Coronavirus.
-
WMHC (2020) Wuhan Municipal Health and Health Commission’s Briefing on the Current Pneumonia Epidemic Situation in Our City.
-
Li Q, Guan X, Wu P, Wang X, Zhou L, et al. (2020) Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med 382: 1199-1207.
-
CDC COVID Data Tracker (2019) United States COVID-19 Cases and Deaths by State. CDC.
-
Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020) A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 382(8): 727-733.
-
WHO (2020) Novel Coronavirus-Japan (ex-China).
-
Edward H (2020) Novel 2019 Coronavirus Genome. Virological.org.
-
Fehr AR, Channappanavar R, Perlman S (2017) Middle East respiratory syndrome: emergence of a pathogenic human coronavirus. Annu Rev Med 68: 387-399.
-
WHO (2020) Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV).
-
Zhou P, Yang XL, Wang, XG, Hu B, Zhang L, et al. (2020) Discovery of a novel coronavirus associated with the recent pneumonia outbreak in humans and its potential bat origin. bioRxiv, pp: 1-18.
-
Li T, Wei C, Li W, Hongwei F, Shi J (2020) Beijing Union Medical College Hospital on “pneumonia of novel coronavirus infection” diagnosis and treatment proposal (V2.0) Med J Peking Union Med Coll Hosp.
-
Medical expert group of Tongji hospital (2020) Quick guide to the diagnosis and treatment of pneumonia for novel coronavirus infections (3 Edn.), Herald Med.
-
Liu T, Hu J, Kang M, Lin L, Zhong H, et al. (2020) Transmission dynamics of 2019 novel coronavirus (2019-nCoV). bioRxiv, pp: 1-27.
-
Huang C, Wang Y, Li X, Ren L, Jianping Z, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497- 506.
-
Gralinski LE, Menachery VD (2020) Return of the coronavirus: 2019-nCoV. Viruses 12(2): 135.
-
Wang C, Wang X (2020) Prevalence, nosocomial infection and psychological prevention of novel coronavirus infection. Chin General Pract Nurs 18: 2-3.
-
(2020) National Health Commission of People’s Republic of China. Prevent guideline of 2019-nCoV.
-
Perlman S, Lane TE, Buchmeier MJ (2000) In “Coronaviruses: Hepatitis, Peritonitis and Central Nervous System Disease. Cunningham MW, et al. (Eds.), Chap. 21, Lippincott-Williams and Wilkins, Philadelphia, pp: 331-348.
-
Sanchez CM, Izeta A, Sanchez MJM, Alonso S, Sola I (1999) Targeted recombination demonstrates that the spike gene of transmissible gastroenteritis coronavirus is a determinant of its enteric tropism and virulence. J Virol 73(9): 7607-7618.
-
Phillips JJ, Chua MM, Lavi E, Weiss SR (1999) Pathogenesis of chimeric MHV-4/MHV-A59 recombinant viruses: The murine coronavirus spike protein is a major determinant of neurovirulence. J Virol 73: 7752-7760.
-
Kuo L, Godeke GJ, Raamsman MJB, Masters PS, Rottier PJM (2000) Retargeting of coronavirus by substitution of the spike glycoprotein ectodomain: Crossing the host cell species barrier. J Virol 74(3): 1393-1406.
-
Dveksler GS (1994) Specificity of coronavirus/ receptor interactions. In “Cell Receptors for Animal Viruses. Wimmer E (Eds.), Cold Spring Harbor Laboratory Press, Cold Spring Harbor, NY, pp: 403-443.
-
Dveksler GS, Pensiero MN, Dieffenbach CW, Cardellichio CB, Basole AA, et al. (1993) Mouse hepatitis virus strain A59 and blocking antireceptor monoclonal antibody bind to the N-terminal domain of cellular receptor. Proc Natl Acad Sci 90(5): 1716-1720.
-
Gallagher TM, Escarmis C, Buchmeier MJ (1991) Alteration of the pH dependence of coronavirus-induced cell fusion: Effect of mutations in the spike glycoprotein. J Virol 65(4): 1916-1928.
-
Wang FI, Fleming JO, Lai MMC (1992) Sequence analysis of the spike protein gene of murine coronavirus variants: Study of genetic sites affecting neuropathogenicity. Virology 186(2):742-749.
-
Fazakerley JK, Parker SE, Bloom F, Buchmeier MJ (1992) The V5A13.1 envelope glycoprotein deletion mutant of mouse hepatitis virus type 4 is neuroattenuated by its reduced rate of spread in the central nervous system. Virology 187(1): 178-188.
-
Pearce BD, Hobbs MV, McGraw TS, Buchmeier MJ (1994) Cytokine induction during T cell mediated clearance of mouse hepatitis virus from neurons in vivo. J Virol 68(9): 5483-5495.
-
Godfraind C, Havaux N, Holmes KV, Couteleir JP (1997) Role of virus receptor-bearing endothelial cells of the blood–brain barrier in preventing the spread of mouse hepatitis virus-A59 into the central nervous system. J Neurovirol 3: 428-434.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future