Impromptu Innovation to Maintain Childhood Immunization during the COVID-19 Pandemic, in Trinidad a Small Developing Country in the Caribbean
Introduction: The interventional strategies introduced by the Government of the Republic of Trinidad & Tobago in an effort to mitigate the impact of the COVID-19 pandemic are likely to act as barriers to vaccination of children, potentially resulting in reduced uptake of vaccines to 2020 birth cohorts. Monitoring and taking steps to maintain vaccine coverage during these critically times are important. Methods: Using a randomly selected site we identified all eligible babies required to start their vaccination course. Using a cohort design these babies were followed during the three month period March-May 2020 during at the peak of the pandemic with lockdown and other public measures in place. All babies registered to start vaccination were monitored and those who actually received as well as those who did not receive their schedule vaccine were recorded. Results: Over the period January-May 2020, there were 318 live births recorded in the area covered by the PCF and these babies were subsequently registered in the CHC. A total of 259 children had at least one dose of IVP and DTwP-Hep-B-Hib at six weeks resulting in a mean vaccine uptake of 83% with a range of 83% - 71%. Although vaccine uptake decreased from 83.1% in January to 74.1% in April, the difference was not significant (ï£2, p = 0.09). Additionally, of those children who were given scheduled appointments for the second dose of the vaccine in two months, 197 of 209 (94.3%) returned and received the second dose. Conclusion: The outbreak of COVID-19 in Trinidad, together with the introduction of public health measures to prevent its transmission in March 2020 had no significant impact on vaccine coverage (VC) which ranged from 83.1% - 71.4% during the period. This was due to health care providers taking impromptu measures to maintain childhood immunization, including but not being limited to, counselling mothers on the importance and safety of the immunization process and ensuring that all public health measures would be maintained. Furthermore, mothers were given exact appointment times, and contacted prior to their appointments to reinforce these messages, and to reassure the mothers about the safety of the process.
Introduction
COVID-19 is the term used for the clinical disease caused by the novel coronavirus SARS-CoV-2, first identified in the city of Wuhan, Hubei Province, China [1]. On March 11, 2020 the World Health Organization (WHO) declared COVID-19 a pandemic [2]. The rapid spread (determined by its basic reproduction number, estimated at the beginning of the epidemic as a value of 2.38 (95% CI: 2.04-2.77) [3], has impacted severely on the demand for health care services, mainly due to the high rates of hospitalizations and deaths among a population naïve to the virus, as well as the unavailability of a vaccine or specific efficacious antiviral agents against SARS-CoV-2. On March 14 (?) the Government of the Republic of Trinidad and Tobago (TTO) introduced population-level movement restrictions, physical distancing and stay-at-home orders, following the first reported case on March 12, 2020. These measures aimed at limiting movement outside the home to essential activities such as, the procurement of food, health, pharmaceutical services, banking and petrol supplies. In addition closing borders, reducing seating to half in public transport vehicles, and closure of non-essential businesses such as bars, barbering shops and churches were also introduced. On the other hand such measures as building capacities for testing and diagnosis, isolation, contact tracing and quarantine were faced with challenges [4]. All these measures are likely to act as barriers to vaccination of children resulting in reduced uptake of vaccines to 2020 birth cohorts, initiate catch-up campaigns with older cohorts and deliver immunisations to at-risk groups. This situation is further aggravated by vaccine hesitancy. In 2019, the World Health Organization (WHO) designated vaccine hesitancy as 1 of the 10 leading threats to global health [5]. Given these developments it seems reasonable to expect declines in accessing child health services. In fact parental concerns about potentially exposing their children to COVID-19 during well child visits have impacted on childhood immunization uptake in the USA [6, 7]. On the other hand vaccines are expected to avert over 23 million deaths between 2011 and 2020 [8] and is an important contributor the sustainable development Goal for health [9]. Hence it is important to monitor vaccine uptake, both at the macro- administrative level as well as the micro- neighbourhood level. Such vaccine coverage surveillance, as well as modelling [7], can inform crisis improvisation and innovation. Although resource scarcity risks undermining services it may stimulate improvisation as healthcare professionals try to maintain services in circumstances where providing normal standards of care is impossible. In these circumstances, improvisation relates to dealing with unforeseen events without the benefit of preparation through concurrent thought, planning and action, drawing on available resources and creating the potential for incremental innovation [10].
The aim of this study is to assess child immunization practices as articulated in the Pink Book [11] during the COVID-19 pandemic at the micro-level in a small developing country. All five categories will be assessed: i) availability of vaccines, ii) assessment of immunization status, iii) effective communication about vaccine benefits and risks, iv) proper storage and administration of vaccines and v) documentation of vaccinations and implementation of strategies to maintain vaccination coverage.
Methods
Health care is delivered in Trinidad through four Regional Health Authorities (RHA) appointed by the Ministry of Health. In Trinidad there is universal health coverage in which all health care services delivered including vaccination are without cost to the client. We used a cohort study design in which all babies born in 2020 were admitted and followed until May 31 2020. A multi stage random process was used to select a Primary Care Facility (PCF) in one of the four RHA serving an estimated population of 33 000. Immunization services are provided by networking this PCF with a tertiary care centre. Women with uncomplicated pregnancies are admitted and followed in maternal and child health clinics (MCH) at the PCF to 36 weeks gestation, thereafter they are referred to a tertiary centre for delivery, unless there is an indication for earlier specialist obstetric referral. After delivery mother and baby return to the PCF for postnatal care and child health care (CHC) which includes mainly immunization and growth monitoring. All immunization records are permanently stored in a register as well as the child’s medical records and the parent is also given a vaccination record card to be used for registration at school entry, as a history of full immunization is a prerequisite by law for school entry. Hence the data is readily available and reliable.
Vaccine coverage (VC) is the traditional metric used to assess vaccine usage. For the purposes of this study VC is defined as the proportion of individuals eligible for vaccination and has received it. The denominator is the number of children referred to the PCF and registered in the clinic and the numerator is the number of children who were actually vaccinated. Calculating intervals between doses, 4 weeks = 28 days, intervals of ≥4 months are determined by calendar months. The schedule of vaccination consists of polio (IVP first 2 doses/ subsequent doses OPV) delivered as a 5-dose series at 2, 4, 6, 15-18 months and the pentavalent vaccine diphtheria, tetanus, pertussis (whole cell), Haemophilus influenzae type b, and Hepatitis-B (DTwP- Hep-B-Hib) delivered at a minimum age of 6 weeks, and administered by 3-doses at 2,4,12-15 months [12]. A two- tailed chi squared (χ2) test was used to test the difference between proportions with a significance level of p < 0.05.
Results
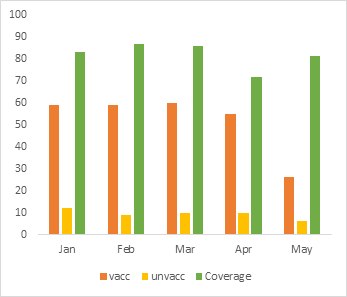
Over the period January-May 2020, there were 318 live births recorded in the area covered by the PCF and these babies were subsequently registered in the CHC. A total of 259 children had at least one dose of IVP and DTwP-Hep- B-Hib at six weeks resulting in a mean vaccine uptake of 83% with a range of 83-71%, (Table 1). Although vaccine uptake decreased from 83.1% in January to 74.1% in April the difference was not significant (χ2, p = 0.09). In addition of those children who were given schedule appointments for the second dose of the vaccine in two months, 197 of 209 (94.3%) returned and received the second dose. The first case of COVID-19 in Trinidad was reported on the 12 March 2020, and public health measures implemented on March 14, 2020. However there was no immediate impact on vaccination coverage in March or April 2020 (Figure 1 & Table 1).
| Births(n) | Vacc (n,%) | Unvac (n,%) | Coverage | |
|---|---|---|---|---|
| Jan | 71 | 59(83.1) | 12(16.9) | 83.1 |
| Feb | 68 | 59(86.8) | 9(13.2) | 86.8 |
| Mar | 70 | 60(85.7) | 10(14.3) | 85.7 |
| Apr | 77 | 55(71.4) | 10(28.6) | 71.4 |
| May | 32 | 26(81.3) | 6(18.7) | 81.3 |
| Total | 318 | 259(81.4) | 47(14.8) | 81.5 |
Table 1: Number Babies Admitted to CHC Over the Period January 2020 to May 2020, The Number Vaccinated (Vacc) and Unvaccinated (U
Discussion
Timely and accurate measurement of VC is required to evaluate the success of vaccine programmes as well providing a better understanding of unvaccinated groups such that novel approaches could be developed. Hence the major finding of this study is VC was sustained during the months in which COVID-19 threatened. It provides evidence that the outbreak of COVID-19 in Trinidad together with the introduction of public health measures to prevent its transmission in March 2020 had no significant impact on VC which ranged from 83.1-71.4 % during the period. This finding is consistent with reported vaccine coverage rates for Trinidad reported by WHO [13]. Maintaining VC during the COVID-19 pandemic sustains the gains made in the past such as the prevention of the spread of vaccine-preventable diseases, increase in life expectancy, and reduction health care costs. This is against a background in which the COVID-19 pandemic is expected to impact children adversely, jeopardising child welfare gains, and causing a global economic crisis in which children will be the prime casualties [14]. Preparing for population level health threats, such as infectious disease outbreaks, requires sustained in- vestments in certain public health functions, including preventive interventions (ex: immunization programmes, food and waterborne disease control measures), physical infrastructure (ex: laboratory and surveillance capabilities), trained personnel (ex: health professionals, epidemiologists) [15, 16, 17], and ongoing commitments to resources for supplies, maintenance, and training [18].
Notwithstanding VC rates must be interpreted with caution, as overestimation or under estimation can have serious adverse consequences on health and resources. In 2009 in Burkina Faso the reported VC for measles was reported as exceeding 95%, yet there was a large measles outbreak which killed 367 and affected over 54 000 individuals, mostly unvaccinated children [15]. Conversely, in London in 2013, MMR coverage among 10-16 year olds was estimated to be 61% [16], yet no large outbreaks occurred, but the same study suggested that up to 60% of London children aged 10-16 with no MMR vaccine record were in fact vaccinated, suggesting the low coverage was at least partly caused by inaccurate data. In fact many who were targeted in a MMR catch-up campaign the same year were already immune. Further the WHO-UNICEF-Lancet Commission emphasises that “what is good for children is good for societies: investment in children’s wellbeing provides benefits that are immediate, long term, and intergenerational” [17].
This achievement must be credited to impromptu innovation. Confronted with the challenge to convince mothers it was safe to bring their babies to the CHC, health care providers first counselled mothers on the importance and safety of the immunization process, emphasizing that all public health measures will be maintained. All mothers were given exact appointment times, so as to avoid overcrowding. In addition a contact telephone number was requested from each client, which was stored in the register. As the date of the appointment approached each mother was contacted and all messages were reinforced. Urgency and resource scarcity during crises may contribute to the generation of new innovations, whose implementation, over time, may lead to substantial improvements in health and social care systems. By and large, providers choose how to solve an issue, which encourages creativity and allows for a “test and learn” mentality that is necessary for innovation. Covid-19 is the quintessential example of the way that public health interventions can extend the reach and efficiency of our existing health care system. These findings suggest that driven by necessity, we observed a type of flexibility, acceptance and tolerance for creative solutions even though imperfect or untested [19, 20].
There are several limitations to the study. Although the PCF selected had a total sample size of over 30 000 no data was available of the number of women of childbearing age. We were unable to determine whether those children who remained unvaccinated were as a result of parents who are of antivaccine thinking and vaccination hesitancy which can directly impact on vaccine coverage. Notwithstanding existing immunization laws mandate vaccination before school entry, hence unvaccinated children may be attribute to intentional delay of vaccine administration. Strength of our study is cellular telephone services are inexpensive and easily available hence all mothers in the study had access to a cellular phone. Currently it is estimated that approximately 60 000 Venezuelan refugees are living in Trinidad who have free access to the MCH services, however we were unable to separate this group into a specific category. In conclusion this was an opportunity to implement an unprecedented public health measure, although a small-scale innovation, sharing the experience across a global platform, to encourage diffusion is important [21].
Declaration
We declare no conflict of interest or financial support for this work. The manuscript has been read and approved by all named authors, and we confirm the order of authors listed in the manuscript.
References
-
Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020) A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 382: 727-733.
-
WHO (2020) WHO Director-General’s opening remarks at the media briefing on COVID-19, World Health Organization.
-
Li R, Pei S, Chen B, Song Y, Zhang T, et al. (2020) Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). Science 368(6490): 489-493.
-
WHO (2020) COVID-19 strategy update, World Health Organization.
-
WHO (2019) Ten threats to global health in 2019. World Health Organization.
-
Hoffman J (2020) Vaccine rates drop dangerously as parents avoid doctor’s visits. New York Times.
-
Santoli JM, Megan CL, Malini BD, Elyse OK, Matthew FD, et al. (2020) Effects of the COVID-19 pandemic on routine pediatric vaccine ordering and administration- United States, 2020. MMWR Morb Mortal Wkly Rep 69(19): 591-593.
-
CDC (2015) The Global Impact of Vaccines in Reducing Vaccine-Preventable Disease Morbidity and Mortality. Center for Disease Control and Prevention.
-
WHO (2016) WHO’s mission and vision in immunization and vaccines 2015-2030. World Health Organization.
-
Hadida AL, Tarvainen W, Rose J (2015) Organizational improvisation: a consolidating review and framework. International Journal of Management Reviews 17(4): 437-459.
-
Adam B, Jennifer H, Tom S (2020) Immunization strategies for Health Care Practices and Providers. The Pink Book, Epidemiology and Prevention of Vaccine Preventable Diseases, Chapter 3.
-
Kidd S, Ouedraogo B, Kambire C, Kambou JL, Huong M, et al. (2012) Measles outbreak in Burkina Faso, 2009: a case-control study to determine risk factors and estimate vaccine effectiveness. Vaccine 30(33): 5000-5008.
-
WHO (2019) Global Vaccine Action Plan. 2019 Regional Reports on Progress towards GVAP-RVAP Goals. Annex to the GVAP review and lessons learned report, World Health Organization.
-
(2020) Policy brief: the impact of COVID-19 on children. United Nations.
-
Carafano JJ, Florance C, Kaniewski D (2015) The Ebola outbreak of 2013-2014: An assessment of U.S. Actions. Special Report of the Heritage Foundation, pp: 166: 1-48.
-
Gates B (2015) The next epidemic-Lessons from Ebola. N Engl J Med 372: 1381-1384.
-
Heymann DL, Chen L, Takemi K, Fidler DP, Tappero JW, et al. (2015) Global health security: The wider lessons from the west African Ebola virus disease epidemic. Lancet 385(9980): 1884-1901.
-
Katz R, Seifman R (2016) Opportunities to finance pandemic preparedness. Lancet Glob Health 4(11): e782-e783.
-
Kidd S, Ouedraogo B, Kambire C, Kambou JL, Huong M, et al. (2012) Measles outbreak in Burkina Faso, 2009: a case-control study to determine risk factors and estimate vaccine effectiveness. Vaccine 30(33): 5000- 5008.
-
Simone B, Balasegaram S, Gobin M, Charlotte A, Andre C, et al. (2014) Evaluation of the measles, mumps and rubella vaccination catch-up campaign in England in 2013. Vaccine 32(36): 4681-4688.
-
Clark H, Coll Seck AM, Banerjee A, Stefan P, Sarah LD, et al. (2020) A future for the world’s children? A WHO- UNICEF-Lancet Commission. Lancet 395(10224): 605- 658.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future